
Juanita H. Williams
Psychology of Women
Behavior in a Biosocial Context
1. Myths, stereotypes, and the psychology of women
Woman as enchantress-seductress
From Myth to Stereotype: The Virtuous Woman
The Psychology of Women: Philosophical Origins
A minor theme: the argument for equality
The Psychology of Women: Science and Social Values
On Understanding Women: Contributing Sources
2. Psychoanalysis and the woman question
The early development of psychoanalysis
Freud’s theory of female development
Psychoanalytic research and psychotherapy
Epilogue: Emma Eckstein and the seduction theory
Narcissism, passivity, and masochism
Sexuality and the feminine role
Psychosocial development: the “eight ages of man”
Sex differences and the use of space
3. Woman and milieu: innovative views
4. Sexual dimorphism, biology, and behavior
Determinants of Sexual Differentiation
The animal model: experimental studies
Puberty: Physical and Hormonal Changes
Menarche and the Menstrual Cycle
Dysfunctions Associated with the Menstrual Cycle
Behavior and the Menstrual Cycle
Why Do Women Live Longer Than Men?
Sociobiology: The New Biological Determinism
5. The emergence of gender differences
Social class and cognitive development
Determinants of gender differences
What Do We Know about Gender Differences?
Cognitive-developmental theory
Development of Gender-Role Identification
Parental Identification in Adolescent Girls
The Daughter-Parent Relationship
The mother-daughter relationship
The father-daughter relationship
Sex Typing and Socialization Experiences
The Menarche: Socialization Effects
Achievement: Conflict and Resolution
Other Influences on Achievement
The Development of Competence in Girls
Moral Development: In a Different Voice?
Women and Sexuality: Historical Perspective
Only Yesterday: The Victorian Context
Etiology of Sexual Dysfunction
Treatment of Sexual Dysfunction
Social Values and Birth Control
The Billings method: “natural birth control”
Teenagers, Sex, and Birth Control
Abortion: The Continuing Controversy
Birth Control and Public Policy: The China Example
Birth Control: A Woman’s Right
Motivations for Having Children
Cross-cultural attitudes and practices
Alternative experiences in childbirth
Psychological Aspects of Pregnancy
Relationship with one’s mother
The Postpartum Period: Mother-Infant Bonding
The Postpartum Period: Reactions and Adaptations
10. Women’s lives: tradition and change
Women’s careers: “Dream vs. Drift”
Black Women: The Minority Experience
Lesbianism in History and Culture
“Romantic friendship”: bonding in a female world
Lesbianism and the Medical Model
“Once We Were Sick and Now We Are Well”: The Shift in Perspective
Dimensions of Lesbian Experience
12. Psyche and society: women in conflict
Early Life Adaptation of Girls
Woman as Victims: Violence and Intimidation
Mental and Emotional Disorders of Women
Social Roles and Mental Disorders
The Double Standard for Mental Health
[Front Matter]
Juanita H. Williams is also the editor of
Psychology of Women: Selected Readings
Second Edition
[Title Page]
Psychology
of Women
Behavior
in a biosocial
context
Third Edition
Juanita H. Williams
Professor of Psychology and Women’s Studies
University of South Florida
W • W • NORTON & COMPANY
New York • London
[Copyright]
Copyright © 1987, 1983, 1977, 1974 by Juanita H. Williams
All rights reserved.
Printed in the United States of America
First Edition
Library of Congress Cataloging-in-Publication Data
Williams, Juanita H., 1922-
Psychology of women.
Bibliography: p. 507
Includes index.
1. Women—Psychology. 2. Women—Physiology.
3. Women—Sexual behavior. I. Title.
HQ1206.W72 1987 155.6’33 86–21655
ISBN 0-393-95567-2
W. W. Norton & Company, Inc., 500 Fifth Avenue, New York, N.Y 10110
W. W. Norton & Company Ltd., 37 Great Russell Street, London WC1B 3NU
1 2 3 4 5 6 7 8 9 0
[Dedication]
To my mother,
Anna Bryant Hingst,
with love
and appreciation
Preface
The psychology of women is now established as a discipline, and most colleges and universities have courses focusing on the female experience. Since the first edition of this text in 1977, scholarly work in the area has flourished and today finds the interest and involvement of researchers even stronger. The rapid growth of the field with its many new discoveries makes this third edition necessary. As before, the text is organized on a life cycle perspective that emphasizes critical patterns of events that are likely to be experienced by most women. Much new content has been added. A full chapter (11) on lesbian identity, including the tradition in culture as well as the earlier medical model and the contemporary research-based perspective that has replaced it, informs students of the important issues. A major section, in chapter 10, on the black female experience adds balance to discussion of the psychology of women. In addition, references to research on black girls and women appear in other relevant contexts.
The early chapters that provide the historical setting for the work now include the new controversy over Freud’s seduction theory, and the work of Leta Hollingworth, an early twentieth-century psychologist whose research portended some of today’s issues. New topics include research on why women live longer, a critique of sociobiology, and updated material on gender differences. Carol Gilligan’s work on women’s moral development is reviewed, along with teenage sexuality and birth control, an expanded treatment of abortion, and China’s one-child policy and its effect on women. Also new is the “dream vs. drift” conflict in women’s career decisions, the “having it all” syndrome, and a full new section on pornography and the controversy within feminist circles as women struggle with issues of morality and repression. The incorporation of DSM III permits the latest examination of gender differences in mental disorders, suicide, and eating disorders with analysis of some of the factors that underlie these differences. More positive attitudes coming from research on aging are presented. All chapters have been brought up to date by inclusion of the latest research and theory in the field.
This edition continues to reflect the underlying perspective that the behavior of women occurs in a biosocial context and can only be understood within that context. While women have in common certain biological experiences, they live in drastically different social settings under varying moral codes and conditions of life. No understanding of the psychology of women is possible without taking into account this social context with its permissions and prohibitions. Further, the psychology of women cuts across all the subdisciplines in psychology; it looks at the whole spectrum of behavior as it is shaped from all its sources: the personal, the social, and the biological.
Most of the recent research on the psychology of women has been done by women, an observation reminiscent of John Stuart Mill’s prophetic comment in Subjection of Women over a hundred years ago that no understanding of women would ever be possible until women themselves began to tell what they know. The authenticity of women’s knowledge about themselves and of the kinds of questions that science can ask about them is now recognized by women and men alike. We are assuming more instrumental and authoritative roles in seeking out the answers.
It is now fifteen years since I began teaching courses on the psychology of women. My students continue to inspire me, and I want to thank them again for their interest and enthusiasm. I would also like to thank Marian Johnson at Norton for her careful attention to detail as she edited the new copy. My editor, Don Fusting, has worked with me on all three editions of this book, and his knowledgeable assistance and concern with quality have helped to make each one better than the last.
Once again I appreciate my husband Jim’s support (especially his culinary skills) during my days at the typewriter, and the unfailing interest and curiosity of my daughters, Karen, Anita, Gretchen, and Laura.
J. H. W.
Tampa, 1986
1. Myths, stereotypes, and the psychology of women
It is always difficult to describe a myth; it cannot be grasped ar encompassed; it haunts the human consciousness without ever appearing before it in fixed farm. The myth is so various, so contradictory, that at first its unity is not discerned.... [W]oman is at once Eve and the Virgin Mary. She is an idol, a servant, the source of life, a power of darkness; she is the elemental silence of truth, she is artifice, gossip, and falsehood; she is healing presence and sorceress; she is man’s prey, his downfall, she is everything that he is not and that he longs for, his negation and his raison d’etre.
—Simone de Beauvoir, The Second Sex, 1953
Mythic Woman
Over the millennia women have been variously observed and understood, and the derived wisdom recorded in literature, art, and religion for the enlightenment of all. Mostly, understandings of women have taken the form of strongly held beliefs which served to validate and to order experience, or have emanated from such authoritative sources that few would question them. Thus women have been seen as incarnations of both the highest good and the basest evil, of chastity and of lust, of virtue and deceit, and of the sacred and the profane. Men, and women who are co-opted by the prevalent male view, have rarely been able to perceive women simply as human beings with the same range of idiosyncracies as themselves. Rather, they have had to make myths to explain their awesome differences and their strange powers. Occasionally, in time of great stress, when women’s brains, hands, and backs are needed to win a war or tame a frontier, they are seen for a while as simply human— though with certain disabilities, to be sure. But myths do not swirl about the form of the grandmother who matter-of-factly digs a trench for the children to sleep in, nor does a mystique lie about the woman who guides a plow and mule down the rows of some remote farm newly developed from the wilderness.
Aside from such unusual exigencies, however, man has always felt the need to explain and to codify woman, to come to terms with her presence on earth and to accommodate her within his rational system. As he made myths to explain other phenomena of the universe, so he devised explanations of the phenomenon woman which expressed significant truths about her, and images such as old maid or virgin that bring to mind the essential features thought to characterize all persons so called. Such beliefs are ways of knowing; they predate but continue to exist alongside the attempts of science to explain human behavior. The tenacity and continuity of these beliefs in different eras and cultures must mean that they serve potent needs in the human experience.
In addition to their explanatory power, myths also provide man with the hope that he can control the frightening and inexplicable phenomena with which they deal. For example, he sees that a natural event like a prolonged drought threatens his existence. If his mythology includes a responsible god who expresses his displeasure by visiting him with droughts, and who can be placated with gifts, then he can end the drought by making sacrifices to that god. Thus he perceives that he has a measure of control over his own destiny. If the procreative and sexual powers of women awe and frighten him, he can hedge them about with taboos, confine them to special places, or devise elaborate rituals whereby he can deal with the mythic female power. Myths thus introduce a semblance of understanding and order into the apparent chaos of the universe.
Myths about the powers, motives, and special qualities of women have been reflected in the literature and religion of most cultures from earliest times. Although they occur in myriad forms, certain themes have been observed to be universal, and to have continuity with the present. They have been analyzed in detail elsewhere (e.g., Campbell, 1959; de Beauvoir, 1953; Diner, 1973; Figes, 1970; Janeway, 1971). After briefly describing a few of these myths, we shall look at one of them more closely because of its relevance to contemporary ideas about women.
Woman as mother nature
The analogy between woman and the earth as sources of life has always inspired the myths and poems of men and caused them to create their earliest religions and figures of worship. Myths of the Great Mother were part of all the cultures that contributed to the stream of Western civilization. Whether she was called Demeter, Isis, Ishtar, or golden Aphrodite—the goddess of a hundred names—she was the mother and nurturer of both gods and men (Diner, 1973).
A curious reciprocity pervades the mythic concepts of woman and nature. The fecundity of nature, earth bringing forth fruit and grain, sea and river yielding their fishes, all are symbolized by woman. The French author Simone de Beauvoir, tells how an Indian prophet warned his disciples against spading the earth, because it is a sin “to tear the mother of us all in the labors of cultivation” (1953, p. 145). The reciprocity lies in the reversal of these images in the assimilation of nature’s forms to woman. One could find hundreds of examples of comparisons of woman and her various parts to the flora and fauna of nature. Surely one of the most beautiful of these is in the Old Testament Song of Solomon:
Thy belly is like an heap of wheat, set about with lilies ...
This thy stature is like to a palm tree, and thy breasts to clusters of grapes (Solomon 7: 2,7).
The identification of nature with woman and the description of woman in terms of nature suggests an affinity between the two. Man could reside and make his mark, could observe and comment, but it was woman who linked him to earth. “Literally woman is Isis, fecund nature. She is the river and the riverbed, the root and the rose, the earth and the cherry tree, the vine-stock and the grape” (de Beauvoir, 1953, p. 145). She was closer to the mysterious scheme of things, to the heart of the matter, than he was. Did not her very body share with the moon its periodicity, and with the earth its power of generation? Thus she was part of that nature which he could not control, which could destroy him with her capricious whims. To effect a separation of the mortal woman from the identity he feared she had with that power, he had to neutralize her magic by setting up systems which would protect him and would give him some control over the unspeakable contingencies emanating from that identity: “That is why she is never left to Nature, but is surrounded by taboos, purified by rites, placed in charge of priests; man is adjured never to approach her in her primitive nakedness, but through ceremonials and sacraments, which draw her away from the earth” (de Beauvoir, 1953, p. 169).
Woman as enchantress-seductress
Myths of the woman who enchants man with her magic charms and seduces him away from the high paths of his holy mission are as old as communication and as persistent as the sex drive itself. On one level, they are stories, simple or epic, about man rendered powerless, having no choice but to surrender to her who has only the frail weapons of her body and her eyes, and, of course, her special connections with potent forces in those occult dimensions which defy the rational mind. On another level, they represent his projections upon her of his own worst fears about himself, of that dark part of his nature with which he constantly struggles, that part most resistant to being tamed into the service of his higher being. Thus for the statement “Against my better judgment I did something that was very bad,” he substitutes, “She bewitched me, and caused me to do something which I would otherwise never have done.”
Mythic enchantresses, bent upon diverting man from his noble tasks, causing him to abandon reason, and eliciting his essential wickedness, which he had repressed with such pain, are part of our earliest chronicles. The common motif in such accounts is that woman, otherwise powerless, gets what she wants by using devious, cunning means in which her sexual attraction is a strong element to effect the downfall of her prey, man (Figes, 1970). Odysseus, for example, was delayed in his attempt to return home from the Trojan War by the goddess Circe, who, having turned his men into swine, seduced him and kept him on her island for a full year.
Sometimes the fear of being emasculated is brought out in masked form in stories where women cause men to lose their strength, to become like women. Such a woman was lole who feminized the mighty Hercules in an account by Boccaccio. To get even with him for killing her father and carrying her off, she pretended to love him. “With caresses and a certain artful wantonness,” she made him desire her so much that he could deny her nothing. Once he was in this state, she had him take off his lion skin and lay aside his club and quiver of arrows. Defenseless, he submitted to having his beard combed and his body anointed with oils. Adorned with garlands and clad in a purple robe, he came finally to such a pass that he would sit among the women and spin wool. The deceitful lole had more surely destroyed him than if she had used a knife or poison (Figes, 1970).
Other members of the sisterhood who were invested with the myth were the witch and the prostitute. That vision of women which caused millions of them to be tortured and put to death between the fifteenth and eighteenth centuries was presented most vividly by Jacob Sprenger, a fifteenth-century Dominican and a witchcraft inquisitor. In the Malleus Maleficarum—“hammer of witches”—he set forth the doctrine that large numbers of women were in unholy alliance with Satan, and were a horrible threat to man, particularly to his genitals. The worst vice of these women was their insatiable lust, which led them to copulate with the Devil and become his intermediary, working his mischief on the body of man. This idea persisted in less virulent form in later ministerial invocations against the prostitute. She aroused men like Henry Ward Beecher, the famed nineteenth-century American preacher, to passionate rhetoric: “What horrid wizard hath put the world under a spell and charm, that words from the lips of a STRANGE WOMAN shall ring upon the ears like tones of music.... [F]rom the lips of the harlot words drop as honey and flow smoother than oil; her speech is fair, her laugh is merry as music.... [T]rust not thyself near the artful woman, armed in her beauty, her cunning raiment, her dimpled smiles, her sighs of sorrow, her look of love” (Walters, 1974, p. 70).
Woman as necessary evil
The perception of woman as necessary evil, as inferior, insignificant nonperson who is barely tolerated for the services she performs, is true misogyny. Necessary to perform the functions of sex object and child bearer, she is otherwise unimportant, rightfully excluded from the company and affairs of men. While the fortunes of women have varied in different societies at different times, it is a universal observation that men have held women to be lesser persons than themselves and have ascribed to them an inferior status (Bullough, 1973). A very early example is Hesiod’s eighth century b.c. account of Pandora, the Greeks’ version of the first woman. Pandora came to the first man as a gift from the gods, who had given her a box never to be opened. All too mortal, she could not contain her curiosity and loosed all the evils and diseases which have plagued humans ever since. Hesiod pointed out that it was from her that all women descended, that troublesome tribe who brought man nothing but misery whether he married them or not. A wife was a constant financial drain who could not be trusted in any case. Without her, however, he would have no heirs and no one to nurse him in his old age.
During most of the history of Western civilization, women have been regarded basically as property, with no rights of their own. A strong tenet of Puritan belief, for example, was the requirement that women be kept in a subordinate position. The Puritan poet John Milton insisted on the inferiority of women and the need for men to guard their authority over them to keep them from foolish action. He expressed the not uncommon theme of woman as a kind of intrusive nuisance in man’s world in Paradise Lost, when he has Adam plaintively ask, after the Transgression, why God created “this novellie on earth, this fair defect,” instead of filling the world with men, or finding some other wax’ to generate mankind (Rogers, 1966). 1 his mythic perception of woman as necessary evil has persisted through the ages, and has survived the evolution of ideas and intellectual changes. As one of the earliest and most influential views of women, it has dominated not only religious teaching but philosophical thought as well. Schopenhauer, the nineteenth-century German philosopher, is only one example of a cohort of the period whose ideas about women ranged from patronizing to loathing. His essay On Women starts out with an innocuous tribute to woman’s contribution to man’s infancy, maturity, and old age, then gets on with his theme. Women are fitted to nurse and teach children because thev are themselves childish and frivolous—an intermediate stage between the child and the full-crown man. Nature lavishes beautv on the young female so that she can capture a man, who, bereft of reason, takes on the burden of her care forever. The fundamental fault of the female character is that she has no sense of justice, being defective in the powers of reasoning and deliberation. In compensation. Nature has caused her to excel in dissimulation, faithlessness, treachery, lying, ingratitude, and so on. Only the man whose sexual impulse has beclouded his reason would call her the fair sex, for she is in fact undersized, narrow-shouldered, broad-hipped, and short-legged. She looks upon everything as a means for conquering man. Thus, she has no genuine interest in any art. and no genius whatsoever.
We shall see later how such vindictiveness encountered a stifling effect with the ascendancy of another myth about women. Even so. the underlying hostility could continue to be vented toward such deviants as old maids—women whom no man had found desirable enough to marry—and feminists, who insisted upon violating the boundaries of woman’s place by demanding a role in the institutions which man had created. Ebe basic ideas of woman’s inferiority and unfitness to be man’s equal continue to be thematically important as determinants of attitudes toward her.
Woman as mystery
The seeming perversity of woman’s behavior, the wonderment she excited with her strange powers, the ways she was different from man gave rise to another myth, which was that her mental processes, her behavior, and the whole of what she was, made up a feminine essence which was beyond the power of philosopher, scientist, or any ordinary baffled male to understand, just as there were other natural phenomena which did not yield to reason or empirical science, so there was woman, with her unpredictable ways and her enigmatic face. This myth, in a way, is a supplement to all the others. Failing any other explanation, she can be viewed as a different order of being, to whom the laws and rules by which behavior and thought are normally understood do not apply.
Simone de Beauvoir in an analysis of the myth of feminine “mystery” pointed out its advantages. First, it permits an explanation which will fit all manner of events. Caprices, moodiness, strange excursions—-whatever about her man does not understand, he can attribute to that quality of hers he is sure of, her essential mysteriousness. Instead of admitting ignorance, he can relegate her to that category of events which are simply inexplicable. Second, he can protect himself from disturbing insights. If she changes in her affections, if she talks in riddles, the mystery explains it all. Last, and perhaps most important, it permits man to remain alone as the One who works, judges, and defines reality. She is the Other, and since he cannot understand her, he is exempt from the effort of building an authentic relationship with her. If he cannot understand her, she cannot be understood, and authenticity cannot occur in the absence of understanding. Thus even when he is with her he stands alone, in charge, an alternative to the admission and sharing of their common humanity (de Beauvoir, 1953).
Upon what basis could such a myth be founded and perpetuated? The mystery is in the inability of man and woman to communicate across the distance that separates her world from his. As de Beauvoir observed, humans are defined by their acts. When a woman is kept by a man, she is a passive recipient of the advantages he bestows upon her as long as he cares about her. But this role is not a vocation and does not bestow identity upon the woman. Her dependency causes her to dissemble, as all subordinates learn to dissemble with their masters, concealing their real thoughts and feelings under an enigmatic exterior. “And moreover, woman is taught from adolescence to lie to men, to scheme, to be wily. In speaking to them she wears an artificial expression on her face; she is cautious, hypocritical, play-acting” (de Beauvoir, 1953, p. 259).
By defining her as mysterious Other, man spares himself the necessity of analyzing her behavior and understanding it as a consequence of her position vis-à-vis him. To do that would require acknowledgement of her oppression, and a possible shift in their power relationship. The price would be very high.
Behavior theorists of modern times have had much to say about women, some of it helpful, some of it not, in furthering understanding. Freud was less sure than some of his followers that either he or the theories he developed had revealed the mystery. His biographer, Ernest Jones (1955), said that Freud found the psychology of women “more enigmatic” than that of men, and reported him as having asked a female colleague, “The great question that has never been answered and which 1 have not yet been able to answer, despite my thirty years of research into the feminine soul, is ‘What does a woman want?’ ” (p. 421). And in 1933, in his last paper on female psychology, he spoke of femininity as a riddle—to men but not to women, since they were considered the problem. If one wanted to know more about women, he said, one could ask of one’s own experiences, or turn to the poets, or wait for science to give the answers (Freud, 1965).
The influences and remnants of these mythic explanations for woman, as Mother Nature, as spellbinder, as necessary evil, and as mystery, are not difficult to find in the popular culture of today. There is another, however, which has probably had more influence on the lives of women in our society because it is perfectly in keeping with the ideal model for womanhood which has persisted until recent times. It is the myth of female goodness, of woman as the embodiment of virtue. This myth told women how they ought to be and described the rewards. From its beginning with the virtuous wife to today’s stereotypes of the feminine woman, this myth more than any of the others has defined woman’s place and her behavior in it.
From Myth to Stereotype: The Virtuous Woman
The model of the virtuous woman has occupied writers, priests, and moralists since earliest times. Throughout history there has been remarkable agreement on her characteristics. She is a faithful, loyal, and submissive wife; a dedicated, loving mother; a competent, diligent housewife; and an unquestioning supporter of the moral and religious values of her society. Although emphasis on the importance of each of these qualities has varied in different periods, the basic elements are nearly always discernible. Together they have defined her place. More than the definition of her physical setting, it has included the constellation of personal characteristics and permissible behaviors which distinguish her from the male and describe her status relative to his. As long as she observed her place and behaved in accordance with its prescriptions, no fault was found in her. In fact, during some periods she was so elevated that men were figuratively if not literally on their knees before her, overcome by the moral qualities of her being, so different from their own.
The Book of Proverbs contains an Old Testament description of what constituted goodness in women:
She riseth also while it is yet night, and giveth meat to her household, and a portion to her maidens.
She considereth a held, and buyeth it; with the fruit of her hands she planteth a vineyard ...
She layeth her hands to the spindle, and her hands hold the distaff ...
She stretcheth out her hand to the poor; yea, she reacheth forth her hands to the needy ...
She looketh well to the ways of her household, and eateth not the bread of idleness.
Her children rise up, and call her blessed; her husband also, and he praiseth her ... (Proverbs 31: 15–28).
This description of industry and household productivity was supplemented by the statements of early Christian writers on the proper role of women. Women were constantly admonished to obey their husbands. “Wives, submit yourselves unto your own husbands, as it is fit in the Lord” (Colossians 3: 18). St. Augustine, the fourthcentury Christian scholar, presented a model of motherhood in a reverential description of his mother, Monica. He praised her for putting up with his father, an unbeliever and adulterer, for praying for him, and above all for never chastising him or showing any temper. Monica had even instructed other women who complained about their husbands that they were bound by the marriage contract to serve, to remember their condition, and not to defy their masters (Figes, 1970).
The ultimate prototype of the model wife, however, was the patient Griselda, whose story was told by the celibate clerk in Chaucer’s Canterbury Tales of the fourteenth century. Griselda was a serf, whose noble husband had married her on the condition that she would be completely obedient to his every wish. To test her he had her two children taken away, saying that they must be put to death. She acquiesced graciously. He later told her that she must return to her father’s hovel, as he had decided to take a younger wife. She agreed to her unworthiness and cheerfully left, thus finally convincing him that she was indeed a good wife. Thereupon he returned her children and brought her back to be his wife. Griselda thanked him copiously, and said that she would die happy knowing that she had found favor in his sight.
During the Middle Ages, there arose the convention of romantic love, a passionate, despairing devotion directed toward an impeccable and unattainable (in theory) lady. Chivalry, the code prescribing that women should be given precedence by a gentle, courteous male, arose from this convention (Bullough, 1973). The man in love, usually a knight, minstrel, or noble, was in a state of total adoration, “in thrall,” indeed. Whether he was rewarded or not, the fact that he was in love had great positive value for him, making him more skillful and valiant at his pursuits, usually war or practice for it. The woman, though she herself was a passive recipient of his ardor, had ennobling qualities: she inspired in him courage, skill, and honor. While very few women benefited from this novel adulation, it marked the beginning of the tradition of courtly love, of the feminine mystique, and of the vision of woman on a pedestal which has been one line of approved wisdom ever since.
Rarely have women been idealized and worshiped with such unrelenting fervor as in the American South during the nineteenth century. This attitude spread to other parts of the country as well and was responsible with some modification for the prevalent view of woman during the nineteenth and the first half of the twentieth century.[1] Southern womanhood became a symbol for the Southern male, who imbued her with qualities of purity and goodness which had to be protected and defended against any hint of defilement or threat to her honor. The ideal woman was described in The Mind of the South as a combination of “lily-pure maid” and “hunting goddess”: “And she was the pitiful Mother of God. Merely to mention her was to send strong men into tears—or shouts. There was hardly a sermon that did not begin or end with tributes in her honor, hardly a brave speech that did not open and close with the clashing of shields and the flourishing of swords for her glory” (Cash, 1960, p. 89).
This romanticization of women was an important social motif in mid-nineteenth-century America, epitomized by the “cult of true womanhood” (Welter, 1973). The true woman, a Victorian adaptation of earlier models of the virtuous woman with strong Puritan and moralistic overtones, had four virtues: piety, purity, submissiveness, and domesticity. So identified, she was secure on her pedestal, and reverential paeans were sung in her honor. Her religious piety made her the moral arbiter of the home and the society; by her doing, souls would be saved; erring men, always more subject to temptation than she, would repent; and fallen women be brought to salvation. Purity meant chastity until the wedding night, an event to which she brought her greatest gift, her virginity. Girls were warned over and over again about the perils of sitting too close to males, of dancing, of inflaming the senses with novels, of listening to “the siren voices of vicious pleasure.” For “the sin against chastity was a graver, deeper sin, than any other; ... the white robe of innocence once soiled, could never again be restored to its former purity” (Brockett, 1869, pp. 213–17). In the sexual relationship, it was woman’s responsibility to set the pace and to keep a healthful balance. Physicians taught that women had little or no sex drive and responded to their husbands only to keep them from going to prostitutes. Woman’s lack of desire was nature’s way of taming man’s animal lusts, thus avoiding the drain on his vitality that too frequent or prolonged intercourse would have (Haller, 1974). This view of female sexuality contrasts remarkably with that of its counterpart, the seductress, who was invested with such insatiable appetite that man must be ever on his guard against her.
The third virtue, submissiveness, was the God-imposed role of good women, who deferred to their husbands in all things. The woman who questioned this, or took independent action, was a threat to the sacred order of the universe. It was mostly on this point that the antifeminist argument rested. The suffrage movement, for example, was seen as an assault against Christianity, the home, and the institutions of marriage and the family. The physician James Weir, Jr., in 1895, “proved” that the woman who advocated equality of the sexes had “either given evidence of masculo-feminity (viraginity), or had shown conclusively that she was a victim of psychosexual aberrancy” (Haller, 1974, p. 77). The view that submissiveness was natural and therefore good for women was supported in countless books and treatises which documented sex differences in brain and physique to support the point that woman was delicate, frail, and weak, and that too much intellectual or otherwise assertive activity would damage her health irreversibly (Bullough, 1973). It was common for the medical men of the time to assert that overexercise of the female brain in study would cause mania, sterility, and deterioration of health.
Finally, the true woman was revered for her domesticity. The care of the home and its occupants was her highest calling. To her family she was a comforter and a ministering angel. Gentle, patient, and merciful, she was a perfect nurse, teacher, and inculcator of values. She formed the mind of the infant, the holiest of tasks, and made it possible for the successful man to give her the ultimate accolade, “All that I am I owe to my sainted mother.”
The myth of female goodness, building as it did upon the belief in woman’s special nature and her moral character, was in fact for women a two-edged sword. On the one hand, it set her apart from the world in a small sphere of her own defined by rigid conventions and artificial pretensions. As long as she observed her place and her duties, she was the object of esteem and adoration, was “better,” in fact, than the male whose life was too rough and competitive to permit such refinement of taste and decorum. But this elevated status had very little material reward or prestige, other than that ascribed to her by her husband’s position. She had no legal or political power, very little personal freedom, and no way to achieve economic independence. But secure in her place, and venerated as she was, what need had she of these? Thus was she rewarded for her meekness and compliance, and told that she was too good and too delicate to participate in the affairs of men.[2] Women who refused to conform to this model, such as the feminists and other radicals, were castigated in pulpit and press as anarchists and perverts, as unnatural and morally defective.
Another major problem with the myth was that it conflicted with reality. Most Americans of the time still lived on farms, and women did not have the leisure or the means to cultivate the manners and life style of the proper female, as prescribed by the cult of true womanhood (Bullough, 1973). But while probably only a small minority of American women ever lived the myth in all its connotations, it was still the official style of being female and was promoted in the printed media and from the pulpit until recent times. In fact, the same rhetoric has recently reverberated through the land, in support of the arguments of those opposed to the Equal Rights Amendment. Opponents contend that women are a special class of being, and need special protection; not man’s equal, they are his superior. Those who demanded equality and liberation from the old shackles of role and place were rejecting their femininity. They were frustrated harridans or lesbians or both. The more things changed, it seemed, the more they remained the same.
The Psychology of Women: Philosophical Origins
The mythic models of women described above were constructed and maintained mostly in literature, religion, and the popular culture. While they have survived historically in the attitudes and beliefs of people of all statuses and walks of life, it is interesting in particular to note their presence in the thinking of many of the great philosophers of the Western intellectual tradition.
The reason for this is that psychology as a scientific discipline has its roots in philosophy, as well as in the natural sciences. For example, Aristotle, the great fourth-century b.c. Greek philosopher whose ideas about women we shall look at later, made contributions to both these branches of knowledge that are evident today in psychological assumptions and methodologies. These include the construction of a system of knowledge whereby the behavior of living organisms may be studied, both empirically and rationally; the assumption of the intimate relationship between the mind (“soul”) and the body; and the practice of recording and interpreting human behavior and experience in concrete terms. Psychology emerged as a separate discipline in the late nineteenth century as it adapted scientific methodology to the study of behavior and began to move closer to the natural sciences with their emphasis on measurement, experimentation, and control. The link with philosophy has remained strong, however, and manifests itself in modern times in the work of such psychologist-philosophers as, for example, William James (1890), John Dewey (1930), and Rollo May (1953).
For these reasons it is enlightening to look at the ways in which women have been conceptualized by our philosophical mentors. And the inescapable observation is that most of the best-known historical philosophers had a strong antiwoman bias that ranged from condescension to virulent misogyny:
Most famous philosophers made sexist remarks or formulated misogynist theories in their lesser-known writings. Now feminists have realized that these are not just incidental comments reflecting the assumptions of the time but integral parts of these philosophers’ larger theories which cannot be quietly expunged or passed over with a sigh (English, 1978, p. 825).
Philosophy is concerned with inquiry into principles of reality, such as human nature, human values, and so on. Analysis of many philosophers’ theories of “human” nature reveals, however, that “human” means “man” and that women are explicitly excluded on the grounds that they lack some essential human capacity possessed by males only, which relegates them, along with children and slaves, to an inferior category. Aristotle was very clear in his view that woman was to man as the slave to the master—that she was an unfinished man, being on a lower level of development. The male, he thought, was fitted to rule by reason of his natural superiority. Women were weak of will and incapable of independence; therefore, their best condition was a quiet home life.. the courage and justice of a man and of a woman are not, as Socrates maintained, the same; the courage of a man is shown in commanding, of a woman in obeying.... [A]s the poet says of women, Silence is a woman’s glory, but this is not equally the glory of man” (Bishop and Weinzweig, 1979, p. 46).
One of the greatest proponents of individual freedom was the French Enlightenment figure Jean Jacques Rousseau (1712—78). Believing that the maintenance of political liberties depended upon an educated populace, Rousseau set forth his ideas on education in Emile, a treatise describing the difference between males and females, their places in society, and how they should be trained for them. The emphasis for the boy is on freedom of intellectual expression, so that his mind may develop to its full power, fitting him to take his place in a democratic society. The girl, however, is to be prepared for a future when she will be totally dependent upon a man, “at the mercy of man’s judgment”:
A woman’s education must therefore be planned in relation to man. To be pleasing in his sight, to win his respect and love, to train him in childhood, to counsel and console, to make his life pleasant and happy, these are the duties of woman for all time, and this is what she should be taught while she is young.... What is most wanted in a woman is gentleness; formed to obey a creature so imperfect as man ... she should early learn to submit to injustice and to suffer the wrongs inflicted on her by her husband without complaint ... (Rousseau, 1979, pp. 365–67).
Rousseau also pronounced that girls should be trained to be docile, that it is more important to show a woman what to believe than to explain to her the reasons for belief: “Unable to judge for themselves, they should accept the judgment of father and husband as that of the church” (p. 369). Though hailed for two hundred years as a champion of human liberty, Rousseau, too, saw “human” as meaning “man.” Woman was still the Other.
A final example of the tradition of misogyny in historical philosophy is Friedrich Nietzsche, for his time the most influential of the nineteenth-century German philosophers. Nietzsche grew to manhood during the flowering of feminism in Europe and the United States. He thought that the ideas of feminism, with its philosophy of sexual equality, were ridiculous, part of the “litter of democracy,” as were any other notions that people had any inherent right to equal treatment in the society. Equality between man and woman is impossible, he said, as well as dangerous. A woman will be content with subordination if the man is truly a man. Anyway, her perfection and happiness lie in motherhood. “Man is for woman a means; the end is always the child. But what is woman for man? ... A dangerous toy.... Man shall be educated for war and woman for the recreation of the warrior; everything else is folly” (Nietzsche, 1964, p. 75).
Aristotle, Rousseau, and Nietzsche are not selected for comment here because they are special in their thinking about women; rather, in the long history of philosophy until very recent times these giants of Western philosophy are typical in their derogation of women and in their assumption, rarely questioned, that women are an inferior order of being for whom equal status with men is unthinkable. It was not until the 1970s that feminist analyses of philosophy began to reveal the systematic flaw of misogyny in the science that seeks truth through reason and logic (English, 1978; Moulton, 1976; Pierce, 1975).
A minor theme: the argument for equality
Though the inequality of women with men was a basic assumption in almost all the great philosophical systems from the Greeks to modern times, we can still discern among them the thin thread of another argument: that, even allowing for some basic differences between the sexes, women and men should be judged as individuals and should have access to positions of equality in the society and in the law, and that women should not be dominated by and subjugated to men.
The earliest of these, and in some ways the most remarkable, was Plato, a fourth-century Greek philosopher and teacher of Aristotle. In the Republic, Plato’s construction of a utopian society, women were included among the ruling elite, the guardians, though within that class men as a whole had higher status. Private property was eliminated, as was monogamous marriage and the private family. Plato argued that men and women were similar in all respects except physical strength and the bearing and begetting of children. Therefore female and male guardians were to be educated alike in preparation for their assignments in the society. Women would strip for exercise like the men did, and they would not bear children until the age of twenty, in contrast to the child-mothers of his own city, Athens. Considering the time in which he lived, perhaps one of Plato’s most remarkable contributions was his recognition of individual differences among women, as well as among men: “... there is no special faculty of administration in a State which a woman has because she is a woman, or which a man has by virtue of his sex, but the gifts of nature are alike diffused in both ...” (Bishop and Weinzweig, 1979, p. 44).[3]
Male feminists in the nineteenth century were rare, but one such was John Stuart Mill, English philosopher and political economist. In On The Subjection of Women (1869), he stated flatly that the legal subordination of women to men was wrong and should be replaced by a principle of perfect equality, “admitting no power or privilege on the one side, nor disability on the other....” Mill pointed out that the subjection of women is different from that of other oppressed classes, in that men, the masters of women, want not just service but sentiment, too. In other words, he said, men want a willing servant, not one who is inspired by fear. Therefore, women have had to be trained from the cradle to live for others in total self-abnegation. Since any pleasure or privilege that women want can in general only be obtained through men, the object of being attractive to them becomes the guiding star of women’s education and formation of character. Men then use this by representing to women that what they want, that what is sexually attractive to them, is meekness and submissiveness. Thus women take on the yoke of servility and become what men want them to be because they have no other choice.
But as with Plato, Mill had his stopping point. He believed in equal educational opportunities for women and in women’s right to seek careers. But, he wrote, marriage was itself a career, and because of certain psychological differences between the sexes, women should not try to combine a career with motherhood (Annas, 1977).
The Psychology of Women: Science and Social Values
Philosophers, whether misogynistic or egalitarian, probably had little effect upon the realities of women’s lives in the late nineteenth century. Attitudes expressed by opinion leaders such as ministers and educators partook of neither the extreme negative bias of, for example, Nietzsche, nor the egalitarian recommendations of Mill. Rather, the prescription of domesticity and the sentimental idealization of woman and her role were descriptive of the socially valued model of woman’s behavior in both Europe and the United States at the time. At the same time there coexisted the notion of woman as a different order of being. A major feature of her difference was her relative lack of characteristics valued in males, such as originality, creativity, emotional control, and educability—in short, a generalized notion of her inferiority. These two ideas were perfectly compatible with each other, the latter being a rationalization for excluding women from public life and confining them to that sphere in which they could exercise their special qualities of tenderness, nurturance, and devotion to the well-being of others. By virtue of her exercise of these qualities, woman and her place were imbued with a romantic aura that was held to be ample compensation for her inability to do the kinds of things that men did, such as acquiring an education and becoming economically productive. This view of how woman was and how she ought to be was the mode when the young science of psychology began to examine her around the turn of the century.
Psychology is the field of study whose goal is to describe, understand, predict, and control the behavior of humans and other animals. During its early development, in the latter years of the nineteenth-century, little attention appears to have been given to the study of women separate from the study of the adult human. Around 1900, however, there developed in the United States a school of psychology known as functionalism, whose defining feature was its incorporation of evolutionary theory into the subject matter of psychology, emphasizing the concept of adaptation and adjustment to a particular environment. The idea that humans had evolved from lower animals and thus were biologically related to the rest of the animal kingdom influenced the functionalists to apply the concept to behavior as well. Human behavior was seen as the end result of a long process of adaptation and adjustment to the environment, and most important for our subject, it included certain innate components which were biologically based and which humans shared with other animals—such as the maternal instinct. The effect of this trend of thinking gave rise to studies of the biological bases of human behavior, and to studies of individual differences, including the study of gender differences. The Significance of the marriage of evolutionary theory and psychology for the beginning of the scientific study of female behavior was demonstrated in a paper which describes the bridge between myth and science, and shows how, in this case, they served each other (Shields, 1975).
The observable sex differences in brain size, in intellectual and cultural achievement, and in nurturing behavior had long been ascribed to the fact, put forth and advocated by the great authorities of religion and philosophy alike, of the inferiority of the female. For the religious authorities she was a lesser being because of her derivative creation and her fateful behavior in the Garden. The European philosophers of the eighteenth and nineteenth centuries, however, attributed her inadequacies to her lack of male virtues, to the fact, ultimately, that she was not male. In either case her inferiority necessitated her subordination to the male and her relegation to the only role that was natural and suitable for her, owing to her biological endowment.
For scientists, such explanations would not suffice, and thus began the search for more sophisticated ways for understanding what was patently observable: the behavioral differences between males and females. The search began, however, with the same old assumptions that woman’s lesser cultural contributions to the society and her behavior in the domestic role were part of the natural order of things. The problem was to find the underlying mechanism to account for these at a level that would satisfy the scientific intellect. To this end did attention turn to topics which had an early relevance to the psychology of women. Three of these were differences in male and female brains, the variability hypothesis, and the maternal instinct. The history of scientific attention to each of these topics shows how their importance as issues lay in the extent to which they explained contemporary beliefs about women and about sex differences (Shields, 1975).
The notion that sex differences in brain size and in development of different areas of the brain explained sex differences in achievement and personality traits was held by neurologists as well as nonscientists until well into the twentieth century. The investigation of its validity became irresistible once tests for measuring intelligence and other abilities became available. Although interest in the issue diminished rather early owing to lack of corroboration within the testing movement, it reappeared, in a paper associating brain size with the maturing of “other powers” (Porteus & Babcock, 1926). Males, because of their larger brains, would have more of these powers and would thus be more competent and achieving. Such proposals, coming from psychologists, fit readily into the social value system and so could be assimilated under the aegis of science.
The variability hypothesis proposed that males vary more from the norm than females do on certain characteristics, including intelligence. This means that a greater percentage of males compared to females would be found at the upper and lower extremes on measures of those characteristics. Thus, for intelligence, the hypothesis is that males would be more likely to manifest both genius and mental deficiency. This explanation would account for the greater achievement and productivity of men, as well as for the observed greater number of men in institutions for the mentally deficient. The popularity of this hypothesis “did not stem from intellectual commitment to the scientific validity of the proposal as much as it did from personal commitment to the social desirability of its acceptance” (Shields, 1975, p. 744). The corollaries of the hypothesis obviously had strong social implications for women. If genius was a peculiarly male trait, then one would not expect so much from women; therefore, their education should fit them not for the wider world, but for their place in it, and their roles as wives and mothers. The variability hypothesis as one explanation for gender differences has continued to be a topic of interest for psychology. Recent evaluations of the relevant research conclude that the available data are contradictory, and are not in general supportive of the hypothesis (Maccoby and Jacklin, 1974; Shields, 1974).
The concept of maternal instinct, which maintains that women’s nurturing behavior is an innate, biological determinant shared with other female animals, was readily incorporated into the early doctrines of psychology. The idea of maternal instinct in human females was quite compatible with evolutionary theory. Along with it went the broader concept that woman’s reproductive physiology was intimately and causally related to her behavior in general. That most of her energy, both mental and physical, was consumed by the functions of reproduction accounted for the lack of development of other qualities. I he parental instinct of the male was seen as a more abstract, protective attitude toward weak and dependent ones, such as wives and children, whereas it was the nature of the female to respond with specific nurturant behavior to the helpless infant.
The notion of the innateness of maternal behavior was not disputed until the advent of the behaviorist school of psychology in the mid-1920s. The behaviorists successfully challenged the entire concept of instinct in humans, holding that most human behavior was learned. Consequently, interest in the maternal instinct appears now in experimental studies of nurturant behavior in other species. Even so, the idea that women’s greatest fulfillment is motherhood has been remarkably persistent: “as much as women want to be good scientists or engineers, they want first and foremost to be womanly companions of men and to be mothers” (Bettelheim, 1965, p. 15).
Explanations of social and behavioral sex differences which rely on differences in brain size, variability, and the maternal instinct seem quaintly archaic to us now, but it is very easy to see how neatly these concepts met the need of behavioral scientists of a few decades ago to understand the social phenomena of their world. In attempting to move from myth to science, they created new myths which would both explain and justify the social order. “That science played handmaiden to social values cannot be denied” (Shields, 1975, p. 753). Though these issues are now of historical interest only, the search for biological bases of behavior and gender differences continues.
Explanations for the phenomena of female behavior have moved from their mythic beginnings to persistent stereotypes whose acceptance by scientists and lay persons alike impeded deeper understanding, probably being sufficiently satisfying at the time to make further inquiry seem unnecessary. As the influence of functionalism declined from the thirties onward, so too did interest in research on female behavior. Except for continued interest in the topic of gender differences, there was little attention to the scientific study of women by psychologists until the late sixties. Since then research has begun to move beyond the mythic and stereotypic ways of viewing woman toward a sounder understanding of the real determinants of her behavior.
On Understanding Women: Contributing Sources
Knowledge about women is less imperfect and superficial today than it was when the British philosopher John Stuart Mill exposed prevailing beliefs of his time about the nature of women for what they were: inventions of a patriarchal society whose purpose was to justify and to maintain the social order. Women today are becoming conscious of themselves, of their commonalities, and of the influences, only now perceived and articulated by large numbers of them, which have affected their lives and their destinies. Women have begun to reflect upon themselves and their lives, to formulate their own questions, to study women, and to tell what they know. Perhaps in the past, as Mill suggested, women had a stake in preserving the mystique which lay about their behavior, since their status relative to men was one of subordination. It was wiser not to reveal oneself, one’s thoughts and feelings, because such revelation entailed too great a risk to one’s already too-vulnerable position. As woman becomes free standing and attains equal status with man, she can afford to let herself be known. Where are we now in the process of understanding women? Some old problems which impeded understanding have been identified, and some still unresolved issues have been raised.
Human behavior emerges from the neonatal repertoire and becomes organized in a social context. It becomes purposeful and responsive and theoretically predictable. Contrary to popular belief, the behavior of women is not more capricious, cryptic, or occult than the behavior of men. It has, however, been less well understood in any scientific sense because theoreticians and researchers most of whom were men shared certain basic assumptions about women and men which diverted their attention from the critical questions whose answers could have dispelled the mysteries about female behavior.
Not infrequently, when women have been included in research samples, their performance has turned up inexplicable sex differences which constituted an anomaly to the existing theory. Their behavior did not fit with the model which was supposed to predict the behavior under investigation. Confronted with this embarrassment, what alternatives has the investigator? First, he can regard the anomaly as uninteresting and simply ignore it by studying males only. An example of this is the research on the achievement motive, an area which has drawn considerable attention during the past two decades. At the height of this attention, a major review of personality research contained the following:
In general, studies of achievement motivation have been confined to samples of males. The few available reports of experiments on women have been ambiguous and inconclusive (London and Rosenhan, 1964, p. 461).
It was not until 1970, that the anomaly of women’s achievement behavior began to be understood (Horner, 1970).
A second possibility is to interpret the female anomaly in such a way that it can be fitted into the theory, or even to extrapolate from or to add onto the theory to make it cover the incidental other.
The female case has often been neglected, and too frequently forced into inappropriate male categories.... [Psychologists have often set up dimensions where the female can only come out as “not male” (weak instead of strong, small instead of large, etc.). And the persistent tendency to read “different” as “deficient” leads to less than rational controversy in this field, especially where it touches on delicate social balances and cherished mythologies (May, 1966, p. 576).
As we will see, the best (and best-known) example in personality theory, which is basically a masculine model, is that of Sigmund Freud. His basic model of psychosexual development based on the male was adapted to fit the female, and the adaptation utilized primarily the fact of her difference from the male.
The problem with these ways of trying to explain women is that they have a point of view which imposes an inherent necessity on them to explain women in terms of men. Hence, they try to fit woman’s behavior into a conceptual scheme devised from a male stance to explain male motivations and behavior.
The fact that humans occur in two basic biological types, male and female, has made further comparisons between them irresistible. The very large literature on sex differences attests to the fascination that such inquiry has for scientists as well as for lay persons (e.g., Maccoby and Jacklin, 1974). But the practice of studying woman by looking at the ways in which she is different from man has the clear potential for reinforcing the use of a masculine model as a standard for humans, or even for raising a new standard, now built on female criteria. Neither of these is more acceptable than the other. Further, an emphasis on sex differences implies a categorical distinction, a dichotomy of opposites, which is not justified. Woman is not the opposite of man, each being more like the other than either is like their same sex in any other species. The intrasex differences in most psychologically relevant variables are so large, and overlap between the sexes is so extensive, that identification by sexual category offers little in the way of prediction of behavior.
Instead of ignoring female behavior, trying to explain it in terms of models developed from studying males, or emphasizing differences between groups of females and males, one can, alternatively, undertake the serious study of women as women, using interdisciplinary conceptual tools and methods that will illuminate the dark spaces in our knowledge about them.
Understanding women requires that attention be paid to a number of determinants which interact to influence the behavior of any particular woman or narrowly defined groups of women. These include biology, socialization within a social order, life chances, and personality. As determinants of behavior, they range from the widely shared (biology) to the unique (personality).
Biology
In the popular wisdom the psychology of women, their motivations, personality, and behavior, has been closely tied to the events of their bodies. Theorists have attempted to explain women in terms of their bodies, and researchers have looked for the demonstrable effects of women’s bodies on their behavior. All of these approaches suggest a basic assumption that for women the relationship between biology and behavior is a uniquely strong and intimate one. While this assumption may be valid, it has yet to be demonstrated as a universal principle by the conventional methods of science.
It is plain that the biological distinctions between the sexes in infancy do not mediate the development of a feminine or masculine gender; rather, with certain rare exceptions (Stoller, 1972) the sense of oneself as female or male grows from innumerable noncontradictory communications from others, which are normally contingent upon the appearance of the external genitalia (Money, 1972). But that sense is less a function of biological sex than it is of parental reaction; thus the crucial factor is psychological, not biological (Stoller, 1974).
Woman’s body, however, is productive of a number of uniquely female events, shared by almost all women to a greater or less extent and reflected in their experiential histories and in the patterns of their lives. These events include the menarche and the subsequent rhythm of menstruation, breast development, pregnancy, parturition, lactation, and menopause. All are relevant to woman’s role as childbearer and nurturer, and none of them has a counterpart in man’s experience of his body. Thus the biological referents of the social roles of mother and father are not even comparable, let alone equal.
Surely all these are important events in the lives of women. But the search for a direct effect of the attendant body changes on the psychology of women has so far been a fruitless one. Rather, the effects are indirect, linked to the consequences of these events and to the meanings they have for the woman and for relevant others.
The menstrual cycle, for example, is a rhythmic reminder to women of their bodies, and much has been made of its hormonal fluctuations and associated discomforts. But there is no evidence whatsoever that menstruation constitutes a handicap for women in the pursuits of their daily lives or that it noticeably deters them from performing as capably as nonmenstruating people, other factors being equal (see Chapter 4).
When we speak of the importance of women’s biology for the psychology of women we are talking about reproductive biology. Today, the issue is less whether and how her biology affects her behavior than it is how much she is in control of her body and can choose how she will use it. So far, valid and reliable psychological correlates to the biological events of women’s bodies have not been demonstrated. Thus there is no scientific basis for the systematic differential treatment of women on the grounds that their behavior is functionally related to the great and small rhythms of their bodies.
Gender-role socialization
The differential ways that boys and girls are socialized to conform to the appropriate behavioral norms derive primarily from the long history of division of labor along sex lines, which was necessitated by the biological and socioeconomic facts of life. Most social systems use the facts of biological sex to organize the responsibilities and opportunities that men and women have: “... we observe that women almost everywhere have daily responsibilities to feed and care for children, spouse, and kin, while men’s economic obligations tend to be less regular and more bound up with extrafamiliar sorts of ties ...” (Rosaldo, 1980, p. 394).
Such sex-related role differentiation would not necessarily in itself be problematic for women, except for another “universal fact”: because of the content of women’s roles, an asymmetry is set up whereby human cultural and social forms are dominated by men. But such differentiation is functional in societies in which the greater strength of males is put to good use in hunting and foraging activities or in physical defense and conquest; and where the bearing and rearing of children is left to the women. In industrialized societies in which physical strength for work or for war is not so important, the rationale for such bifurcation of personality into male and female models seems not only unwarranted but restrictive and growth inhibiting. A general cultural diminution of sex-role differentiation goes along with a greater valuing of the individual and of ideals of personal freedom, such that the boundaries between behaviors designated as “male” and “female” become more permeable and less rigid.
As jobs and other societal roles are less often tagged as male or female, it is inevitable that socialization practices will change too. They will change together, however. There is little point in desexing child-rearing practices unless both boys and girls have the chance to try out their skills along a continuum of ways of being. Nor will the opening of new work roles be meaningful or successful unless the hitherto ineligible persons have the cognitive styles and personalities to function in them.
Many studies have supported the positive value of moving toward androgynous norms for the socialization of children. Men can be permitted closer contact with their feelings and can develop qualities of empathy and greater concern for others, along with an attenuation of macho need for dominance and display of high activity level and aggression. Women can help both men and themselves by practicing assertion, independence, and poise, and by abandoning the unnatural postures of childishness, helplessness, and docility.
Life chances
Characteristics such as sex, race, ethnic origin, size, physical handicaps, and so on are socially defined. That is, they are given meaning in terms of social norms. On the bases of these meanings, the individual is provided with differential opportunities, which are called life chances. In the past her sex was always a major determinant of woman’s life chances all over the world, the fact that she was born female being the single most important determinant of what she would be doing thirty years hence. Today, the importance of her sex as a predictor is quite variable. The chance that a woman has to escape from traditional role requirements and to exercise some degree of control over her own life depends to a substantial degree on the country, class, and ethnic group into which she was born. Childrearing practices, important as they are, only reflect these variables and the value systems associated with them.
For example, consider a report that offered a global perspective and addressed what may be the most important problem of all: the relation between women’s equality of opportunity and their fertility in both developed and undeveloped countries all over the world (Dixon, 1975). Based on data gathered for a United Nations report on the status of women, the report contained compelling evidence of a strong relationship between women’s status in education, employment, the family, and public life on the one hand, and their reproductive behavior on the other. If one grants that education, employment opportunity, the right to self-determination in one’s personal life, and participation in public life all convey power on the person who has them, and that the extent to which one has power or is powerless relative to others is a determinant of behavior, then these factors become important to the psychology of women.
Personality
The word personality is defined and used in a bewildering variety of ways, to mean everything from an evaluation of one’s charm and vivacity to a description of a set of characteristics which define one as unique from all others. That personality, unlike constructs in the physical sciences such as electricity, eludes precise definition is generally recognized by psychologists. But some definitions are more widely used and respected than others, and one of those is that personality is the dynamic organization within the individual of those psychophysical systems that determine his characteristic behavior and thought (Allport, 1961, p. 28).
Certain key words in this definition merit attention, especially within the context of thinking about the psychology of women. Dynamic organization means that personality is always changing and developing, that it is a process, while at the same time it has a systematic unity which relates its components to each other. This attribute accounts for the stability of a person’s behavior across time and situations. Psychophysical systems recognizes that personality has both psychic and physical components, its organization drawing from both mind and body and fusing them into a unity. The word determine means that personality is an active agent in the patterning of the individual’s behavior. Finally, characteristic emphasizes the individuality of personality, the uniqueness of its particular organization in the individual.
At this point, an emendation of Allport’s definition is in order. Personality alone does not determine behavior. A person, for example, may characteristically be shy and reserved in social situations but under certain conditions may become quiet animated and gay. Therefore, to avoid the implication that personality is the determinant of behavior, let us change it to read:
Personality is the dynamic organization within the individual of those psychophysical systems that interact with situational variables to determine an individual’s characteristic behavior and thought.
The term temperament should be distinguished from personality. Temperament refers to dispositions that are largely biologically derived, such as sensitivity and reactivity to stimulation, emotional lability, and so on, dispositions which are manifest quite early in life, before learning has either attenuated or enhanced them. Temperament has been considered to reflect innate, largely hereditary predispositions to behave in certain ways. Thus, along with such attributes as intelligence and physique, it can be thought of as the raw material of personality (Allport, 1961).
To speak of temperament as biologically derived, as a spectrum of genetically determined predispositions to behave in certain ways, should not suggest that personality traits are inherited, and certainly not that the “feminine personality” is passed down from mother to daughter. It is reasonable to assume that the distribution of such predispositions is the same for both sexes. That is, the “raw material” with which environmental events will interact to shape the person is not systematically different for the two sexes. Although males have a greater predisposition to behave aggressively early in life, they exhibit a wide range of individual differences in the display of aggression, as do females. Clearly, aggressive impulses can be shaped by environmental intervention in the direction either of repression or of release.
Although theorists emphasize different aspects of the various factors that contribute to the development of personality, most would agree that the outcome is determined by the experiential history of the person, the kind and degree and pattern of experiences she has had, impinging upon and affecting the development and maturation of the basic or innate qualities that were there at birth. The behavioral repertoire of the neonate is not large, consisting mostly of motoric and unlearned reflexive behavior like crying and sucking. But individual differences in temperament are observable in very young infants. Thus the uniqueness of the developed personality comes about through the interaction of the person’s unique experiential history, which begins at birth, with a unique set of “givens,” the result being an infinite array of individuals, no two alike.
The importance of this for the psychology of women is that intrasex variability is very large, a fact that is often forgotten in the enthusiastic search for gender differences. Acting on a spectrum of predispositions which may become manifest at different maturational levels are thousands of complexes of events producing reactions which are themselves events, all shaping the personality of the individual woman.
We have discussed four sources which influence the behavior of women. At the present time we have no idea what the relative importance of their contribution is to the behavior of any particular woman. Each person, it has been said, is like all other persons, like some other persons, and like no other person (Kluckhohn and Murray, 1949). If we apply this truism to the study of women, we see that its categories describe the contributory sources of behavior that we have been talking about: biology, socialization, life chances, and personality.
From birth woman confronts the world with a body which is more like all other women’s than it is like any man’s. The socialization pressures of family and school are similar to those experienced by many others in her society. She shares life chances with others of her social class, her race, her neighborhood, and her qualities of health, beauty, and so on. From all this material is organized her ineffable and unique personality, with its substratum of temperamental dispositions.
A general theory of the psychology of women must take all these into account in attempting to formulate explanatory concepts about women. In the meantime, however, it is important to look at some early influential theories of the psychology of women. The theories derive not from psychology itself but from psychoanalysis—a system of human behavior whose explanations of female personality are the subject of the next chapter.
2. Psychoanalysis and the woman question
And now you are already prepared to hear that psychology too is unable to solve the riddle of femininity....In conformity with its peculiar nature, psycho-analysis does not try to describe what a woman is—that would be a task it could scarcely perform — but sets about enquiring how she comes into being, how a woman develops out of a child with a bisexual disposition.
—Sigmund Freud, “Femininity,” 1933
Psychoanalysis has been modern society’s most influential theory of human behavior. Developed by Sigmund Freud and his colleagues, it profoundly altered Western ideas about human nature and changed the ways we view ourselves and our experiences. It undermined the treasured belief in the primacy of human reason and in the responsible control of human behavior by free will, the concept that humans freely choose to do good or evil, that their lives are in accordance with a plan of their own devising. Instead, said Freud, we are motivated by strange forces, buried deep in our minds, which are part of the human condition. These shape our behavior and our concepts of ourselves and permeate all our cultural productions and enterprises. Freud’s theories opened a new door to the study of human behavior, revealing sources never before explored by science. They have had a far-reaching effect on psychological theory, research, and practice, as well as on many other expressions of contemporary culture.
But ideas which affect the course of human life do not magically spring Athena-like fully mature from the head of their creator. They are the result of a particular combination of a person and a time and place. In this chapter we shall consider the personal and cultural background of Freud’s thought, and the development and extension of psychoanalytic theory, particularly as it purported to explain how “a woman develops out of a child.”
Sigmund Freud
Freud was born in 1856, the first child of a young mother who gave birth to six other children in the next nine years. His father was a Jewish wool merchant, and the family was solidly middle class. Freud received his medical degree from the University of Vienna, where he had been especially interested in the physiology of the nervous system. In 1886, he opened in Vienna a practice in neuropathology, diseases of the nervous system. In that same year he married Martha Bernays, who became the mother of their six children.
Freud’s personal life was conventional and conservative. Martha was a proper Victorian hausfrau, loving and subservient to Freud, who was a faithful husband and fond father. His attitudes toward women and his beliefs about the appropriate relationship between the sexes were conditioned by his own personal experiences within the cultural milieu of the time in which he lived. Central European society was strongly patriarchal, distinguishing clearly between the roles of men and women, relegating to men all the duties and privileges of their assignments in the outside world and to women the responsibilities of home and children. Along with this went the assumption that male dominance and superiority were the natural order of things, and that the female, who provided the serene comforts of domesticity, was entitled to the love and protection of the man who married her.
During the early years, Freud was very critical of the feminist argument for equality between the sexes. He reacted strongly to John Stuart Mill’s On The Subjection of Women, a treatise arguing for the emancipation of women from economic bondage and for their full participation in life outside the home. Freud thought that it was “absurd” to suggest that a married woman could earn as much as her husband, in that her domestic responsibilities demanded the whole of a human being. Further, the earning of a livelihood would require the suppression of her tender attributes, the ideal of womanhood, determined by nature through her beauty, charm, and sweetness. “ ‘Law and custom have much to give women that has been withheld from them, but the position of women will surely be what it is: in youth an adored darling and in mature years a loved wife’ ” (quoted in Jones, 1953, p. 176–77). These sentiments and the ideology underlying them were not directly related to the later developed content of psychoanalytic theory, but they help to account for the assumptions inherent in Freud’s later formulations of female personality development and female sexuality.
The early development of psychoanalysis
In 1885, Freud went to Paris to study with the famous neurologist Jean Charcot, who was interested in the relationship between hysteria and hypnosis. Hysteria, a commonly observed condition at the time, was thought to afflict mostly women. In fact, the word hysteria was derived from the Greek hystera, meaning uterus, since early Greek physicians had believed that its symptoms were caused by the wanderings of the uterus through the body and its eventual settling in some part. Hysterical symptoms included a variety of afflictions of the muscles and senses which had no apparent organic or physical cause. They included paralysis, loss of speech or hearing, blindness, loss of sensation, trancelike states, and shaking spells, as well as inexplicable aches and pains and conditions in which the body “mimicked” such normal processes as pregnancy. Although Charcot believed that hysteria was a “real” disease, caused by degeneration of the nervous system, he had observed that the symptoms could be relieved by hypnotic suggestion, an instruction to the hypnotized patient that her symptom would be gone upon emerging from the hypnotic state. Freud was impressed with Charcot’s demonstrations, but he found that hypnotic suggestion was ineffectual with many patients. Back in Vienna, he began experiments with a modification of the technique, which involved asking the hypnotized patient to recall the earliest events related to the development of the symptom. He found that if the patient recalled the events, and also felt the emotion appropriate to the original situation, the symptoms would be relieved.
The idea of having the patient, under hypnosis, try to recall the circumstances of the beginning of her illness came to Freud from Josef Breuer, an older physician, who had told him some time before about the case of “Anna O.” This young woman, while nursing her ill father, had developed symptoms, including a cough, a squint that interfered with her vision, headaches, and various paralyses and areas of numbness, which Breuer recognized as hysterical. After the father’s death, Anna’s illness became worse. She began having agitated episodes of hallucination during the day, followed by dreamy, trancelike states in the evening. She and Breuer discovered that if she related to him the details of her hallucinations while she was in the evening trance, she would be relieved and tranquil during the rest of the evening. Later, they found that her troublesome physical symptoms could be removed if she recalled unpleasant events associated with them and talked about them under hypnosis, expressing also the feelings aroused by the memory. Anna called this process the “talking cure,” or “chimney sweeping.” Breuer named it the cathartic method. After a year and a half of treatment, Anna was relieved of her symptoms.[4]
Freud’s knowledge of Anna’s case and his experience with his own patients led him to the belief that the cathartic method was more effective than hypnosis, and he eventually developed a technique called free association in which the patient was instructed to talk about everything that came into her mind, no matter how ridiculous or improper it seemed. Such a train of associations, Freud believed, would lead back to the buried memory that was responsible for the patient’s symptom.
Having become quite successful in treating hysterics with this method, Freud persuaded Breuer to work with him on a book which appeared in 1895 as Studies in Hysteria. The core of their theory was that hysterics suffered from buried memories of a painful or traumatic nature, and that all such memories with their repressed emotions had sexual features. Freud’s association of hysteria with repressed sexual experiences led him to two important discoveries: the effect of unconscious motivation on behavior, and the role of sexuality, particularly in childhood, in human development.
The unconscious, Freud proposed, was a repository of memories which were not available to the individual—they could not be recalled at will. Because they represented events that had caused mental pain or shock, they had to be repressed, relegated to the realm of the unconscious. They continued to have effects, however, and were manifested in dreams and in such everyday experiences as forgetting, slips of the tongue, and other “mistakes,” which, if analyzed by free association, could reveal their source in the unconscious. If the memories had sexual content, they could produce hysterical symptoms. An understanding of puzzling behavior, and the relief of symptoms with no apparent physical catise, could be effected only by bringing to light their unconscious motivating causes, and by releasing the pent-up emotion with which they were originally invested.
The psychosexual stages
In 1905 Freud presented his general theory of sexual development in Three Essays on the Theory of Sexuality. This work, with its later revisions, and his final book, An Outline of Psychoanalysis (1939), deal with infantile sexuality, sexual aberrations, and the stages of sexual development which Freud thought were a universal pattern for all males and females. His later work on the psychology of women grew directly out of this early theoretical unfolding of the development of sexuality through what came to be called the psychosexual stages.
Freud postulated the presence at birth of an undifferentiated sexual energy which he called libido. Early in life the libido was not directed toward or focused on any particular object, nor was it localized in any part of the body. The selection of sexual aims and objects came later as a result of experience. This generalized sexual potential of the infant, which he called polymorphous perversity, made possible the later channeling of sexuality into a variety of expressions, from “normal” heterosexuality to more unusual behaviors such as homosexuality, fetishes, and so on. Freud’s theory of psycho-sexual stages shows how the individual moves from the undifferentiated stage of polymorphous perversity through successive stages in which the libido is organized around certain areas of the body to the final stage, mature genital heterosexuality. This sequence of events, he said, had crucial implications for personality development, and for the later observable psychological differences between the sexes.
The infant’s earliest source of gratification and pleasure is in activities associated with feeding. Hunger is an uncomfortable sensation. Relief comes in the form of the mother’s breast, rhythmic sucking, and warm milk, all inducing peaceful relaxation. Later, sucking by itself becomes a pleasurable activity, leading Freud to believe that such oral behavior that was not nutritional in its results was sexual in nature. Thus, the mouth and lips are the first area of the body to be associated with sexual pleasure. Freud called areas sensitive to pleasurable stimulation erotogenic zones. During the first year of life, the mouth is the primary erotogenic zone, and that period came to be designated the oral stage of psychosexual development.
During the second and third years of life the child develops control over certain body functions, notably the retention and expulsion of feces. Successful mastery of bowel activity is greatly valued by the parents, who bestow warm praise for productive and proper performance. Also, the child’s self-stimulation by retention and expelling feces, and the rhythmic quality of the action, are themselves pleasurable and gratifying. Thus the anal region becomes an erotogenic zone, and the anal stage succeeds the oral stage of psychosexual development.
The three- or four-year-old child has attained mastery over anal functions, and is also physically well coordinated. Now able to manipulate almost any part of the body at will, the child discovers the pleasure potential of the genitals and of infantile masturbation. The locus of sexual pleasure shifts to the genitals, and the child moves into the phallic stage, the last sexual stage of infancy, the most likely to be fraught with problems, and the most important for personality development. Although the word “phallic” comes from the Greek word phallus, meaning the male genital organ, the phallic stage characterizes the development of both sexes, whose libidinal aim now is the stimulation of the genital regions: for the male, the penis; for the female, the clitoris.
Around age six, the child ceases to display overt sexuality and enters a period which Freud called the latency stage. Sexual impulses are not extinct, but essentially lie dormant until their re-emergence at puberty. Infantile sexuality associated with the oral, anal, and phallic stages becomes repressed as a part of the contents of the unconscious, where it may later exercise effects on the individual’s behavior, dreams, and personality.
Puberty terminates the latency stage, and the young person enters the genital stage, characterized by a resurgence of the sexual impulses. The libido, whose aim has been the self-induction of pleasure through the stimulation of parts of the body, may now be directed toward a member of the other sex. In the normal course of events, the individual has reached psychosexual maturity.
Freud thought that the psychosexual development of boys and girls is the same until they reach the phallic stage, whose events were fatefully linked to the attainment of normal personality and sexuality, and to those behavior patterns called masculinity and femininity. Both have the mother as their Erst love-object, and both have their earliest identification with her. During the phallic stage, however, the boy develops sexual wishes for the mother, and begins to see his father as a hated and powerful rival. Freud saw in this development a resemblance to the theme of Oedipus Rex, a fifth-century b.c. Greek drama by Sophocles. Before Oedipus is born, the Delphian oracle tells his father, Laius, that the expected child will grow up to kill his father and marry his mother. In order to prevent such a horror, Laius tries to get rid of the baby at birth by having him abandoned on a mountain. The child is rescued, however, and as an adult he unwittingly fulfills the prophecy by slaying Laius and marrying his mother, Jocasta, the Queen of Thebes. After fathering four children by her, he learns the truth of what he has done and in his horror he puts out his eyes. Freud saw in this story a universal theme that must be in the experience of every small boy. He named it the Oedipus complex.
During this same period that the boy is having unacceptable and anxiety-provoking feelings toward his mother and father, he discovers that girls and women do not have a penis, that organ from which he derives such pleasure. He comes to the conclusion that it has been cut off, probably as a punishment for some misdeed. Such a fate could also happen to him, especially because of his secret desires for his mother and his death wishes toward his father. Thus castration anxiety becomes an important feature of this stage, causing unbearable conflict and psychic distress. The resolution of this greatest of childhood’s problems, Freud thought, came about through the mechanism of repression, the relegation to the unconscious of the Oedipal wishes and all other sexuality as well, thus ushering in the latency stage. The boy then moved, at an unconscious level, into an identification with the father and his masculinity, and finally into psychosexual maturity.
Freud’s theory of female development
And what about the little girl? How did she resolve her phallic stage, move into latency, and develop a feminine identification? Freud first presented a theory of female psychosexual development in Three Essays. Much later he wrote three papers in which he integrated these ideas into a theory of female personality. These are “Some Psychical Consequences of the Anatomical Distinction between the Sexes” (1925), “Female Sexuality” (1931), and “Femininity” (1933). During his earlier writings, Freud held to a vague notion of a parallel development of girls and boys, based on the model of the boy and his resolution of the Oedipal conflict. But all along, he spoke from time to time about the puzzle of female psychosexual development. In Three Essays he wrote: “The significance of the factor of sexual overvaluation can best be studied in men, for their erotic life alone has become accessible to research. That of women ... is still veiled in an impenetrable obscurity” (Freud, 1976i, p. 551). Almost twenty years later, in a paper on the phallic stage, he confined his descriptions to the male child, because “the corresponding processes in the little girl are not known to us” (Freud, 1976d, p. 142). As late as 1926 we find him saying that this ignorance was no cause for shame: “after all, the sexual life of adult women is a ‘dark continent’ for psychology” (Freud, 1976f, p. 212).
The little girl enters the phallic stage, as does the boy, with the discovery of the genital zone and the pleasures of masturbation. Freud saw no particular psychological significance to this early masturbatory activity in either sex. It began as an inevitable discovery as the child explored its body, and was maintained because it was pleasurable. The psychological consequences came later. Early in this stage, Freud declared, the little girl was destined to make a “momentous discovery.” She would notice the penis of a brother or playmate, visible and large, see that it was superior to her own small organ, “and from that time forward fall a victim to envy for the penis” (Freud, I976h, p. 252).
The psychological consequences of her envy for the penis are of critical importance in her subsequent personality development. She perceives that she has been castrated, a personal wound to her self-esteem, and she develops a permanent sense of inferiority. When she learns that her lack of a penis is shared by all females, she develops a feeling of contempt for her sex. Even later, when she no longer consciously envies the male his penis, she is left with a residual of this envy in the form of jealousy, a character trait that Freud thought was much more important in the mental life of women than of men because of its early reinforcement by penis envy.
Another consequence of the girl’s discovery of her genital inferiority is the abandonment of her mother as a love-object. The mother, herself sharing the daughter’s inadequacy, is blamed for the lack of a penis. At this time, the girl’s libido shifts from her mother to her father. Father is taken as the love-object, and mother is seen as her rival. She will now substitute for her unrealizable wish for a penis the wish for a child. In this transfer of the object of her libido to the male, and in the equating of penis with child, she thus resolves her penis envy and prepares to move along the course of normal femininity.
However, two other lines of development may diverge, which preclude the normal outcome. In the first, the girl finds that the pleasure she took in clitoral masturbation is now spoiled by her envy of the penis. She expresses dissatisfaction with her inferior clitoris by striving against any gratification from it, repressing her sexual impulses, and thereby laying the basis for neurotic problems later in life. In the second, she refuses to accept the fact of her castration, defiantly clings to phallic masturbation, and develops along a principle of activity which Freud called a masculinity complex. By this he meant that she would cling to her threatened masculinity, and to her hope for a penis. The fantasy of being a man in spite of everything would pervade her life, so that she might become homosexual, and be compelled to behave as though she were a man.
Freud thought that the girl had a more difficult transition than a boy to effect in her development toward adult sexuality, for two reasons. First, she had to make the transfer from her original loveobject, her mother, to her father; and second, she must change her erotogenic zone from the “phallic” clitoris to the vagina. Thus her libidinal mode of satisfaction had to move from an active to a passive one. Freud’s explanation for the necessity of this, and its effects on female sexuality, is rather complicated, but an understanding of it is important for a balanced evaluation of his theory.
Freud began the last of his three papers on women with a discussion of anatomical bisexuality. He noted that male and female genitalia differentiate out of the same embryonic structures, and that vestiges of the male internal reproductive structures are found in the female and vice versa. Anatomically, he said, the human is bisexual, but more one than the other. Likewise, it is common to speak of certain behaviors as masculine or feminine, regardless of who is displaying them. But this distinction is not truly a relevant sexual one, in that what is usually meant by “masculine” is “active” and by feminine, “passive” and, Freud stressed, it is plain that both sexes can display both activity and passivity. Women can be active in many directions, and men must develop considerable passivity if they are to live in community with others. Therefore, Freud concluded, it is incorrect to equate masculinity with activity and femininity with passivity. One can characterize femininity as giving preference to passive aims, but this is not the same as passivity, since considerable activity may be required in the achievement of a passive aim. How is this related to the transfer of eroticism from the clitoris to the vagina? The libido, Freud said, is neither masculine nor feminine. There is only one kind of libido, present in both sexes. The libido by definition is instinctive, and all instincts are active. Thus, following the convention that equates “active” with “masculine,” the libido is often thought of as masculine. But Freud cautioned that in this usage it must not be forgotten that it also includes passive aims, which occur in the female when the sexual energy is transferred from the clitoris to the vagina.
During the pre-Oedipal period, the little girl’s sexuality is of the same active thrusting kind as the boy’s. Upon learning of her “castration” and abandoning her mother as love-object, she also gives up her clitoral sexuality as she moves into the latency period. Freud thought that the vagina was relatively insensitive prior to puberty, deriving what sensitivity it had from the clitoris and the anus. The vagina, in fact, was for most children undiscovered in childhood owing to the primacy of the phallic clitoris. When clitoral sensitivity reappears at puberty, it no longer has the active aim of the earlier period, but now is likely to be used autoerotically in masturbation, or, in heterosexual activities, as part of foreplay preparatory to sexual intercourse. Freud did not believe that the clitoris lost its sensitivity, or became anesthetic, but rather that clitoral sexuality was converted into a passive aim as sensitivity was transferred to the receptive vagina (Mitchell, 1974a). A woman might remain “clitoridal” all her life, with no wish for penile penetration, exemplifying arrested development of her femininity. The normal adult woman would be able to have orgasm by vaginal stimulation; to be able to have orgasm only by clitoral stimulation was psychosexually immature.
Freud thought that sexual development of the girl from the active aims of her pre-Oedipal clitoral sexuality to the passive aims of her adult vaginal receptivity was more difficult than that of the boy, and that she was more susceptible to psychological disturbances on account of this. Residuals of the early “masculine” period were common, and some women experienced frequent alternations between the masculine and feminine phases, an expression and a reminder of the bisexuality inherent in the female condition. The psychic energy required to bring about normal femininity had a draining effect on the female, and could account for her lower sex drive and for the frequency of frigidity in women. In some women, a lack of interest in sex or the vaginal anesthesia that characterized true frigidity might be psychogenic, but other cases suggested that such problems might be caused by constitutional or even anatomical factors. In any case, he believed, the accomplishment of the biological aim is effected by the aggressiveness of the male, and is independent to an extent of the cooperation of the female.
Certain features of normal mature femininity, Freud proposed, flow from the girl’s pre-Oedipal identification with her mother, her discovery of their common genital inferiority, and the shift of her libidinal aim to her father. The girl’s early doll play, for example, is an expression of identification with her mother; she is her mother, and the doll is herself. Later, when penis-envy is established, the doll-baby becomes a baby from the father, the aim of her strongest wish. Because of her identification of penis with baby, motherhood is a special joy, especially if the baby is a boy, bringing with him the longed-for penis. Freud believed that the mother-son relationship is the most perfect and most free of ambivalence of all human relationships. She can realize through her son all the ambition she had had to suppress in herself, and through him she can satisfy all that was left of her old masculine strivings.
But penis envy had long-term consequences, expressed in traits which Freud thought characterized adult women. One of these was narcissism,[5] a preoccupation with the self which was reflected in a strong need to be loved. Another was vanity, seen in the value which women placed on their physical charms, the more important to them as a compensation for their original sexual inferiority. A third was shame, whose original purpose was the concealment of genital deficiency.
Because the girl was spared the boy’s traumatic resolution of his Oedipal complex under threat of castration, she never totally had to abandon her libidinal interest in her father. Because she was under less duress, her personality would fail to develop the rigorous components of what Freud called superego, which gives rise to conscience, morality, and other traits that mark civilized man. This is why, he proposed, women have little sense of justice and a weak social interest. Finally, Freud offered a comparison of the typical female patient of thirty with her male counterpart. He is still youthful, able to make good use of the possibilities that analysis would open up for him. She, on the other hand, seems rigid and less open to change. No paths are open to further development; the whole process has run its course, as if, Freud said, the development to femininity had exhausted the possibilities of the person.
Criticism of Freudian theory
Freud’s theories, influential as they have been, have attracted criticism almost from their beginnings. First there arose apostates from Freud’s own circle in Vienna, some of whom parted ways with Freud to set up rival systems of analytic theory. One of these was Alfred Adler, whose work we shall consider in the next chapter. Since then, the strongest criticisms have emanated from psychologists and from philosophers of science who fault Freud’s theories and psychoanalysis in general on methodological grounds.
Psychoanalysis, unlike psychology, is not grounded in empirical science, which relies upon the experimental testing of hypotheses using the scientific method. Rather, psychoanalysis over the years has stayed close to Freud’s original theory of personality and to the type of psychotherapy that grew out of it. Developments since Freud have mostly been elaborations of his ideas, the years of practice and endurance as a system having provided them with a patina of credibility, which, in the minds of some, they do not deserve (Grunbaum, 1984). Freud derived his theories from his patients’ accounts and from his own self-analysis, methods that are a fertile source of ideas but do not meet scientific criteria for proving anything. An example is Freud’s theory of repression, which is at the core of psychoanalysis. In theory, repression is the relegation to the unconscious of painful memories of childhood or of unacceptable wishes and thoughts. These give rise to neuroses in later life. If the repression is lifted through analysis, and the unconscious becomes conscious, the neurosis is relieved. The problem is that the theory is not testable by the methods of science, since it deals with mental events that are not observable. Also, it is not actually possible, within a treatment setting, to establish with certainty a link between an event or pattern of events of childhood and an adult neurosis. One may strongly believe that the link is there, but belief does not constitute scientific proof.
Another example is Freud’s theory of “penis envy,” a key concept in his theory of female personality. Penis envy has never been shown to have objective reality in the lives of girls and women. Even if girls did go through a period of feeling they had been denied something important to their bodies, it has likewise not been shown that these feelings of deprivation in childhood would have any effects upon their later personalities. Many have predicted that if psychoanalysis is going to survive as theory and practice, it must subject its statements about human behavior and development to the rigorous testing of modern science (Grunbaum, 1984).
Freud’s theories of female sexuality and personality have drawn heavy fire from feminist critics during the past few years. Because of the key role of penis envy, which is based on the anatomical distinction between the sexes, the events which proceed from it—the suppression of the clitoris, the dependence of further sexual satisfaction on penile penetration, the need for a male child as penis substitute, the derived model of feminine personality with its less than flattering traits—all seem to rest on a biological base which not only limits the range of possibilities but gives scant recognition to the role of social factors as shaping influences of women’s behavior. Furthermore, at face value the theories clearly depreciate female sexuality and female genitalia. It is the male who aggressively consummates the biological raison d’etre of the species. The whole notion of envy of the male organ, and the girl’s perception of herself and all those like her as inferior castrates, clearly issues from assumptions of male superiority within the context of patriarchal society. Even Freud’s great friend and biographer, Ernest Jones, observed the “phallic” bias of Freud’s position.
On the other hand, both the followers and the critics of Freud have generally ignored his cautions of the tentative nature of his exploration of femininity, his call for further validation, and his disclaimers of final answers. He began his 1925 paper by saying that its findings would be of importance “if they could be proved to apply universally,” and described them as “in urgent need of confirmation before [their] value or lack of value can be decided” (Freud), 1976h, p. 249). In conclusion, he said that though he was inclined to “set some value” on these ideas, “this opinion can only be maintained if my findings, which are based on a handful of cases, turn out to have general validity and to be typical” (1976h, p. 258).
Although Freud certainly did not stress the effects of society as determinants of personality and behavior, he was not altogether unaware of such influence. In his later work, as he spoke of those personality traits that seemed to be more characteristic of women, he denied claiming more than an “average validity” for his assertions, and went on to state that “nor is it always easy to distinguish what should be ascribed to the influence of the sexual function and what to social breeding” (Freud, 1965, p. 132).
In another, earlier paper, “ ‘Civilized’ Sexual Morality and Modern Nervous Illness,” Freud showed how the double standard of morality, the Victorian ideal of abstinence, and woman’s sexual frustrations in marriage brought about neurosis:
Under the cultural conditions of to-day, marriage has long ceased to be a panacea for the nervous troubles of women; and if we doctors still advise marriage in such cases, we are nevertheless aware that, on the contrary, a girl must be very healthy if she is to be able to tolerate it.... On the contrary, the cure for nervous illness arising from marriage would be marital unfaithfulness. But the more strictly a woman has been brought up and the more sternly she has submitted to the demands of civilization, the more she is afraid of taking this way out; and in the conflict between her desires and her sense of duty, she once more seeks refuge in a neurosis. (Freud, 1976a, p. 195).
The young girl was educated to be chaste and was not told what her sexual role in marriage would be. Under such circumstances, she could not suddenly become sexually responsive in marriage: “... the preparation for marriage frustrates the aims of marriage itself” (Freud, 1976a, p. 198).
A recent analysis of Freud and of several of his important recent critics presents a strong argument that orthodox feminist attack on Freud is a serious error (Mitchell, 1974b). Psychoanalytic theory offers an explanation for the oppression of women which explanations relying on biological and cultural roles cannot do. The notion that biology is an innate determinant of personality is not inherent in Freud’s feminine psychology (nor in the whole of psychoanalytic theory), because psychoanalysis does not deal with.biology but rather with the transformation of biological facts into mental representations. The forms of these mental representations are a function of the social reality of patriarchy, which is synonymous with culture. In other words, psychoanalysis deals with the inheritance of a social order, and with its acquisition by each succeeding generation of males and females. That social order is patriarchy, the law of the father, and psychoanalytic theory is concerned with showing how the boy learns his place as heir to the law of the father, and the girl learns her place within it. Thus their concern is with “how the human animal becomes the sexed social creature—the man or the woman” (Mitchell, 1974b, p. 402). The ways in which this happens are not parallel for the two, in that the resolution of the pre-Oedipal active sexuality and desire for the mother, shared by both, must be asymmetrical, consistent with the asymmetry of their places in the patriarchal society. Thus the boy must give up his desire for the mother knowing that he is heir to the father’s place and will some day have a woman of his own. The girl also must renounce her unrealistic love for her mother, not because it is dangerous, but because she has nothing with which to implement it. She learns to identify with her because of their similarities and to expect to take her place. Thus the girl’s Oedipus complex occurs almost by default. It is not as strong as the boy’s, and there is no reason that she must fully give it up. Its acquisition, in fact, sets her on the path to her feminine destiny under patriarchy. Her subjugation to the law of the father means that she becomes the representative of nature and sexuality. In submitting to the law, she becomes its opposite, loving and irrational. Her task is to provide for the reproduction of mankind within the family, where sex is contained and organized. According to Mitchell’s observation, this is the place of all women in patriarchal culture. Differences of class, historical period, or specific social situation may affect the expressions of femininity, but in relation to patriarchy, the law of the father, women’s position everywhere is comparable.
Feminist criticism of Freud, that he overvalued the male in taking for granted that the penis is a superior organ and that anyone who did not have one would feel deprived and be envious, and that he was not sensitive to woman’s powerlessness and lesser status in society, is ill-conceived, argues Mitchell, for several reasons. Such criticism tries to deal with Freud’s statements on feminine psychology outside the contextual framework of psychoanalysis, thus misinterpreting it and distorting its meaning, which can be understood only as an explanation of the psychology of women in patriarchal society. Far from ignoring social realities, the concern of psychoanalysis is with the mental representations of those very realities. The little girl’s renunciation of her pre-Oedipal sexuality and desire for the mother are a prerequisite to her assumption of her place in the real society of ubiquitous patriarchy, just as the destruction of the boy’s Oedipal attachment and identification with the father prepare him to assume his role.
Furthermore, in arguing that cultural conditioning is solely responsible for woman’s inferior role and for the “feminine personality,” Freud’s critics ignore or by implication deny the unconscious and infantile sexuality. The struggle between nature and culture which is the essence of the Oedipal conflict is not conscious or overt, nor is it dealt with overtly. Its repression and inaccessibility to consciousness give it a power which cannot be matched by superficial social reforms or by other changes based on understandings which’ invoke either biology or conditioning as causes for women’s oppression.
Mitchell says that patriarchal ideology, the law of the father, with its prescriptions for women, is “in the slow death throes of its own irrationality” (1974b, p. 143). But its final demise will require a political struggle—a cultural revolution—which may be spearheaded by revolutionary feminism. When this happens, then it will be possible for those mental representations, reflecting the social realities which psychoanalysis is all about, to change in fundamental ways. But for the present and the past, psychoanalysis is an analysis of the human condition in patriarchal society.
Psychoanalytic research and psychotherapy
Psychoanalytic theory, as developed by Freud and his colleagues, was generated and tested by clinical analyses and investigations of patients. The theories of the unconscious and of infantile sexuality, for example, grew out of Freud’s early experiences in the treatment of hysterics. The term psychoanalysis was applied both to theory and to a particular kind of therapy, and the two were closely interrelated. The insights gained in the therapy itself provided data for the development and modification of theory, and the theory in turn guided the process of therapy. Unlike the research methods of modern psychology, which are modeled after those of the physical sciences with their reliance on controlled observation and quantitative measurement, psychoanalytic research was based on case studies of individuals. Elaborate studies of the single case were presented to “prove” or to elucidate a point. Sometimes, a theoretical innovation would be introduced, based on a small number of cases. For example, Jeanne Lampl-De Groot, a Dutch psychoanalyst, supported a thesis on the Oedipal complex in girls with data derived from the analysis of two female patients, and Helene Deutsch attributed female homosexuality to regression to the “masculine” clitoral stage, based on her study of eleven women.
Another characteristic of psychoanalysis is its use of explanatory concepts that are difficult if not impossible to verify. Penis envy, for example, “explains” certain aspects of female personality, but its actual existence and nature have defied illumination, as witness the fifty-year controversy it has generated.
Related to this is a feature of psychoanalytic psychotherapy, which relies upon overcoming the patient’s resistance in order to reveal unconscious material, which is then made meaningful by interpretations which relate it to the patient’s problem feelings and behavior. The free-association process and the analytic skill of the therapist combine to remove resistance to remembering long-buried events, to understand their significance, and to show how their motivating properties have contributed to the presenting symptoms of the patient. But whether or not the interpretation is correct depends on the subjective opinion of the analyst, whose assertion that it is may be impossible to verify. For example, one case described a padent who remembered how as a child he had fainted in the school playground. “This first attack was the unconscious symbolic equivalent of an amorous swoon” (David, 1970, p. 60), which meant his desire for his mother. Obviously such an interpretation taking place many years after the event cannot be checked for accuracy. Freud was aware of such criticisms and offered as a defense his finding that childhood memories persisting into adulthood were screens for important events, usually sexual in nature, and that a correct interpretation of the memory, when recognized by the patient, was often followed by a recession of symptoms. In any case, these characteristics of psychoanalytic theory and therapy have presented obstacles to its acceptance by contemporary psychology just as its male bias, as viewed by feminists, has caused its statements on women to attract withering criticism.
Against all these criticisms however, stands the unassailable fact of the enormous influence that psychoanalysis has had upon Western culture and its interpretations of the human condition. Of women, if it originally did not prescribe how they ought to be but rather analyzed them as they came into being in a patriarchal society, its appraisal continues.[6] Attention is directed not only to Freud’s papers on female sexuality and personality but to his own accounts of the cases of the women who were his patients. One in particular exemplifies the development of theory, the process of therapy, and unwittingly, the dynamics of patriarchy as they affect both. In 1905, Freud published “Fragment of an Analysis of a Case of Hysteria,” better known as the case of Dora.
Dora was eighteen when she was brought to Freud by her father, whom Freud had treated several years earlier for syphilis. The precipitating reason for the consultation was a letter written by her, and found by her parents, in which she said goodbye to them with the implied intention of taking her life. Although her father doubted that she was serious, he was disturbed enough to insist that she see a doctor. She also had a “nervous” cough, with a history of fainting spells, loss of voice, headaches and depression going back to childhood. Freud diagnosed her collection of symptoms as a typical case of hysteria, and set about an analysis to uncover the cause, which by that time he was already convinced lay in the repressed content of early sexuality. His treatment of Dora lasted for three months, until she abruptly terminated it, much to Freud’s disappointment.
Dora’s family included her parents and a brother who was one and a half years older. Dora was “tenderly attached” to her father. Her mother, whom Freud never met, was a pallid creature who spent her time obsessively cleaning the house. She and Dora did not get along. Dora was very critical of her, and ref used to be influenced by her, at least consciously. The brother took the mother’s side in family arguments, and Dora and he had grown apart. Thus were father and daughter aligned against mother and son, a drama with which Freud by now was very familiar. Earlier, a governess had been part of the household. She and Dora had been close until Dora began to believe that the older woman’s kindness to her was a strategy to attract her father, with whom the governess had fallen in love.
Dora was precocious as a child, and Freud described her at eighteen as lively and intelligent. She attended lectures and was interested in her studies. Having experienced a variety of medical treatment since childhood for her various symptoms, she now laughed at the efforts of doctors and refused to see them. Her father induced her to see Freud against her will, she told him, and she had decided to “put up with it” until the New Year. Her last session was on December 31, 1899.
Dora’s father revealed to Freud what he thought had precipitated Dora’s most recent illness and the suicide note. Her parents had some time ago formed a close friendship with a married couple, Herr and Frau K. Frau K., an energetic and attractive woman, had nursed Dora’s father through a long illness, and Herr K. was especially fond of Dora, going on walks with her and bringing her presents. Dora and Frau K. had spent much time together, and had been confidantes, a type of relationship that Dora had not had with her mother.
Two years before, said the father, Dora had reported that Herr K. had made an indecent proposal to her while they were walking by a lake. She had slapped him in the face and had gone home alone. Confronted by her father, Herr K. denied that any such episode had occurred, suggesting that Dora’s imagination had been inflamed by reading books with sexual content, and that she had fantasied the whole thing. Dora’s father believed him. But Dora insisted that he break off relations with the K.’s, especially with Frau K. This her father refused to do on the grounds that Herr K. was innocent, and that his own relationship with Frau K. was platonic.
After Dora started in treatment with Freud, she told him of still another episode with Herr K. when she was fourteen. She had gone to his office to watch a street festival, and he had embraced and kissed her. She reacted with disgust and ran home. For some time, she avoided being alone with him.
Freud found Dora well informed about sexual matters, and apparently she was able to talk freely to him. She was insistent on two things: her father and Frau K. had been having an affair for years, and Herr K. had tried to seduce her. To Freud’s credit, he believed her: “... I came to the conclusion that Dora’s story must correspond to the facts in every respect” (Freud, 1976c, p. 46). He thought that the sexual trauma of Herr K.’s initial advance, when she was fourteen, provided an explanation for Dora’s symptoms, in accordance with the theory which he and Breuer had derived for the etiology of hysteria. But there was much, much more. Analysis of her dreams was consistent with Freud’s theory of the girl’s Oedipal love for her father. Dora was reacting to her father’s affair with Frau K. as if she were a wronged wife or a betrayed lover—as if she were the woman her father once loved, her mother, or the woman he now loved, Frau K. Since she was neither of these, her reaction, which Freud interpreted as jealousy, was inappropriate. Furthermore, he thought that her reaction to Herr K.’s advances, even when she was fourteen, was “entirely and completely hysterical” (p. 28). Without question this was true of any person in whom an occasion for sexual excitement elicited exclusively negative feelings. Instead of the genital sensation which would have been felt by a healthy girl in such a situation, Dora had felt disgust. Disgust is an oral phenomenon, and this, along with her throat symptoms of coughing and loss of voice, Freud related to her fantasies of her father and Frau K. having oral intercourse.
Although she denied it, Freud insisted that Dora was sexually attracted to Herr K. Her feeling for him reflected both her feeling for her father and her feeling for Frau K. That is, she identified Herr K. with her father, and herself with Frau K. Thus her attraction to Herr K. was a recapitulation of her father’s love affair with Frau K.
Freud interpreted Dora’s unexpected termination of her therapy as evidence of his newly developing theory of transference, the psychic mechanism by which a patient transfers to the therapist old feelings and conflicts which she once felt for significant persons, such as her mother and father. Just as she had transferred her love for her father to Herr K., so she now transferred in the therapeutic situation some of the same feelings to Freud. But these feelings were negative as well as positive, and for her treatment at the hands of the other two she would take her revenge on Freud, by deserting him. She was saying, Freud thought, “Men are all so detestable that I would rather not marry. This is my revenge’’ (p. 120). Dora’s termination caught Freud by surprise. Fifteen months later, she visited him one more time for treatment of a facial neuralgia that had started two weeks earlier. He showed her that exactly two weeks before she had read an article about him in the newspaper. Thus her pain was a self-punishment for the double crime: the long-ago slap at Herr K. when he had compromised her virtue, and her peremptory treatment of Freud in her abrupt termination of their relationship.
Freud never saw her again. But a half century later, Dora reappeared in the psychoanalytic literature. Felix Deutsch (1957) revealed that in 1922 he had been asked to do a “psychiatric study” of a middle-aged woman who turned out to be the Dora whom Freud had made famous. Deutsch found her still complaining of symptoms which he thought were hysterical: dizziness, ear noises, and migraine headaches. She complained that her husband was unfaithful, and denounced all men as selfish, demanding, and ungiving. Many years later, Deutsch, having learned of her death, made inquiries about the course of her life during the intervening years, and was told that her symptoms had continued throughout her life. In fact, said Deutsch’s informant, she had been “one of the most repulsive hysterics” he had ever met.
Freud published this case, incomplete as it was, because he thought it was an important demonstration of the sexual origin of hysteria. Dora’s Oedipal love for her father, her transfer of this feeling to Herr K. (even though she persistently denied any sexual arousal in her encounters with him), her conscious jealousy of Frau K. and her unconscious identification with her—all these features of the case made it important to Freud. But suppose we examine it from Dora’s perspective. How did it feel to be Dora, a teenage girl in turn-of-the-century Vienna? What was the state of her relationships with the significant people in her life?
She and her mother had never been close. Her mother seems to have been unable to help her daughter, and presented such an unattractive model in her role of obsessional housewife that Dora looked elsewhere for a woman she could love and admire. The kindness of her governess was not genuine, but was an exploitative means of winning Dora’s adored father. She became very attached to Frau K., who appeared fond of the girl only to betray her in the same way. The once-loved brother abandoned her, joining with the mother in an attitude of rejection. Herr K., family friend and admired adult, made indecent proposals to her, then lied about it. And her father chose to believe him, at the same time denying what was obvious to everyone (including Freud), that he was having an affair with a woman who Dora had once thought was her friend. “None of her father’s actions,” Freud wrote, “seemed to have embittered her so much as his readiness to consider the scene by the lake as a product of her imagination” (p. 46). Freud thought she was over-reacting, but saw that in another respect her reproaches about her father were justified: “When she was feeling embittered she used to be overcome by the idea that she had been handed over to Herr K. as the price of his tolerating the relations between her father and his wife” (p. 34). Freud himself believed that the two men were engaged in an unspoken conspiracy in which Dora was the pawn: her father would ignore Herr K.’s attempted seductions of his daughter in exchange for Herr K.’s pretended ignorance of his wife’s affair with Dora’s father. “[E]ach of the two men avoided drawing any conclusions from the other’s behaviour which would have been awkward for his own plans” (p. 35). Incredibly, Freud also knew the father’s motive for bringing Dora to see him. He wanted Freud to talk her out of her notion that there was anything more than friendship between him and Frau K.
Caught in this web of lies, deceit, and betrayal, where could she turn? Her situation as it must have seemed to her was cause enough for depression and suicidal ideas. Freud might have said to her, “You are right, and they are wrong.” But Dora had left therapy prematurely; thus it was her fault that she was never cured, that finally, the intelligent, lively girl had earned the epitaph that Deutsch bestowed upon her.
Epilogue: Emma Eckstein and the seduction theory
It is indicative of the enormous influence of Freud’s ideas that today, almost fifty years after his death, they can continue to excite controversy. In 1984 Jeffrey Masson, former projects director of the Sigmund Freud archives, published an account of what he believes is the hitherto unrevealed reason why Freud abandoned his original theory that the etiology of hysteria in adult women was the result of sexual abuse in childhood, often by the girl’s own father. Freud retracted this theory, saying that he had come to realize that these “scenes of seduction,” related to him by his patients, had never taken place, that they were only fantasies that the women had made up. This change in Freud’s thinking was of crucial importance to the further development of psychoanalytic theory; the notion of the fantasized, rather than real, sexual encounter with the parent led to the theories of the importance of childhood sexuality, of the role of fantasy in sexuality as well as in mental life, and of the Oedipal conflicts of childhood, central to Freud’s explication of the psychosexual stages and to their developmental outcomes. The story behind the change is one of the more bizarre in the history of scientific ideas. Unfortunately, it reflects negatively not only upon Freud but upon psychoanalysis in general, which is why it has created so much controversial comment.
By 1895 when Freud and Breuer published Studies in Hysteria, Freud was already convinced that the etiology of hysteria lay in the sexual “seduction” of a child by an adult. Noting that it is more common for girls to experience such assaults, he wrote: “Furthermore, a path is laid open to an understanding of why hysteria is far and away more frequent in members of the female sex; for even in childhood they are more liable to provoke sexual attacks” (Masson, 1984, p. 47). Breuer would not agree to permit the seduction theory to be included in the book, however, probably believing quite correctly that the world was not ready to hear of the frequency of the brutalizing of girl children by their fathers and other adult males. It was not until 1896 that Freud announced his discovery of the causal relationship between sexual abuse in childhood and later neurosis, based upon his psychoanalytic investigation of thirteen cases of hysteria. In none of these cases, Freud said, was sexual assault in childhood missing. He also argued that these stories told by adult women could not be inventive fantasies: “... the memory must be extracted from them piece by piece, and while it is being awakened in their consciousness they become the prey to an emotion which it would be hard to counterfeit” (p. 47).
Freud’s announcement of these ideas met with great disapproval and downright hostility from his professional colleagues in Vienna. Writing to Wilhelm Fliess, a long-time friend, he said: “I am as isolated as you could wish me to be: the word has been given out to abandon me, and a void is forming around me” (p. 36). As Breuer had feared, the suggestion that childhood, a time of joy and innocence, had its darker side of pain and terror and sexual abuse at the hands of those whom children needed to depend upon and to trust was too much for even analysts and psychiatrists to give credence to; thus Freud, for a time, became a pariah—until, that is, he abandoned the theory for one that blamed the child for immoral wishes and fantasies of sexual scenes with the desired adult.
Wilhelm Fliess was a nose and throat physician who was Freud’s closest friend during the years that Freud was formulating his theories of the origins of mental illness. They carried on a voluminous correspondence for many years, and it is Freud’s letters to Fliess that relate the theoretical beginnings of psychoanalysis, including the seduction theory, and reveal the incredible chain of events that caused Freud finally to change his mind.
In February 1895, Fliess performed a nasal operation on a woman whom Freud was seeing in analysis. Emma Eckstein was about twenty-seven when she first came to Freud, suffering from menstrual pain, stomach ailments, and difficulty in walking. Freud believed her to be a hysteric, and his analysis of her revealed that she had indeed been the victim of sexual assault on two occasions by a shopkeeper when she was eight years old. Freud at that time believed that her memories were of real events; it was not until later that he would decide they were fantasies, based on wishful thinking.
Freud discussed the case with Fliess, and it is believed that Fliess suggested that he operate on Emma’s nose to relieve her symptoms. His recommendation was the result of his strange belief that the nose was intimately connected with the sexual organs and that masturbation caused painful menstruation. Since Emma herself, along with many others of her generation, believed firmly in the unhealthful consequences of masturbation, and since both Freud and Fliess believed that masturbation could cause neuroses, the nasal alteration proposed by Fliess seemed appropriate.
Emma developed serious problems after the surgery on her nose and almost bled to death. After a month of severe pain and lifethreatening crises, another surgeon was called in and discovered that Fliess had left a half meter (about twenty inches) of surgical gauze in Emma’s nasal cavity, which had prevented healing and caused her hemorrhages. Finally, in May, after several other procedures, Freud wrote Fliess that she was doing better, though she continued in analysis with him for some time.
Throughout Freud’s letters to Fliess recounting Emma’s ordeal there runs a thread of anxiety, shared by both, that Fliess’s mistake would ruin his reputation as a surgeon. The letters reveal that Freud held strong doubts about the wisdom of the operation in the first place. But his loyalty to Fliess was very strong, and as time went on he began to turn his attention away from the botched operation and the grossly conceived theory that inspired it and to look for the cause of the bleeding in the patient herself. In order to do this, as Masson argues, it would be necessary to build a theory based on hysterical fantasies, whereby the traumas suffered by the patient were inventions. “If Emma Eckstein’s problems (her bleeding) had nothing to do with the real world (Fliess’s operation), then her earlier accounts of seduction could well have been fantasies” (p. 49).
Thus, in 1896, more than a year after the operation, Freud wrote to Fliess that he had an explanation of Emma’s hemorrhages “which will give you much pleasure.... [S]he bled out of longing.... She has always been a bleeder.... [A]s a child she suffered from severe nosebleeds.... [S]he joyously welcomed her severe menstrual bleeding.... Then, in the sanatorium [where she had been taken after the surgery], she became restless during the night because of an unconscious wish to entice me to go there, and since I did not come during the night, she renewed the bleedings, as an unfailing means of rearousing my affection” (p. 49—50). Clearly Freud, concerned about the rejection of his seduction theory, motivated by his wish to exonerate his friend, and, perhaps more importantly, driven by his own guilt feelings (after all, he was the one who had turned her over to Fliess), had rationalized the whole episode such that it was now Emma’s fault that she almost bled to death.
In 1905 Freud publicly retracted the seduction theory: “... I was at last obliged to recognize that these scenes of seduction had never taken place, and that they were only fantasies which my patients had made up” (p. 36).
It is not possible to know with certainty how important was the case of Emma Eckstein in Freud’s abandonment of the seduction hypothesis. In a letter to Fliess in 1897, Freud confided the “gradual dawning” of his disbelief, and gave the reasons for it. One of them was “... the surprise that, in all cases, the father, not excluding my own, had to be accused of being perverse—the realization of the unexpected frequency of hysteria, with precisely the same conditions prevailing in each, whereas surely such widespread perversions against children are not very probable” (p. 53).
In any case, the change in theory had important implications for the further development of psychoanalysis, as noted before. In addition, it had perhaps fateful implications for women who have gone into analysis and who have had their accounts of sexual abuse in childhood treated as fantasies motivated by their own sexual yearnings for their father or father surrogate. Today we know that the sexual abuse of children in its many forms is widespread. Boys as well as girls are used as sexual objects by adults upon whom they are dependent, and the costs in later life of such sexual exploitation are only beginning to be recognized. Freud’s retreat, therefore, from Emma’s pain is more than just an interesting footnote in the history of psychoanalysis. The relationship of real sexual abuse in childhood to neurosis in adulthood is a phenomenon that is still in search of a theory.
Helene Deutsch
Helene Deutsch was born in 1884, in Poland. Like Freud, she received her medical training at the University of Vienna, and in 1918, she spent a year in analysis with him in Vienna. From that time until he left Vienna in 1933, she worked closely with him, and there is no doubt that this association was the single most important influence on her own work. She married Felix Deutsch, Freud’s friend and one-time physician (and consultant to Dora), and had one son. In 1935 she emigrated with her family to Boston. There she lectured at the Boston Psychoanalytic Institute, taught at Boston University, and practiced psychiatry at Massachusetts General Hospital. She presented the culmination of her ideas about women in her two-volume Psychology of Women, published in 1944 and 1945.
Deutsch was truly a Freudian, one of those women analysts who have been called the “dutiful daughters” (Chesler, 1972). Her early papers were concerned with applying his concepts of the libido, the unconscious, and infantile sexuality to female functions such as pregnancy and childbirth. Though her work is within a Freudian theoretical framework, she greatly expanded the classical concepts as they applied to women. Her data were her clinical experiences with women in her analytic practice, case studies, and analyses of works of literature.
In certain important ways, however, Deutsch revised two key Freudian concepts of female personality development: penis envy and the resolution of the Oedipal conflict. Penis envy, while real, is not the basis of the girl’s most essential conflicts, nor does it have a fundamental role in the development of her personality. It is, in fact, a secondary development, growing out of a general tendency to envy, experienced by all children when they observe another child, perhaps a new baby, receiving a great deal of love and attention; or when they see that another child has something of value, and they desire to have it for themselves. Boys experience this more fundamental envy as readily as girls do. When girls express penis envy it is a derivative of the general envy of another who has something one does not have. Some girls, Deutsch observed, even imagine that they have a penis when they are small, but do not need it any more when they are older. The personality trait of envy, described by Freud as a residual of penis envy, is not peculiar to women, said Deutsch.
Freud had assumed that the girl’s abandonment of the mother as love-object in favor of her father was accomplished in early childhood. Deutsch believed, to the contrary, that this detachment is never fully achieved. The role of the girl’s bond with her mother, and its characteristics, are of crucial importance to her personality development. She tests herself in struggles against it, and it forms a base for her own feminine identification. She must eventually free herself; too persistent a tie is restrictive of healthy emotional development. But the shadowy mother in Freud’s system, early rejected by the girl in favor of her robust father, is restored to full and powerful form by Deutsch.
Deutsch’s major work on the psychology of women was written when the Western world was in the throes of the Second World War, and women in large numbers were entering the armed services and working in industry. She considered the effects of this and other social changes on female personality, but she remained unimpressed with the importance of cultural factors as sources of change in the feminine psyche. During the war, women had entered the masculine world out of bitter necessity. Competitiveness, that curse of man, had not really got hold of women, who were dominated by tender and erotic motives rather than by aggressive ones. Certain prototypes of women would always recur, as they always had, perhaps showing different aspects in different cultures; the facade might change, but the feminine core would remain.
Narcissism, passivity, and masochism
Central to Deutsch’s theory of femininity is a triad of personality characteristics: narcissism, passivity, and masochism.
Narcissism for Deutsch means taking oneself as the libidinal object, a loving and valuing of the self. Obviously, this can have both positive and negative, healthy and unhealthy aspects. Healthy narcissism is inherent in self-esteem, self-respect, in caring for the self, independently of others’ opinions. Unhealthy narcissism is an immature concern for the self that requires constant affirmation from others. It is a manifestation of insecurity and inferiority feelings. Both sexes, of course, can exhibit degrees of each kind of narcissism. In women, narcissism may enrich or impoverish emotional life, but in its most helpful form it serves the woman as a protective function, as that mechanism which supports the instinct for self-preservation.
Adolescence brings a resurgence of sexual urges accompanied by anxiety over unfamiliar feelings and body changes. The ego marshals its defenses against such threats, and an important one of these is narcissism. The girl develops a great preoccupation with herself, with her body, her fantasies, her identity. Even her intense relationships with other girls are narcissistic, the ego drawing advantages for itself from its love for the other. By identifying with another, the girl’s ego extends and acquires confidence from the sharing of strength. Healthy narcissism at this age prevents the girl from developing too many identifications, which would interfere with the growth of her own personality. By increasing self-confidence it promotes a strengthening of the ego and a gradual integration of the personal self. Her identity, the “I am I,” emerges.
For Deutsch, passivity is the central attribute of femininity, an attitude of receptive waiting and expectancy. The passive person is one who does not act but is acted upon. She did not heed Freud’s caution that it w’as improper to equate femininity with passivity and masculinity with activity. That very equation is at the heart of her psychology of women, a general principle that she said would always assert itself because of its constitutional origins in the body’s hormones, anatomy, and reproductive functions. The model had its counterparts in conception and in intercourse, when the aggressive male penetrates the passive female. Woman’s greater tendency to identification, her propensity for fantasy, her subjectivity, her inner perception, and her intuition all originate in her passivity. She will abandon her own opinions and tastes, for example, and adopt those of the man she marries. While both sexes fantasize, the male’s fantasies are turned more to reality, to dreams of power and conquering the outside world, while hers are preoccupied with her narcissistic needs and with her relations with others. Such preoccupations determine her other characteristics, her subjectivity and perception which come from her feelings rather than from the objective reality of events, and her intuition, a way of “knowing” in the absence of facts. These tendencies are all passive, compared to their male counterparts of independent identity, fewer, more purposeful fantasies, objectivity, perception based on observable events, and rationality.
This is not to say that women do not behave actively. Indeed, the active mother, engaged in all the tasks of motherhood, is a model for her daughter. Woman’s activity is harmful, Deutsch thought, only if it comes into conflict with the feminine core, in the form of the “masculinity complex,” a protest against acceptance of her feminine self. But her urge toward activity is weaker, and the external inhibitions stronger, than the male’s. Above all, the aggressive components are inhibited. The social environment rejects them, and in compensation offers a woman’s ego a prize, which is love and tenderness. So the girl gives up her aggressions, partly because of her own weakness, partly because of the taboos of the environment, and mostly because of the love prize she receives in return.
Feminine masochism in Deutsch’s thinking must be distinguished from the more familiar model of perversion and neurosis, in that it lacks the components of cruelty, of a seeking out of suffering and pain. In psychoanalysis, masochism means the derivation of pleasure from punishments inflicted by oneself or others. But Deutsch’s usage of the term lacks the pejorative connotations. Masochism as she sees it is a normal condition for women, and normal women show no tendency to inflict pain or suffering upon themselves in the pursuit of pleasure. However, women are more attracted to suffering than men are, and are more likely, in the normal course of their lives, to experience it paired with pleasure. The woman’s willingness to do this is what Deutsch means by masochism. Thus it is adaptive, an adjustment to the realities of her life, in which many of her normal female biological functions involve a combination of pain and pleasure, even joy, such as childbirth. Defloration, the destruction of the hymen in the first intercourse, can be painful, and pain experienced in the sexual act can lead to a connection with submission and gratification. It is to guard against “surplus” masochism, pain as a condition of pleasure, that narcissism is invoked as a defense. Thus viewed, normal femininity involves a balance between narcissism and masochism, the one in the service of the ego, the other, of reality. The healthy woman, then, will accept the discomfort, even pain, associated with her normal functions, because of the pleasure which accompanies them. And always guarding the gates of the ego is her healthy narcissism, her self-love, which will allow her to accept some suffering, but not too much.
Sexuality and the feminine role
Deutsch’s conception of the unfolding of the feminine role is displayed in the subtitles of her two volumes on the psychology of women: Girlhood and Motherhood. The sexuality of the normal woman was in the service of reproduction, and coitus was the beginning of a process leading to parturition. The central problem of the feminine woman was motherhood, a goal and a condition which eventually would absorb all the active forces of her personality.
Human culture had so modified the natural processes of sex and reproduction, separating them from each other, that their psychophysical unity had been obscured. But this unity was preserved in woman’s unconscious, where coitus and childbirth were identified with each other. This relationship was usually imperceptible in normal, feminine women, but sometimes appeared in pathologically distorted forms in disturbed women. The case of Mrs. Andrews was related by Deutsch as an example.
Mrs. Andrews was twenty-nine years old and the mother of six children when she was admitted to the hospital with a number of neurotic symptoms, including fits of anger toward her husband and children. Her greatest expressed concern was an obsessional fear of pregnancy, which had tormented her since puberty. With each pregnancy, she had fought without success for an abortion, had aborted herself a few times, and had even poisoned herself with ergot to bring on her menses. She worked outside the home, forcing her husband to do much of the housework and child care. She associated childbirth with humiliation, saying, “Woman’s most degrading position is on the delivery table, with her feet in the stirrups and men taking charge of her” (1945, p. 100).
The oldest of five children, Mrs. Andrews had been victimized and physically abused by her mother and her mother’s lovers. She had reacted strongly to her mother’s two illegitimate pregnancies, and had early decided that she would never have children. On the one hand, Mrs. Andrews felt an aggressive hatred toward her mother; but on the other, she identified with her, recognizing in herself her mother’s temper tantrums and scornful treatment of her husband. It was this identification, Deutsch thought, that caused her pregnancy obsession. Consciously she rejected pregnancy with an overreactive aversive fear; unconsciously, she desired it.
The unconscious wish to be pregnant, Deutsch believed, appeared in the patient’s requirements for satisfaction in coitus. She compulsively sought intercourse with her husband, even though she did not love him. But she could attain orgasm only at the moment of his ejaculation, when the semen flowed into her body. Orgasm then, was contingent upon the condition of possible impregnation. Thus was the conscious “No” to pregnancy countermanded by the unconscious “Yes,” and in this neurotic woman Deutsch saw revealed what she believed was in the universal female unconscious—the identity of coitus, impregnation, and childbirth.
The case of Mrs. Andrews is presented here because it gives the flavor of Deutsch’s interpretations of female behavior. These, of course, attract the same kinds of criticisms as Freud’s did of Dora. Was this tormented woman unconsciously desiring and arranging her own pregnancies, while consciously repudiating them, pleading for abortions, and expressing her conflict through her numerous symptoms? Or was her fear a realistic sequel to her wretched childhood, leading to an inability to tolerate the female role prescription of the time, further forced upon her by a string of unwanted pregnancies? There is no way to know how much of her psychiatric illness was caused by the intrapsychic conflict described by Deutsch, and how much was caused by her inability, at that time, to control the events of her body. In any case, no epitaph exists to confirm or to invalidate any of the possible explanations, or to tell of her eventual fate.
For Deutsch, the sexuality of women, culminating in the climax of orgasm, was continuous with its natural consequences, pregnancy and childbirth. Unlike the male, for whom the sexual act was discrete, an end in itself, the female experienced orgasm almost incidentally, as a pleasurable sensation which could be described as a vicarious reflection of her mate’s orgasm. Implicit was the notion of adjustment of her sexual activity to his. The expectation of multiple orgasm or of any obligation of the male to bring about sexual satisfaction for the female is absent from her work. Indeed, she termed ridiculous the instruction of “sexologists” that men should heighten their mates’ erotic pleasure by their manipulative dexterity (1944, p. 222).
Years later, Deutsch commented on the high incidence of frigidity in women, and the poor results of psychoanalytic treatment for the condition (Chasseguet-Smirgel, 1970). A severe neurosis could be helped without affecting the problem of the patient’s frigidity. Some psychotic or very aggressive masculine women had intense vaginal orgasms, while feminine, giving, maternal women did not, even though they expressed sexual gratification through intercourse. Also, analysis often revealed anxiety and depression after vaginal orgasms. By contrast, if the vagina remained passive-receptive, the sex act culminating for the woman in mild, slow relaxation, peaceful sleep usually ensued. Since orgasm, then, seemed to be related to pathological conditions, Deutsch was led to suggest that the passive-receptive kind of gratification for women be accepted as normal. If the intense, vaginal orgasm was not experienced by normal feminine women, then it was incorrect to conclude that frigidity was on the increase; rather, the increase was in the demands for a kind of sexual gratification which was not in harmony with the constitutional purpose of the vagina, an organ of reproduction.
Deutsch shared with Freud certain basic assumptions about women, which were based on the facts of women’s anatomy and physiology, and their observable role and function in the society. Since women were biologically equipped to become mothers, and since most did in fact become mothers, such an outcome was the normative base upon which Deutsch built her psychology of women. The active-aggressive components of girlhood were converted to the service of femininity. Some women, such as the matriarch and coquette, channeled their “masculine” aggressiveness into powerful mother or seductress roles, involving activity which was still within the feminine tradition, nurturant and sexual. Others did not successfully integrate the masculine component into the service of femininity. Driven to achievement goals in intellectual or competitive pursuits, their personalities were in constant conflict. Their masculine component, unassimilated and alien, prevented them from accepting the full flavor of their destiny as women. Thus the masculinity complex was clearly a pejorative label, compared to the ideal, an integration of feminine personality and mother role into a harmonious model for womanhood.
Feminists have tended either to dismiss or to attack Deutsch’s views because they seem to follow too closely the Freudian position of biological determination, thus locking women inevitably into roles of self-abnegation and oppression. However, examination of her work and her life together reveals her attempts to reconcile psychoanalytic theory with her own personal experiences and observations. In her autobiography, (hmfrontations with Myself (1973), for example, she tells of her own conflicts in trying to reconcile motherhood with her career in psychoanalysis. But nowhere does she say that she ever considered giving up her career to stay at home with her child. She did, however, point out the pitfalls in trying to integrate motherhood with outside interests, a reality that no mother, feminist or not, would deny. Deutsch’s ideal woman would be mature and self-confident, balancing her many activities with an acceptance of biological functions, including her passive-receptive sexual role. Though perhaps not a model woman from today’s perspective, she is healthier than Freud’s envious masochist, reflecting more clearly Deutsch’s own life with its diverse and active roles (Webster, 1985).
Erik Erikson
Erik Erikson is a contemporary psychoanalyst who was born in Germany of Danish parents in 1902. In 1927, he went to Vienna and with friends started a progressive school for visiting English and American children, some of whose parents were in analysis or were training to be analysts. He became acquainted with Freud and his family, and underwent a training analysis with Anna, Freud’s daughter. He studied clinical psychoanalysis with Helene Deutsch and others who had gathered about Freud in Vienna. He has written extensively about problems of youth and identity, and he has published cross-cultural studies of childhood in American Indian tribes.
In the total context of Erikson’s work, his statements about the psychology of women are not extensive. In fact, like Freud, he was in the seventh decade of his life when he published the paper which represented his analysis of female personality development, “The Inner and the Outer Space: Reflections on Womanhood,” in 1964. Later, in 1975, he returned to the subject, responding to feminist criticism of his views in “Once More the Inner Space.” Though our interest in Erikson concerns mostly these two papers, they should be viewed in the context of his larger contributions.
Erikson’s most widely known book is Childhood and Society (1963). In this work he presented his concept of the “eight ages of man,” the psychological stages of identity development beginning in infancy and culminating in old age, and analyzed some examples of identity development in America, Germany, and Russia. He brought psychoanalytic insight to bear on child-rearing practices of two American Indian tribes and on the sex differences in play constructions of white American children. These were to provide data for his theoretical formulations about women in the 1964 paper. Our major interest in Erikson’s work on identity formation and on childhood lies in those aspects of it that deal with girls and women, and that presumably influenced his later thinking about them.
Psychosocial development: the “eight ages of man”
According to Erikson’s conception of the development of the person through the life cycle, the child passes through a series of phases, each with its own conflict, or crisis, to be resolved. Personality, he thought, develops in accordance with the person’s readiness for successively increasing interactions with society, which in turn invites these interactions, encourages the rate at which they occur and their unfolding in the proper sequence. These stages,[7] and the period in the life cycle when they appear are shown in Table 2.1. The individual progresses, with variations in tempo and intensity, from one stage to the next, meeting and resolving the conflicts associated with each. The quality of the resolutions depends on what is given or permitted by the caretakers, whose offering in turn is affected by social customs and beliefs. Throughout, Erikson is concerned with the effect of society on the developing person, and thus with commonalities of personality which reflect commonalities of experience, as in child-rearing practices, for example.
The study of identity, Erikson said, is as strategic for our time as the study of sexuality was for Freud’s time. Neither, however, precludes the other, as he showed by correlating the psychosocial stages of identity development with their counterpart periods of psycho-sexual development. While the various components of personality are inseparable, different historical periods evoke attention to different aspects of the whole.
Table 2.1 Erik Erikson’s life stages{1}
| Psychosocial stage | Period |
| Basic trust vs. mistrust: learning that the provider of comfort is reliable, consistent, and predictable. | Oral sensory |
| Autonomy vs. shame and doubt: learning to exercise independence and freedom of choice, along with self-control. | Muscular-anal |
| Initiative vs. guilt: undertaking, planning and attacking a task, for the sake of actively doing it. | Locomotor-genital |
| Industry vs. inferiority: developing as a worker and producer. | Latency |
| Identity vs. role confusion: evolving a sense of self that is reliable and consistent, both for oneself and for others. | Puberty |
| Intimacy vs. isolation: readying oneself for a commitment to affiliation with others, and developing the ethical strength to abide by such commitments. | Young adulthood |
| Generativity vs. stagnation: using oneself in the establishment and guidance of the next generation. | Adulthood |
| Ego integrity vs. despair: integrating the earlier stages into an acceptance of one’s own life cycle and an assured confidence in one’s own life style. | Maturity |
Youth and identity
From this theoretical base, Erikson then proceeded to explore problems of identity by analyzing experiences of youth in three countries, America, Germany, and Russia. Although the “eight ages of man” are also the eight ages of woman, Erikson’s examples are all male: in America a certain adolescent “type,” a normal middle-class WASP with a mother, a father, and an older sister; in Germany, the young Hitler, who would become the demonic leader of a nation whose collective identity was ready for him; in Russia, the child Maxim Gorky, who grew up to be a famous writer and idol of the Russian people. Each of these boys had mothers, and Erikson’s descriptions of the boys’ perceptions of them, and how they were affected by them, reveal some of the characteristics of Erikson’s psychoanalytic approach to social phenomena.
The mother of the American adolescent boy is somewhat of a “Mom.” She has an ideal male image which she believes her son can live up to, but she is not overly dominating or protective, unlike a more virulent strain (Philip Wylie, 1942). She is more willing to extend freedom to the boy than the father is, since she is more sure of the kinds of control she has built into him. The authentic “Mom,” however, is also very much on the American scene. She is the one better known to clinicians, who, having been labeled cold, rejecting, or overpossessive, has been identified as the major cause of pathology in the young. Erikson’s discussion of the American “Mom” includes both a description of her personality, which Wylie had earlier provided, and, uniquely, a sympathetic explanation of how she came to be that way:
“Mom,” of course, is only a stereotyped caricature of existing contradictions which have emerged from intense, rapid, and as yet unintegrated changes in American history. To find its beginning, one would have to retrace this history back to the time when it was up to the American woman to evolve one common tradition, on the basis of many imported traditions, and to base on it the education of her children and the style of her home life; when it was up to her to establish new habits of sedentary life on a continent originally populated by men who in their countries of origin, for one reason or another, had not wanted to be “fenced in.” Now, in fear of ever again acquiescing to an outer or inner autocracy, these men insisted on keeping their new cultural identity tentative to a point where women had to become autocratic in their demands for some order (1963, p. 291).
In frontier communities, desperate men fought over her. At the same time she was responsible for culture, religion, and the education of the young. In a time when life style might be either sedentary or migratory, she had to prepare her children for extremes of milieu, for readiness to seek new goals and to compete mercilessly for them. Thus she was in part a product of a historical situation.
In addition to the requirements of a frontier culture, another force in the making of “Mom,” Erikson proposed, was Puritanism, which at first was a system of values “designed to check men and women of eruptive vitality, of strong appetites, as well as of strong individuality” (1963, p. 292). As the country grew older, Puritanism became rigid and defensive, a frigid influence on woman’s tasks of pregnancy, childbirth, nursing, and child training. As fathers abdicated their familial and cultural roles for others in business, technology, and the professions, mothers had to assume^ the paternal role as well. Thus did “Mom” appear on the American scene, to provide a scapegoat for generations of clinicians seeking to explain the peculiar malaise of the American boy.
The older sister hardly figures in Erikson’s account of the American adolescent. Her burden is to become a woman and mother without becoming a “Mom.” Her success depends on region, class, and the kind of man she marries.
Erikson did not offer an analysis of Hitler’s real mother, who hardly figures in his autobiographical Mein Kampf. The prototype German mother, he notes, important as she may be to the children, is obsequious and subservient to the father. The child observes her deviousness, as when she selects certain of his misdeeds to report to the father, depending on her whims. For Hitler, there evolved a two-faced mother image: the loving, childlike martyr of the home, and the superhuman goddess whose hands controlled man’s destiny. She might dispense good or evil, might be generous or treacherous. “This, I believe, is a common set of images in patriarchal societies where woman, in many ways kept irresponsible and childlike, becomes a go-between and an in-between. It thus happens that the father hates in her the elusive children, and the children hate in her the aloof father” (1963, p. 339).
In Erikson’s analysis of the boyhood of young Gorky, it is the grandmother who emerges as the strong, calm, and generous one, who, when she prays, approaches God as an equal, as if He Himself were one of her children who happened to become God. When the boy’s mother left him to marry, the babushka became mother too, a symbol of survival and persistent endurance. “It is as if she had lived long before passions had made men ambitious, greedy, and in turn, childishly repentent; and as if she expected to outlast it all” (1963, p. 367).
Erikson comments on the “diffusion” of the mother role in peasant Russia, whereby the child is mothered by more than one, “women who are at home in this world because ... they make it a home for others. Like the big stove in the center of the house, they can be relied upon eternally” (pp. 367–68). He speculates that such an experience of childhood might make the world more reliable, since the child’s security was not dependent upon one relationship only. At the same time, the utter reliability of the babushka could condition a people who would endure and wait—“so long that reliance becomes apathy and stamina becomes serfdom” (p. 368).
This kind of analysis reveals an essential difference between Erikson and Freud. While both believe in the critical importance of early childhood, Erikson is less concerned with the intrapsychic events described by Freud. Instead, he wants to show how the customs of a society, as they affect what happens to children, result in a kind of shared way of seeing the world, so that, for example, a Hitler can emerge and be accepted by a particular people at a particular time. The “Mom” he describes is not the result of frustrated penis envy, eternally bent upon castrating her sons. She herself is the victim of a confluence of historical trends and events.
Included in Childhood and Society are Erikson’s studies of childhood among the Sioux and the Yurok, two American Indian tribes. Both are male-dominated societies with sharply differentiated sex roles. The boys are trained to be hunters (Sioux) and salmon fishermen (Yurok), and the girls in both cases are trained to be mothers who will bring up hunters and fishermen. As a child analyst Erikson was drawn to study differences in the ways that different societies handled such universal events of childhood as weaning and bowel training, and the effects of these on adult personalities and values. He observed that even trained anthropologists had until recently failed to see that even primitive tribes trained their children in some systematic way—that they did not just grow up like little animals, but were prepared, almost from birth, to assume the role ordained for them in society.
Among the Sioux, for example, the first taboo the child encountered concerned social intimacy between brother and sister. Beginning around age five, the girl was confined to female play, and kept close to the mother and the teepee, while the boy was encouraged to go with the older boys, first for games and later for hunting. Every educational device, Erikson tells us, was used to inculcate selfconfidence in the boy. Trust, autonomy, and initiative, the positive poles of the first three psychosocial stages, were assured him first by maternal generosity and later by the older brothers of the tribe. “He was to become a hunter after game, woman, and spirit” (p. 143). The girl, on the other hand, was trained to be a future helper and mother of hunters. She learned to sew, cook, and put up tents. Along with such practical education, she also learned to be shy, reticent, and fearful of men. She must observe certain boundaries in the camp, and as she matured, she had to sleep with her thighs tied together to prevent rape. Not only was virginity highly prized, but the genitalia must not even be touched by a male if the girl were to retain status as a desirable mate. As a mother, she would teach her children the taboos and responsibilities in the relationships between the sexes.
Cultures, then, “elaborate upon the biologically given, and strive for a division of function between the sexes, which is simultaneously ... meaningful to the particular society, and manageable for the individual ego” (p. 108).
Sex differences and the use of space
At Berkeley, Erikson began to study the play construction of ten-, eleven-, and twelve-year-old boys and girls who were subjects in an ongoing longitudinal study of child development. His method was to invite the children, one at a time, to construct on a table an exciting scene from an imaginary motion picture, using a random selection of small toys and doll figures. He found that the girls tended to build interior scenes, serene and peaceful, of furniture groupings and people and animals in static positions, or doing sedentary things, such as playing the piano. Enclosures consisted of low walls, with gates or vestibules. In some cases, an intruder would cause an uproar, forcing the women in the scene to hide or to become fearful. This intruder was always a man, boy, or animal. Boys, by contrast, erected buildings and towers, and introduced the exciting element of downfall, either causing it to occur or making plain that catastrophe was imminent. Elaborate walls and facades were ornamented with protrusions, such as cones and cylinders. Automobiles and animals moved along the streets.
The spatial tendencies determining these two kinds of productions, Erikson thought, were analogous to sexual anatomy; the males emphasizing erectile, projectile, and active motifs; the females, enclosure, protection, and receptivity (albeit with the ever-present threat of forceful intrusion). He came to believe that this reflection of genital modes on spatial organization was analogous to the sexually different ground plans of the human body, which determined both biological experience and social roles. Later, these data would form the observational basis for his statement on the psychology of women.
Erikson’s paper on the dynamics of womanhood and female identity came when America was well into the space age, and it was an observable fact that the exploration of outer space and all its supporting technology belonged to men. In this paper, Erikson proposes that it is the somatic design of the female body, the inner space of its womb and vagina, that determines the identity formation of women and makes it different from that of men. The anatomical plan of her body signifies a biological, psychological, and ethical commitment to take care of human infancy. The core problem of female fidelity is her disposition of this commitment (1964).
The concept of penis envy, Erikson thought, came about when the first clinicians had to understand their female patients with male empathy, leading them to encourage acceptance of reality, of what is not there. But almost all girls and women know of the existence of their productive inner space, set in the center of the female form. This, he said, is more important than the missing external organ. When the clinician finds his female patient beset with feelings of deprivation, he should not interpret them as evidence of her resentment at not being a boy. Rather, such feelings may emanate from the specific loneliness that women may experience if they fear being left empty and unfulfilled.
Thus the inner space, the locus for her potential for fulfillment, may also be the center of despair:
To be left, for her, means to be empty, to be drained of the blood of the body, the warmth of the heart, the sap of life. How a woman thus can be hurt in depth is a wonder to many a man, and it can arouse both his empathic horror and his refusal to understand. Such hurt can be reexperienced in each menstruation; it is crying to heaven in the mourning over a child; and it becomes a permanent scar in the menopause (1968, p. 278).
Thus is anatomy destiny, as it determines the potentials and limitations of physiological functioning, and, to an extent, personality. Further, it is because of her biological function that the female differs from the male in many empirically validated ways. She is healthier and lives longer because she is the womb of the species and the nurturer of its helpless infancy. Her psychological superiority, compared to males, in tasks involving concentration on details, sensory discrimination, reactivity, docility, and a tolerance for limitations on her activities equips her especially to respond to the needs of others and is a perfect adaptation to her symbiosis with the infant human.
Her unique attractiveness and the kind of man she seeks affect the progress of her identity formation; but the final closure occurs when she selects what will be admitted to the inner space. In the meantime, such resolution may be postponed while she develops as a person, including participation in the world of men. Since she is never not a woman, her special vision may lead to new areas of inquiry and application of knowledge. Her unique contributions might bring about an evolution of society which would include more human adjustments of work to people, and new kinds of social institutions which would use and cultivate the behavioral referents of woman’s inner space: caring, compassion, nurturing, and acceptance.
Who would argue with the merits of such a vision? Surely, the incorporation into the fabric of society’s institutions of such feminine values as these would effect a more benign and less brutal environment for the world’s children. At the same time, it would profoundly change the ground plan of Western technological society. In analogy to Erikson’s own observations on the play construction of girls and boys, a feminine ground plan for society would include the lowering of barriers among people and groups, making peace instead of war, valuing cooperation instead of competition, and attending more to the inner life and less to the outer arena. Though some marginal groups have attempted just such a life style, with greater or less success, it is as difficult to imagine the adaptations of the major institutions of our society to such styles as it is to visualize the forms life might take on another planet.
In recent years Erikson, along with Freud and Deutsch, has attracted considerable negative criticism from feminist writers [8] because of his views on identity development in women. The concept of inner space, while it refers to what woman is rather than to what she is not, still has in common with the concept of penis envy and the feminine core a view of woman which assumes that her unique biology, with all its prerequisites for biological motherhood, uniquely determines, through the indirect mechanisms of identity formation and commitment, her adaptation to life. Thus it shares with the other two theories the flavor of biological determinism which conflicts with feminist ideology.
On other grounds, the relationship between Erikson’s theory and the psychology of women has three major problems. First, his model for psychosocial development and the substance of his work from which it was derived both assume the male as the prototype of humanity. This is not to quarrel with the psychosocial stages themselves, which can theoretically be invoked to explain females as well as males. Rather, the problem is that the model was clearly formulated in terms of a male experiential process which then was adjusted to accommodate women as well. For example, the stage of identity precedes the stage of intimacy. But for women, “the stage of life crucial for the emergence of an integrated female identity is the step from youth to maturity, the state when the young woman, whatever her work career, relinquishes the care received from the paternal family in order to commit herself to the love of a stranger and to the care to be given to his and her offspring” (1968, p. 265). Thus her identity is contingent upon the achievement of intimacy with another, while the male presumably evolves an identity which is independent of that necessity.
In describing the “young adult” of the sixth stage, intimacy versus isolation, he writes: “Body and ego must now be masters of the organ modes and of the nuclear conflicts, in order to be able to face the fear of ego loss in situations which call for self-abandon: in the solidarity of close affiliations, in orgasms and sexual unions, in close friendships and in physical combat” (1963, pp. 263–64). The language of this passage makes it plain that the “young adult” is male.
Further evidence that Erikson’s prototype is implicitly male is the pervasive use of male examples. For instance, as noted earlier in the discussion of youth and identity in Childhood and Society, all the youths are male; women are discussed as mothers, in terms of the ways they influenced the boys’ development. In describing childtraining practices among the Sioux and the Yurok, his major interest is in showing how the Sioux boys grow up to become hunters and the Yurok fishermen. Thus he tells how the cultural system of the Sioux limits itself in “specializing the individual child for one main career, here the buffalo hunter” (p. 156), and how “the Yurok child .. is to be trained to be a fisherman” (p. 176). In both these examples, child means boy. Sioux girlhood is dealt with briefly, as preparation for the future roles of wife and mother; Yurok girlhood is not described.
The objectionable part of all this has nothing to do with Erikson’s observations of male and female identity development or with his portrayals of the impact of society on the quality of childhood; the value and accuracy of these observations are empirical matters which can be validated by research yet to be done. Rather, it is the identification of a theory of human development with a theory of male development, to which female development is then compared. If women are an exception to the theory, then it is not a theory of human development. What the theory does is to provide a background against which women appear as an anomaly.[9] Either separate explanations must be made for her, or she is a silent presence who is lost somewhere among the assumptions underlying the theory.
The second problem is Erikson’s persistent identification of woman with mother. Just as Deutsch’s conception of woman progressed from girlhood to motherhood, so does Erikson see her identity as achieving its closure within the context of marriage and motherhood, with the disposition of the commitment to care for human infancy. This identification is revealed in a discussion of how men and women can transcend their roles, and each partake of the concerns of the other: “For even as real women harbor a legitimate as well as a compensatory masculinity, so real men can partake of motherliness—if permitted to do so by powerful mores” (1968, p. 286). In man, the female principle, if acknowledged, is mother.
Again, the issue is not whether women do or do not achieve identity through motherhood. No doubt a great many women do so, although almost one in five American women never have children (Lopata, 1971). The problem is the emphasis in the theory on women’s reproductive role (which is what the inner space is all about) as the main determinant of identity, thus projecting a bias which cannot possibly account for observable exceptions. If one wishes to maintain that the dynamics of inner space are important even for the exceptions, then one must support the assertion with credible evidence. So far, this has not been done. The matter of evidence leads us to the third problem with Erikson’s theory.
The concept of the inner space developed, as described earlier, from Erikson’s observations of the way prepubescent children make play configurations. Their spatial organization, different for boys and girls, reflected, it seemed, their different genital modes; the one active, erectile, and thrusting; the other quiet, receptive, and protective. Thus the boys were showing a concern for outer, and the girls with inner, space. But while the modes expressed in play were observably different for girls and boys (although one-third of each sex did not conform to the majority), there is no justification for concluding that these differences are determined by, or even related to, sexual or reproductive morphology. A simpler and less far-fetched explanation would rely on what the children had already learned about toys and play, in a society which gives boys trucks, guns, and telescopes, and girls doll houses, dolls, and everything else they need to rehearse them for motherhood. This explanation would also account for the exceptions, since the experiences that children have are more variable than are their anatomical sex differences. Nowhere in Erikson’s description of these experiments does he speak of cultural conditioning as a factor in the play constructions, although he emphasized it elsewhere, as when he told how the Sioux girls were given toys “clearly intended to lead little girls along the path to Indian motherhood” (1963, p. 142), and how they were trained to stay close to home, never to cross certain boundaries, and to maintain a reserved and bashful demeanor. Given such sex-linked differences in socialization it is not possible to know the extent to which innate factors contribute to differences in behavior in later childhood.
In response to his critics, Erikson (1975) returned to the subject of inner space, in a paper which is less a defense than an affirmation of the earlier one. He stated, however, that he should not have written about American identity formation without including its meaning for women. Such oversight, he said, should be corrected by looking at the correspondences between female and male experiences in different periods. Thus the statement that woman is never not a woman corresponds to the statement that man is never not a man; and as women have been limited and unfree in making choices, so have men.
To this unarguable point, though, we should observe that the kinds of “unfreedom,” or bonds which constrain the two sexes are different. Women have been more confined by definitions of what they can do; men, by definitions of how they can be. Specifically, women have been relegated to the social and work roles of wife and mother, with historically relatively recent permissible incursions into occupational roles consistent with the feminine image, such as teaching and nursing. Men, on the other hand, have had much more freedom of choice among occupational roles, and these contribute heavily to their identification and to the kinds of discriminations that are made among them. But ways of being, at least in American society, are more rigidly prescribed for men than for women. The model of masculinity precludes any behavior which is labeled feminine. All traces of the old mother identification must be expunged. Women, however, have more leeway; a girl may revel in her tomboy years, and the active, competent woman is certainly more favored than is the passive, helpless man.
Corresponding to penis envy (which Erikson did not defend in the earlier paper) is man’s anxiety about the worthiness of his organ compared to the competition. And says Erikson, as if this were not enough, he also envies the maternal capacity of the woman. Thus his highest acclaim goes to her for what she can do but he cannot; and his lowest appraisal to any traits of hers which may lurk in his own identity.
As woman has historically assented to an exploitation of the masochistic potential of her roles, to the suffering inherent in them, so has man inflicted on others hardships whose masochistic and sadistic potentials have been disguised as heroism and duty. Thus there are negative and positive elements in the identity development of both sexes, reinforced by the collusion of both, “in both flattering and enslaving each other and themselves” (p. 242).
As a final correspondence, Erikson considers the meaning of two contemporary developments: birth control and arms control, the one going to the core of womanhood, the other to the core of the male identity. As birth control gives women greater role choice, so does arms control imply a liberation of men for roles that are free from the imagery of hunting and conquering. The vision of the future must guide mankind to an order in which chosen children learn to humanize adult inventions. This can come about only “through an equal involvement of women and of their special modes of experience in the over-all planning and governing so far monopolized by men” (p. 247).
From Erikson’s re-examination of his own earlier statement on the development of womanhood, we can come to three conclusions. One, the original statement that the ground plan of the body mediates between instinctual genital and reproductive modes and their manifestation in sex-linked behavior continues to represent his position; two, this is not, however, supportive of any argument that women (or men) should be constrained toward certain roles and not others, or confined to roles on the basis of sex; three, the new society will depend not only upon the willingness of men to lay down their arms, but also upon the involvement of women, with their special modes of experience, in institutions formerly dominated by men.
“Special” means: “1. Having some peculiar or distinguishing characteristic; out of the ordinary, uncommon; particular. 2. Designed for or assigned to a specific purpose; limited or specific in range, aim, or purpose.”[10] Erikson’s designation of women’s modes as special is not pejorative; it simply means that she is still the Other. In her specialness, she will infuse man’s old institutions with her humane values and virtues and presumably guide them toward better solutions for human problems. But the movement that Erikson sees is not unilateral. What about man’s mode of experience, even if it is not special? What does it bode for a peaceful society and its microcosm, the family, the single institution in which women ever prevailed, if only in the overseeing of its domestic arrangement, the care of its children, and the maintenance of its harmony and interpersonal relations? Pursuing Erikson’s notion of correspondence, as women take up roles in the public world, men must take up roles in the private world of home and family.
One is special only within a context, compared to its norms. Women, to be effective in the public world, will need to incorporate some of the more adaptive features of “masculine” behavior into their previously limited range. Men, if they would participate in that world hitherto designated as female, will need to recognize that their mode of experience is special and limited in that context, and that, if they would do at least as well as women have done, they must bring forth and cultivate the residuals of those personality traits usually labeled feminine. The emergence of women and the influence of their special’ experiential modes now seem, in today’s value system, to meet theoretical approval. The corresponding shift for men, and the influence and desirability of their experiential modes, as they adopt role prescriptions previously assigned to women exclusively, has not been explicitly dealt with in the literature. Perhaps the shift for them will be the greater revolution.
These three views of the psychology of women are representative of the traditional psychoanalytic approach to the question. Although they differ somewhat in the concepts they employ, and in the focus of their emphases and the importance they attach to the matter, they have certain characteristics in common.
The first of these is the importance they give to woman’s body as a determinant of her personality and behavior. For Freud and Erikson, the relationship is direct, described in the concepts of penis envy and the inner space. For Deutsch, it is mediated by her mother role, real or potential, which is of course made possible by her unique biology. For all of them, woman is very closely identified with her body and its functions.
The second shared quality of these theories is their invocation of a double standard to explain behavior. The male is seen as the norm, as the prototype human being. His sexual anatomy serves sociosexual behavior with greater dedication than it serves reproductive behavior; in fact, he does not necessarily even recognize the relationship between the two. While his sexuality and its many sublimations may affect behavior, no one advances a theory of male personality which rests on his biosocial role as father, because his role in reproduction is only momentarily important, and he does not typically nurture offspring. The norm is the exemption of the male from these functions, whose relative unimportance in his psychic economy means they cannot have determining effects on his personality. On the other hand, woman, in no way exempt, is in a different class. Since her biology allows her to bring forth young and usually causes her to be assigned the social role of mother, she shares with all women a function and role different from the norm, and this difference is seen as having a profoundly shaping effect on her behavior. Thus the female personality is a deviation from the norm, which is the male, and the deviation is explained on the basis of her biological functions.
In psychoanalytic theories of personality, it is implicit that the model is male. Considerations of the female within such a framework have given rise to conceptual spin-offs which sought to bring her under the theoretical umbrella. But such belated attempts at accommodation prove awkward, both for the general theory and for their specific purpose as explanatory concepts meant to deal with the special case of woman. Furthermore, they highlight the embarrassing lack in traditional psychology of serious and systematic attention to the parameters of “female” behavior, as it appears in the great arc of human behavior.
3. Woman and milieu: innovative views
Now, if we try to free our minds from this masculine mode of thought, nearly all the problems of feminine psychology take on a different appearance.
—Karen Horney, “The Flight from Womanhood,” 1926
Psychoanalytic theory and its derived views of female personality and sexuality attracted considerable scholarly evaluation and criticism, and several of Freud’s colleagues and intellectual heirs abandoned the orthodox position he represented and set forth theories of their own. Of particular interest to us are those whose innovative approach included new interpretations of woman’s behavior, her feminine personality, and her experiential history.
Although there was no dearth of criticism of psychoanalysis among the ranks of its early practitioners, almost none of them made the problem of female personality and sexuality, or even of male-female differences, central to their thinking. Few viewed it as a fundamental question of the human experience. However, a few theorists did provide a new direction for thinking about women. Among them were Karen Horney, Clara Thompson, and Alfred Adler, psychoanalysts who took particular exception to Freud, reinterpreting his observations from different perspectives.
Researchers in other social science disciplines as well provided data which led to changes in understanding of human experience, and of concepts of femininity and masculinity. One of the most prolific of these is Margaret Mead, a cultural anthropologist whose observations of non-Western cultures demonstrated decisively the malleability of human behavior.
Although they differ in their theoretical positions—and Mead in her methodology and the nature of her data—they share an appreciation of experiential and cultural influences in the shaping of personality and behavior. The three psychoanalysts set up systems of thinking about human behavior which departed radically from classical Freudian views and Mead showed to students of the individual the importance of the commonalities that one shares with all others within a culture. Among them, they made possible a more balanced approach to the scientific study of women and men.
Karen Horney
Karen Horney was born in 1885, almost thirty years after Freud, and grew up under very different circumstances. Though it was unusual for a woman to become a physician, she was encouraged by her independent mother to attend medical school in Berlin, and later to seek training there in psychiatry and psychoanalysis.
Her training was in classic psychoanalytic theory, under two Freudian analysts, Karl Abraham and Hanns Sachs. Horney began her confrontation with the basic tenets of psychoanalysis in her first published paper, “The Technique of Psychoanalytic Therapy.” “Psychoanalysis,” she wrote, “can free a human being who has been tied hands and feet. It cannot give him new arms or legs. Psychoanalysis, however, has shown us that much that we have regarded as constitutional merely represents a blockage of growth, a blockage which can be lifted.”[11] While not doubting the importance of the unconscious and of early childhood experiences, she thought that the person could be understood only by considering also his or her interaction with the present environment. Constitutional factors were not fixed and unilateral determinants, but were possibilities which would be shaped by this reciprocal interaction. Thus Horney defined her approach as holistic, a view of the person as a dynamic whole, in contrast to the nineteenth-century psychoanalytic theory which tended to view the person as a mechanistic system of parts whose operations were relatively independent of other variables.
Having shifted her philosophical base away from biological determinism, Horney began to develop her interest in feminine psychology. Between 1923 and 1935, she published a series of papers in which she critically examined Freud’s theories of the libido and the psychosexual stages of development as they were alleged to affect women (Horney, 1973). In Horney’s later work, these formulations became incorporated into a psychology of the whole person regardless of sex which showed how human growth, or its obstruction, came about through the intimate interplay of the person and the changing environment.
Horney’s method of investigation, like that of Freud and Deutsch, was based on clinical observation of patients. From the data of such observations, hypotheses might be formed, which could then be tested in further practice. She insisted that the explanatory statements of psychoanalysis be confirmed by actual observation in behavior. This rigorous attitude was an important factor in her critical approach to Freud’s ideas about women. For example, in a discussion of his hypothesis of penis envy she cautioned that it is an hypothesis, not a fact. Furthermore, the claim that it is a primary factor in the early lives not only of neurotic females but of all females is unsubstantiated by data. “Unfortunately little or nothing is known of psychically healthy women, or of women under different cultural conditions” (1973, p. 216).
An important reason for the dearth of knowledge about women, Horney said, was the male bias of psychoanalytic observers. In “The Flight From Womanhood” Horney supported the point that in our civilization all its institutions were dominated by men. The concept “human being” was identified with the concept “man.” The psychology of women evolved from a male point of view. In this paper, written only one year after Freud’s first paper on the psychology of women, Horney expressed the belief that the masculine bias of psychoanalysis reflected an earlier time when only masculine development was considered and when the evolution of women was measured by masculine standards. To show this influence in the existing analytic picture of feminine development, she compared the ideas that young boys have of girls with analytic ideas of feminine development (1973, pp. 57–58):
| The boy’s ideas | Analytic ideas of feminine development |
| Naive assumption that girls as well as boys possess a penis. | For both sexes it is only the male genital which plays any part. |
| Realization of the absence of the penis. | Sad discovery of the absence of the penis. |
| Idea that the girl is a castrated, mutilated boy. | Belief of the girl that she once possessed a penis and lost it by castration. |
| Belief that the girl has suffered punishment which also threatens him. | Castration is conceived of as the infliction of punishment. |
| The girl is regarded as inferior. | The girl regards herself as inferior. Penis envy. |
| The boy is unable to imagine how the girl can ever get over this loss or envy. | The girl never gets over the sense of deficiency and inferiority and has constantly to master afresh her desire to be a man. |
| The boy dreads her envy. | The girl desires throughout life to avenge herself on the man for possessing something she lacks. |
Reprinted from Feminine Psychology by Karen Horney, M.D., edited by Harold Kelman, M.D. (Copyright © 1967 by W. W. Norton & Company, Inc.)
Such a “remarkable parallelism,” she proposed, might be an expression of the fact that observation of feminine development had been made from a male point of view.
Horney then re-examined the Freudian concepts of penis envy, the masculinity complex, and basic inferiority feelings in women. She did not deny the prevalence of these qualities in women. She argued, however, against the importance that Freud ascribed to them in the case of women and his designation of such traits to women only. While a young girl might openly display penis envy, this was not necessarily a manifestation of a deep instinctual need which would persist into adulthood and color her whole life. Furthermore, the masculinity complex was not, as Freud had said, an unresolved form of penis envy, but rather a “flight from womanhood,” occurring in some cases when the girl, forced to renounce her libidinal wishes toward the father, abandons the feminine role altogether. Adopting a masculine attitude, she uses the “fiction of maleness” to escape from the female role and the guilt it holds as a result of the libidinous wishes. But the penalty must be feelings of inadequacy and inferiority. Deviating from her norm to that of the male, she must apply to herself values and pretensions that are biologically foreign to her, and must inevitably see herself as inadequate.
Nor is it only women who consciously or unconsciously envy the attributes of the other sex. Horney drew attention to the intense envy in boys of the events of motherhood: pregnancy, childbirth, and the act of suckling, as well as of the breasts themselves. The sense of this clear biological superiority of the woman is so strong that the recognition of it must be kept from consciousness. Thus it is early repressed, and is kept repressed by transforming it into its more palatable opposite: a conviction of her inferiority, fed by a need to depreciate her, as if the denial of her worth would magically negate what he knew to be true. The fact that the femininity complex in males is seen less frequently than is its counterpart in females, Horney said, is because males have more opportunity for achievement in the world of work and creative activity than females have. Thus the great creative productivity of males can be seen as a compensation for their inability to create life. This view is quite different from Freud’s idea that all the masculine achievements of civilization are a result of the requirement for the modification and rechanneling of the basic sexual energy, the libido.
Horney presented one of her strongest arguments for a consideration of cultural factors as major influences in the psychology of women in “The Problem of Feminine Masochism,” published in 1935. Deutsch had already published her views on masochism in women, which had grown out of Freud’s idea that clitoral sexuality had to be suppressed in the interest of the primacy of the vagina in mature femininity. Both Freud and Deutsch assumed a biologically determined relationship between femininity and masochism. Deutsch believed it was a basic drive in the mental life of women. It represented a directing inward toward oneself the active-aggressive drives associated with clitoral sexuality, a renunciation which occurred when the girl discovered the inadequacy of her organ compared to the male’s. The events of sex and reproduction, with their potential for pain and suffering, could provide masochistic satisfaction. Since classical psychoanalytic theory held that general behavior patterns were modeled on sexual behavior patterns, it followed that women, masochistic in their attitudes toward sex and reproduction, would also reveal such trends in their nonsexual approach to life. Therefore masochism was normal for women, who would manifest it much more frequently than would men. In men, in fact, it was a manifestation of feminine qualities.
Horney’s argument with this view was not whether a masochistic derivation of pleasure from pain is found more often in women than in men; rather, she doubted that its occurrence was psychobiologically necessary. While it might be observed in many neurotic women, she was unconvinced that most women would lastingly be driven to seek suffering as a consequence of the early genital trauma. “A living organism, when hit by some traumatic event adapts itself to the new situation” (1973, p. 221). The one-sidedness of the prevailing views, she said, came about because of the exclusion of cultural and social factors from the picture. As an example, she noted that Russian peasant women during the Tsarist regime had sought beatings from their husbands as proof of love. But lest one take this as evidence of innate masochism in women, one must note the emergence of the modern Soviet woman, who would hardly view beatings as signs of love. “The change has occurred in the patterns of culture rather than in the particular woman” (1973, p. 224).
Insisting upon the necessity for careful investigation, Horney suggested that cross-cultural research would show whether such traits as masochism were in fact inherent in the feminine personality. For example, anthropologists could examine different cultures for observable masochistic attitudes: inhibition of assertiveness, seeing oneself as weak and helpless and expecting advantages on account of this, becoming emotionally dependent on the other sex, tending to be self-sacrificing and submissive, and using weakness and helplessness to subdue the other sex.
All of these attitudes came out in psychoanalysis with masochistic women, and because of their ubiquity in Western society, had been used as evidence of biological causation. But here, as she had with penis envy, Horney pointed to cultural factors as causative agents, and said that she would expect these masochistic behaviors to appear in any culture which included for women:
-
blocking of outlets for expansiveness and sexuality;
-
restrictions on the number of children, when childbearing is the measure of a woman’s value;
-
estimation of women as inferior to men;
-
economic dependence of women on men;
-
restriction of women to roles that are built on emotional bonds such as family, religion, and charitable works;
-
surplus of marriageable women, facilitating emotional dependence on men and sexual competition with other women.
When these elements are present, Horney pointed out, then there appear ideologies about the “nature” of women, such as that she is weak, emotional, and poorly suited for autonomous and independent activity. Such ideologies serve to reconcile women to their subordinate role, to identify it with their hope of fulfillment, and to define it as desirable. Strengthening the influence of such beliefs is the practice of men in choosing women who have such traits. If she is to be chosen, she must conform to the image believed to be the true nature of woman. Given the powerful influence of such factors, and their prevalence in our culture as well as others, few women can escape becoming masochistic to some degree, without any contribution by anatomical factors. Beyond admitting the masochistic potential of woman’s traditional role in sex and childbearing, any other assertion of an inevitable relation of her constitution to masochism is only hypothetical.
The ideas that Horney formulated during her years of interest in female psychology became part of her general theory of the whole person, first presented in The Neurotic Personality of Our Time, (1937). She had rejected Freud’s libido theory, with its emphasis on biological instincts and drives, and its pessimistic view of man as a driven
creature at odds with himself and his world. Instead, she saw the child as born with a potential for growth, for self-actualization which could be facilitated by a healthful environment.
The basic principle motivating human behavior was not the instinctual dyad of sex and aggression, but the need for security. The child whose emotional needs were regularly and consistently met would experience a harmonious development, in the course of which his or her own capacities would unfold. The insecure child, sensing the world as a hostile place, would develop a feeling of basic anxiety, of isolation and helplessness. To cope with these feelings, the individual in the course of growth would develop various strategies for dealing with other persons. In general these strategies, motivated by the person’s anxious needs, fell into three categories: moving toward people, moving away from people, and moving against people. In the normal person, these ways of relating are balanced and integrated in the personality, and are not in conflict with each other. The insecure person, however, is driven to exaggerate one or the other of these adaptations, becoming over-compliant and docile, over-withdrawn and isolated, or over-aggressive. Each of these “solutions” to the problem of anxiety is unsatisfying because it restricts the person’s growth and engenders self-hate and impoverished relations with others.
By the time Horney wrote her last book, Neurosis and Human Growth (1950), she had broken completely with the Freudian school of psychoanalysis. Against the Freudian view of man as a creature born to conflict, whose best accomplishments in love and creativity were at the cost of renunciation of his basic instincts, she set her own vision of the person, whose best energies are affirmative strivings toward knowledge, toward developing spiritual powers and moral courage, toward achievements in all areas, toward the full use of intellect and imagination. “Albert Schweitzer uses the terms ‘optimistic’ and ‘pessimistic’ in the sense of ‘world and life affirmation’ and ‘world and life negation.’ Freud’s philosophy, in this deep sense, is a pessimistic one. Ours, with all its cognizance of the tragic element in neurosis, is an optimistic one” (p. 378).
Clara Thompson
Born in Rhode Island in 1893, Clara Thompson planned to become a medical missionary. She abandoned this goal before going to medical school at Johns Hopkins, where she became interested in psychiatry and psychoanalysis. Between 1928 and 1933, she underwent psychoanalysis with Sandor Ferenczi, a Hungarian member of Freud’s inner circle, who had already begun to move away from Freudian orthodoxy. In addition to Ferenczi, those who influenced Thompson most were Karen Horney and Harry Stack Sullivan. Sullivan, educated in the humanist tradition of American psychology, rejected the classical mechanistic view of human personality in favor of an interpersonal approach which saw the nature of the person’s relationships with others as central to adjustment and well-being.
The basic difference between Freudian psychoanalysis and interpersonal psychoanalysis is in their different views of personality development. Freud’s instinct theory of the libido, the basic sexual energy, pictured development as a grim struggle against the primacy of savage instincts. Out of this battle emerged man’s character, his conscience, and his creativity. The interpersonal school assumed as the basic drive the need to grow and to master one’s environment. This meant learning the pattern of one’s culture, its speech, customs, and taboos. The human becomes a product not of the renunciation of libidinal urges but of interactions with significant persons around him or her. Humans are the least instinct-dominated of all animals, and psychoanalysis should be concerned with the social forces which dominate human behavior.
The central feature of early childhood development was not the successful negotiation of libidinal stages but the formation of the self and the emergence of an identity separate from that of the mother. The child goes through a series of stages, involving varying and increasingly mature kinds of interactions with others. In infancy, the most important relationship is with the mother. Through their interaction he learns of his separateness and establishes a basis for communion and empathy with others. In childhood and the juvenile era, the beginnings of cooperation and competition develop through playing with others. Sex is not an important component of the child’s growth. During preadolescence, the normal child learns to care about the happiness of others and to form close bonds with peers. Only in adolescence does sex begin to become important. It is not a problem in itself. It is the cultural attitudes about sex that make this a hazardous time, since the social restrictions make it difficult for the adolescent to gratify sexual urges. Maturity is achieved when the person is able successfully to form a durable and intimate relationship with another person. Thus personality development is a process of acculturation, and it is not dominated by the requirement to repress and to transform the sexual energy.
In “Cultural Pressures in the Psychology of Women” (1942) Thompson responded to Freud’s view of female personality as an inevitable result of her original biological inferiority. She showed how penis envy and all its derived personality traits—jealousy, feelings of inferiority, weak superego, prematurely arrested development, and rigidity—could be explained by a theory of cultural causation, as adaptations to the lives women lead in Western society. The penis, she said, is a symbol of privilege in a patriarchal society, and it is this privilege that women envy in men. Women do not, as Freud thought, want a penis for themselves. Penis envy in the Freudian sense is not universal, and is not found in normal women. Jealousy and envy are traits characteristic of a competitive culture, which implies comparison of one group with another usually to the disadvantage of one of them. The restricted opportunities available for women, and the limitations placed on her development and her independence, are real bases for envy which have nothing to do with neurosis. Likewise, women’s feelings of inferiority are a reflection of their real position in the society and not of a biological lack as Freud thought. Women’s weaker superego, or the lack of internalized standards, is typical of those whose security depends on the approval of a powerful person or group. The Victorian girl, for example, protected and dependent on her father, had insufficient opportunity to develop a mind of her own. It would have been dangerous had she done so because it would have interfered with her adaptation to her future husband. The weak person must adopt the ideology of the strong one in order to survive.
Freud had further pointed out that women lose their ability to grow emotionally and intellectually earlier than men do, and that they become rigid in their beliefs and attitudes. The woman of thirty, he said, seemed inaccessible to influence for the future, while a man of that age was at the beginning of his growth to peak maturity. Thompson countered that as long as a woman’s sole achievement was in marriage and motherhood, her career was made or lost by age thirty. In Freud’s time, as well as in the mid-twentieth century, a woman of thirty had no future. Yet psychoanalysis itself held that in order for therapy to be successful, actual opportunities for further development must exist. This alone would explain the cessation of growth in women, and their greater rigidity, if in fact these could be demonstrated to affect women more than men. In reality, stunted and rigid men of thirty were not scarce. Given unfortunate life situations or lack of training, a narrowed outlook and early rigidity were predictable for anyone regardless of sex.
Thompson did not dispute Freud’s observations of his women patients. What she did argue with was the inadequacy of his interpretation of those observations, resulting from two errors in Freud’s thinking. First, he saw female development from a masculine point of view. The woman was the negative of the man, and her childbearing function was a compensation for the missing penis. Was not, Thompson asked, this function important in its own right? Second, Freud studied women only in his own culture and believed that what he saw in them was universally true for women. Freud was analyzing not “natural” women but women in a patriarchal society. Assumption of women’s inferiority was a prevalent attitude accepted by both sexes as a biologic fact. Men would not only have an interest in believing this because of its obvious advantage to them, but would share with women the difficulty of freeing themselves from an idea which was part of their earliest training and permeated the whole society.
Thompson also considered some alternate explanations for the masculinity complex which Freud thought to be a refusal of the woman to accept her “castration.” The culture, she said, invites masculinity in women. As women move out of the old sheltered role in a restless search for a better life, they tend to adopt the behavior of those who are already successful. Having no models of their own, they copy men because the world rewards masculine behavior. In a male domain, created and maintained by men, the so-called masculine traits of decisiveness and daring lead to greater achievement than do gentleness and submissiveness. When women behave this way, it is not necessarily a sign of pathological character development.
In a later paper on working women, Thompson (1953) returned to the problem of woman’s conflict between being the way she is and feeling that she must adopt male values and behavior in order to be able to achieve anything of importance in the world outside the home. She cautioned against believing that one must behave like men in order to succeed. Women must find their place in the social order without feeling that they must compete with men in a system created by men. When women wanted to become free, they took as their blueprint the masculine pattern, as there was no other. Perhaps it would be better if women found their own pattern, remembering that the competitive race for success does not enrich the lives of those trapped in it. Tentatively, she suggested that women might lead in bringing about a change in the cultural attitude toward competition.
Thompson also drew attention to the effects of attitudes toward female sexuality on woman’s self-perception and self-esteem. In 1950, she presented a paper which examined the derogatory attitude that women’s sexual needs were unimportant. This attitude arose because women did not have obvious evidence of erotic excitement as men did, and because the prevailing morality, a residual of Victorianism, encouraged a denial of pleasure in the sexual act. Woman was not supposed to be erotic, but she must participate in sex at any time. Since man must have his satisfaction, the wife must be available whether she partipates actively or not. Thompson felt that such derogation of her sexuality generalized to a devaluing of herself as a person. If a woman’s sexual needs and interests were relatively slight, then the male could use her as an instrument for his pleasure and gratification without much concern for her feelings. Given the puritanical flavor of attitudes toward the body and sexuality, woman, being invested as standard-bearer of morality and virtue, could least of all risk censure by expressing interest or making demands in the sexual area of her life.
What Thompson was rejecting was the notion that woman, her body, and her functions were inferior. She felt that woman’s concurrence and her own depreciation of herself and her sex was a result of the social roles that man wanted her to play. Thus Freud was describing women who were the result of these social conditions, while Thompson emphasized that these social conditions were the cause of women’s behavior.
Alfred Adler
Alfred Adler was born in Vienna in 1870. By 1895, he had begun to practice general medicine. Adler had already become interested in psychopathology through his own practice and through reading the works of Charcot and others. After Freud published Interpretation of Dreams in 1900, the two met, and Adler became one of the charter members of the Vienna Psychoanalytic Society. By 1911, it became apparent that Adler’s views were at odds with Freud’s, and the disagreement culminated in Adler’s resignation from the Society. Adler believed that Freud’s insistence upon strict adherence to his views was an infringement on freedom of scientific investigation, and he began work on a new approach to personality, which came to be known as Individual Psychology.
Adler’s Individual Psychology differed in a number of important ways from Freudian psychoanalysis. He rejected Freud’s assumption that behavior is motivated by biologically determined instinctual urges that are primarily sexual in nature. Adler believed that the human is primarily a social being motivated by social interests and relating to others through cooperation in work for the common interest. The individual acquires a style of life which is identified by his or her interactions with others.
Perhaps most important, Adler reinstated conscious thought processes to the role of greatest importance. Where Freud had presented the pessimistic view of the human as being at the mercy of unconscious forces which had their pathological roots in the events of early childhood, Adler taught that people are ordinarily aware of why they do what they do. He said that most of us know what our goals are and what our limitations are in striving for them. Furthermore, we can plan our behavior knowing what it will mean for the realization of our selves.
Adler believed that individuals are motivated more by their expectations of the future than by their experiences of the past. Thus they develop fictional goals, which are beliefs about present or future events. These beliefs have a regulatory effect on behavior, and cause the person to behave consistently in situations relating to the belief. For example, the person might hold to such ideas as “every man for himself,” “honesty is the best policy,” or a belief in a life after death which will reward the virtuous and punish the wicked. It is reasonable to assume that such beliefs would have an effect on the person’s behavior. Here, Adler seems to be recognizing the importance of a personal ideology which serves as a general guide for behavior. These beliefs consist of goals toward which the person strives in her or his attempt to maintain consistency between behavior and belief. This tenet of Adler’s system was in total opposition to Freud’s emphasis on the past with its deterministic grip on the future. Even if the goal did not in fact exist, Adler held the belief in its reality would motivate behavior, just as surely as if it were real.
Early in his medical career Adler became interested in the idea of organ inferiority, the tendency of a person’s illness to focus on a certain organ system. He noted that sometimes the afflicted one attempts to make up for such an inferiority by developing unusual strength in that particular area of functioning. For example, a person who had a muscular weakness from childhood might exercise especial diligence and become a skilled ballet dancer. Adler later broadened the concept of inferiority as a motivating force to include not only biological but psychological sources. In normal persons feelings of inferiority were part of the experience of everyone, issuing from the universal helplessness of the infant. Thus behavior was motivated by a need to overcome this basic inferiority, to attain ever greater development and growth of the self.
The innate principle that Adler thought was basic to human growth was a striving for superiority. By this he meant not dominance, leadership, or an important position in society, but a striving toward completion of the self and toward an actualization of the best that one could be given one’s goals and the exigencies of one’s life. It is this striving that carries the person from one stage of development to the next. The neurotic may strive for power, or for other selfish goals, but the normal person strives for goals that are in the service of social interests. It was in this connection that Adler introduced the concept of “masculine protest” or an overcompensation that both women and men may show when they feel inadequate. The compensatory behavior takes the form of an exaggeration of masculine qualities.
By social interest Adler meant the individual human’s investment of self in the interests of the larger society. Thus it includes the willingness of the individual to cooperate with others to achieve common goals, to form interpersonal relations and to identify with the group. Alone, the person was weak; social interest was a compensation for the impotence of the individual. Adler saw this characteristic as an innate disposition which, like other potentials of the person, would fully develop with proper care and guidance.
Adler’s theory of personality, in contrast to Freud’s, was an affirmative statement of trust in human potential and of one’s ability to choose, to order, and to influence the course of one’s life. Thus it restored a certain freedom and dignity to personhood, and held out the hope that humankind could fashion the good life for the individual and for the society. Like Horney, Adler was optimistic.
Adler’s ideas about women followed directly and logically from his theory of personality. In fact, the key concepts of his theory seem unusually fitting as useful explanations of some aspects of the so-called feminine personality. For Adler, the only biological fact of any importance was the helplessness of the human infant. From this condition issued universal feelings of inferiority which motivated the compensatory striving for power. These strivings, when accompanied by social interest and common sense, all attributes of the normal human, were channeled into achievement behavior directed toward a goal. If the child were dealt with intelligently and sympathetically, the healthy personality would develop naturally, because of the innate capacity to do so. If the child’s inferiority feelings persisted, because of parental failure to encourage compensatory striving, or if the child were neglected or permitted to become selfish and spoiled, then she or he would fail to develop adequate coping power and would find “erroneous” solutions to life’s problems. Adler believed that the system of socializing children into roles of dominance and submission based on sex had all the potential for inducing bad solutions in the form of neuroses and character distortions. For example, the boy is forced into an unnatural requirement for domination, a behavioral pattern which depreciates the female sex. The girl, in addition to the feelings of inferiority shared with all young children, has the added consciousness of her sexual subordination. The twin fallacies of the superiority of the male and the inferiority of the female erode the erotic and social relationships between the sexes, and result inevitably in hostility and suspicion at the expense of comradeship, trust, and candor.
Adler believed that the girl loses self-confidence as she continually experiences prejudices against women. She is routinely thwarted in acting out a basic drive for power and superiority common to all humans. Her sex category determines the way she is treated by society, and that treatment must cause disturbance in her psychic development. “The whole history of civilization ... shows us that the pressure exerted upon women, and the inhibitions to which she must submit today, are not to be borne by any human being; they always give rise to revolt” (Adler, 1927, p. 134).
As evidence that the female’s diminution of self-esteem is conditioned early in life, Adler cited research showing that daughters in families where the mother was the sole breadwinner were more talented and capable than girls in families where the mother’s role was subordinate to the father’s. Because of the model of competency presented by the mother, they failed to develop negative concepts of themselves as women.
Adler called attention to the division of descriptive concepts along sex lines, whereby “masculine” means worthwhile, powerful, and capable, and “feminine” means obedient, servile, and subordinate. Traits valued by society are masculine, and those less valued are feminine. Whatever pertains to women appears inferior, so that both women and men depreciate the female sex.
The psychic life of women, Adler said, is deeply affected by the imposition of this additional ascribed inferiority. Many girls and women End compensation in certain privileges accorded to them because of their sex such as special courtesies and exemptions from some kinds of obligations. While these may seem to elevate women, it puts them in a position which has been designed by men for the advantage of men.
The almost universal dissatisfaction with the feminine role may manifest itself, Adler thought, in three ways, all of which are distortions away from healthy personality. The first type develops in an active “masculine” direction. In this case the woman seeks to compensate for her inferior status by revolting against it. This is the “masculine protest” which both males and females adopt when they feel inferior. They are trying to purge themselves of the dreaded weakness of femininity. Adler seemed to think that given the situation, such a protest in women was predictable. Since there were only two socially approved types, the ideal woman and the ideal man, desertion of the female role could only appear masculine. “This does not appear as the result of some mysterious secretion, but because, in the given time and place, there is no other possibility” (p. 134). The second kind of rebellion appears in the woman who over-identifies with the feminine role, cloaking herself in resignation, humility, and obedience. She adjusts everywhere because of her docility, but is so helpless and weak that she accomplishes nothing. She develops neurotic symptoms, showing clearly how her “training” has made her sick. A third woman may accept the condemnation of inferiority and of subordination, and feel convinced that these sentences on women are just. She believes that men are entitled to their position of privilege, and that only they can do the important things in life. Her indirect way of revolting takes revenge by shifting all responsibility onto the male, as if to say, “Since only you are competent, you must do everything.”
One can see certain similarities between Adler’s first two types and Freud’s women who developed neurotic solutions to their penis envy, but only the behavioral styles are similar. Adler refused to consider a constitutional determinant at all. He saw all these forms of protest as the result of man’s privilege and woman’s powerlessness and not a result of biology. While men were also hurt by their social conditioning for dominance, Adler implied that women could be expected to suffer more because as children they had to bear a double load of inferiority feelings from their status as child and their identity as female. Adler believed that it was normal for all humans to strive for superiority and that women who did so should not be considered deviant.
Adler’s understanding of the factors underlying female behavior and personality led him to conclusions which were strongly supportive of the prevailing feminist positions on social reform. He deplored the competitive pressures of the educational process, which forced boys to prove their masculinity and taught girls to be victims. He thought that the prejudices against women, and the emphasis on roles, pushed many girls toward marriage as an “emergency exit out of life,” and led to marital problems and increased tensions between the sexes. He deplored the inequality of sexual standards. “A subordination of one individual to another in sexual relationships is just as unbearable as in the life of nations” (p. 145).
Leta Stetter Hollingworth
One of psychology’s foremothers, Leta Stetter Hollingworth differed from Horney, Thompson, and Adler in some important ways. They were all physicians subsequently trained in psychoanalysis, whose major contributions were to theory and clinical practice. Hollingworth, by contrast, was an academically trained psychologist who specialized in developmental child and educational psychology. Her intellectual roots were firmly planted in scientific research as it was applied to psychological investigation in the first few decades of this century. Her own contributions to psychology were based not only on clinical observation but also on laboratory experiments, using such designs and statistical methods as were available at the time. Thus she is the first psychologist whose ideas and studies relevant to the psychology of women we have considered.
Hollingworth was born in 1886 in Nebraska, in an environment of “sod houses, long-horned cattle, and roving Indians” (Poffenberger, 1940, p. 301). She was educated in a one-room log schoolhouse until she entered the University of Nebraska at the age of sixteen. After graduation she taught high-school English for two years, resigning to be married. Her husband was in the psychology department at Columbia University, and it was there that Hollingworth received her doctorate and spent the rest of her professional life.
In her early years in New York, Hollingworth was an active feminist and a member of the Women’s Suffrage Party, which worked for the ratification of the nineteenth amendment to the Constitution, which would give women the right to vote in 1920. She marched in suffrage parades and spoke on behalf of women’s issues, lending the credibility of science to the women’s movement (Russo and O’Connell, 1980). Her interest in political equity for women was reflected in her pioneering work in the psychology of women. She researched and wrote in areas that were highly pertinent to the psychology of women as it was structured at the time. Of even greater importance, she was one of the few who insisted that scientific methods, not beliefs in the service of social values, must be used to study social issues such as women’s opportunities and achievements and their roles in the society. Accordingly, she designed and carried out an experiment to test the widely held belief that women’s performance was impaired during their menstrual periods; she challenged the popular variability hypothesis (see Ch. 1, p. 14), which held that men varied more from the mean than women did—thus more men than women would be geniuses as well as mental defectives; and she analysed social mechanisms that functioned to impel women to bear and rear children.
Hollingworth’s doctoral dissertation was an experimental study of the mental and motor abilities of women during menstruation. She undertook the study, as she said, because there were no scientific studies of behavior across the menstrual cycle. Medical literature of the time, however, was rich with assertions of the malignant effects on women of the menses. For example:
Even though scientific experiments are as yet lacking, it may nevertheless be stated that a very great number of healthy women are mentally different during menstruation.... Thus woman needs protection during menstruation. All demands on her strength must be remitted. Every month for several days she is enfeebled, if not downright ill (qtd. in Hollingworth, 1914a, p. 2).
Hollingworth’s experiment involved comparing the performances of women and men on several mental and motor tests over a three-month period. She found that the women not only did as well on the tasks during their menstrual periods as at other times of the month, but that they did as well as the men did overall. While her methodology is flawed by today’s standards, the value of the study lies in its unique insistence upon substituting science for cherished beliefs about the effects of women’s bodies upon their behavior. Finally, she confronted directly the use of dogmatic beliefs about such effects to deny women political freedom and educational and employment opportunity (Hollingworth, 1914a).
In the first decade of this century, the variability hypothesis was supported by several eminent psychologists who saw in it a perfectly logical explanation for the observable overrepresentation of men among the highest achievers in the society as well as among persons in institutions for the mentally defective. The variability hypothesis rested upon the notion that human characteristics, both mental and physical, are distributed like the normal curve. Thus the statement of greater male variability meant that more men compared to women would be found at the extremes of the distribution, and this was held to be a fundamental and innate difference between the sexes.
Interestingly enough, one of the strongest supporters of the variability hypothesis was Edward Thorndike, a professor at Columbia and one of the great names in the history of psychology. In 1906, before Hollingworth came to Columbia and began studying with him, Thorndike was writing that because of the “restriction of women to the mediocre grades of ability and achievement” and because society needed only a few gifted persons in the professions, women should be trained for work “where the average level is the essential” (p. 213).
A short eight years later, in 1914, Hollingworth launched an assault on the variability hypothesis, offering a different interpretation of the oft-cited surplus of men among the gifted as well as among the retarded. Women, she said, have historically been restricted to domestic roles where eminence is not possible. Further, both educational and occupational opportunities have been restricted or denied to women, thus closing to them those doors for developing potential that have always been open to men. Therefore, without equality of opportunity, it is fallacious to compare the achievements of the two sexes. As for the finding of more men among the retarded, such figures came from persons in institutions, where men were more likely than women to have been admitted. This was because of women’s social role, which made it more possible for them to survive outside an institution: “Women have been and are a dependent and non-competitive class, and when defective can more easily survive outside of institutions, since they do not have to compete mentally with normal individuals, as men do, to maintain themselves in the social milieu” (Hollingworth, 1914b, p. 515).
Hollingworth’s alternative explanation for the lesser range of women’s achievement is both more cogent and more scientifically parsimonious than is the biologically based variability hypothesis. Since her time, it has ceased to be an important issue, at least in the guidance of women’s education and rights in the society. As for evidence, even when sophisticated testing programs occasionally reveal sex differences in variability, the argument from biology is not being raised (Benbow and Stanley, 1983). As long as social conditions vary as much as they do for the socialization of boys and girls, as in many other areas it is not possible to know what are the relative contributions of nature and nurture.
In 1916 Hollingworth published “Social Devices for Impelling Women to Bear and Rear Children.” This was a remarkable paper for its time, for it challenged the universality of the maternal instinct and the sentimental idealization of motherhood, both popular concepts at the time, and showed how it was neither biological nor altruistic motives that caused women to have large numbers of children. Rather, said Hollingworth, powerful agents in the society exercise control mechanisms over women to insure that women will be motivated to dedicate their lives to the bearing and rearing of children to the exclusion of other interests.[12]
Ever the scientist, Hollingworth began her argument by stating that it is necessary to “clear our minds of the sentimental conception of motherhood and to look at facts” (p. 19). These facts are (1) the bearing and rearing of children are necessary for the country’s existence; (2) the bearing and rearing of children are painful, dangerous to life, and require years of labor and self-sacrifice; (3) there is no evidence of a maternal instinct of such power as to impel women voluntarily to seek the pain, danger, and labor involved in maintaining a high birth rate. Therefore, she said, those in control of society have invented powerful mechanisms to insure that women will willingly take on the burden of producing large numbers of children. These include:
The social type. Similar to today’s concept of “role model,” this was the ideal of the normal woman, the criterion being her enthusiasm for maternal activities. Authorities agreed that it was abnormal for a married woman to want no children or to have other interests that competed with maternity. Since no one likes being seen as abnormal, this device, sanctioned by the authorities of medicine and science, served well the national interests of engaging women in procreation to the virtual exclusion of other activities.
Public opinion. Opinion leaders, including the media, appealed to women’s patriotism as they deplored the slowing of population growth. Jesuit priests praised maternity. The German kaiser announced he would be godfather to seventh, eighth, and ninth sons. A president congratulated a mother of nine.
Law. Here was a social instrument that, by restraining women from owning property, blocked them from any power of their own and made them dependent upon men, with no way to escape to a life of their own making. Provisions that acted directly to keep up the birth rate included the right of the male to divorce his wife if she proved to be sterile and those that forbade the distribution of birth control information. Thus women were forbidden the knowledge that would make childbearing voluntary.
Education. From birth girls were reared to be future wives and mothers, with no aspirations for lives of their own. Not only was no real enlightenment provided for girls, their education being seen as unimportant, but immature minds were drilled with the expectation, both overt and covert, that they would spend their lives in these roles, regardless of their individual abilities, talents, or tastes.
Illusion. To create a desired illusion, Hollingworth said, one must conceal and taboo all mention of any of its negative elements. Thus conversation about the processes of birth, its pain and risks, was taboo, especially with the young. Maternal mortality rates were suppressed. The drudgery and labor of caring for young children was not mentioned. Rather, there was fostered the illusion that motherhood consisted of gratification only, and popular art promoted this by depicting motherhood as a joyful and gracious state.
Bugaboos. Finally, Hollingworth cited the use of threats of negative consequences to women who had no or few children. Medical authorities of the time claimed that women should begin their childbearing as early as possible, as risk and pain increased with age. They also claimed that women who bore children lived longer than did those who were never mothers. In addition, it was widely advised that only children were at risk to be selfish, egotistical, and generally undesirable as citizens. When women became conscious of these methods of social control, cheap and effective as they were, they would reject them, Hollingworth believed. When that happened, and when women could have free choice to have no, one, or many children, then and only then would we gain an understanding of the “maternal instinct” and its distribution as a human trait in women’s personalities (Hollingworth, 1916).
Leta Hollingworth urged women researchers to follow John Stuart Mill’s advice to “give testimony,” to give their attention, to women’s issues:
Thus, in time, may be written a psychology of woman based on truth; not on opinion; on precise, not on anecdotal evidence; on accurate data rather than on remnants of magic. Thus may scientific light be cast upon the question ... whether women may at last contribute their best intellectual effort toward human progress, or whether it will be expedient for them to remain ... the matrix from which proceed the dynamic agents of society (Hollingworth, 1914a, p. 99).
Margaret Mead
Margaret Mead was born in 1901. Her father was a professor at the University of Pennsylvania, and both her mother and her paternal grandmother had been teachers. In Mead’s autobiography, Blackberry Winter (1972), she attributes her attraction to intellectual interests to her father. But it was the two women, her grandmother and her mother, who most influenced her early life. Her grandmother, she wrote, was “the most decisive influence in my life” (p. 45). She had attended college when it was still unusual for a woman to do so, had married, had a child, and continued with her career in education. She had advanced ideas about child rearing and education, and, in fact, taught the young Margaret at home until she was ready for high school. Margaret’s mother was an ardent supporter of social and political causes, including feminism and woman suffrage. With her large family, however, she had little opportunity to realize her talents and abilities. “In my life,” Mead wrote, “I realized every one of her unrealized ambitions” (p. 29). With such models as these in her early years, Mead grew up with “no reason to doubt that brains were suitable for a woman.... I learned that the mind is not sex-typed” (p. 54).
Her interest in anthropology began at Barnard College, where Mead took a course with the famed anthropologist Franz Boas. She attended graduate school at Columbia and continued to work with Boas, who persuaded her to do her doctoral dissertation on adolescent girls to determine whether the troubles of adolescents were tied to the culture or if they were inherent in the psychobiology of youth.
Mead had learned from her training respect for all people and their various ways of life. Primitive people were not savages or barbarians; they were people whose culture had developed and persisted “without script,” that is, without written language or history. Any language or culture was as valuable as any other, and a primitive language or art could be as complex and elaborate as a civilized one.
For nine months Mead lived with the Samoans, observing, interviewing, and testing young girls. From this work came her first book, Coming of Age in Samoa, which became a best seller soon after its publication in 1932. This book included a chapter on the “deviant,” in which Mead described girls whose temperament had a certain intensity of response which made them different from the placid personality she came to expect of Samoan girls. The relationship between temperament, sex, and deviance in different cultures became increasingly interesting to her, and by 1931 she was ready to look more closely at the way culture shapes the personalities of men and women. She wanted to develop a new approach to the old question of innate sex differences, because “until one had got out of the way the problem of the effects of cultural stylization on feminine and masculine personalities, it seemed to be futile to raise questions about biologically-given sex differences” (1972, p. 196). With this in mind, she began during the early 1930s her studies of three primitive societies in New Guinea: the Arapesh, the Mundugumor, and the Tchambuli. The result of this was the now-classic book Sex and Temperament in Three Primitive Societies (1935).
In the Arapesh tribe, both men and women exhibited “maternal,” nurturant behavior and were equally concerned with the care of children. Child betrothal was practiced, and small boys learned to assist with the feeding and care of their small wives-to-be. Life centered on making things grow: animals, plants, and children. Members of both sexes learned to be cooperative, unaggressive, and responsive to the needs of others. Aggression against the rights of others met with serious disapproval. Even so, a few men and women were known to be aggressive. The others took pains to avoid provoking them, as the one who aroused anger in another was even more guilty than the one who got angry. The model personality for both sexes was built on traits considered feminine in our society. Mead found the Arapesh rather uninteresting at the time, because they yielded little that was helpful to her question of how cultural prescriptions of sex-linked behavior affected the personalities of men and women. For the Arapesh, the prescriptions were one and the same.
The Mundugurnor were different from the Arapesh in every possible way. Both sexes were ruthless, aggressive, and strongly sexual, and the maternal, nurturing aspects of personality were barely apparent. The cultural shaping of personality was very strong, and both women and men were expected to conform to a single model. Rivalrous and exploitative, they were rejecting and, by Western standards, cruel to their children. Women wanted sons and men wanted daughters, and babies of the wrong sex were tossed alive into the river. Not only did Mead loathe the Mundugumor culture, but again she felc that her central problem was not advanced by her contact with them. She was still missing the cultural contrast in sex training that she was looking for.
Finally, the Tchambuli provided the missing piece that made possible a new interpretation of the earlier data. Among these lakedwellers, the roles and characteristics of the men and women were the reverse of those considered appropriate in our society. The women took charge of all important business and domestic affairs. They worked in large cooperative groups carrying their individual fireplaces about with them and setting them down whenever there was work to be done. The little girls, like their mothers, were competent. Mead remarked in 1972, that it was the only culture she had seen in which it was the girls who were the upcoming ones, curious, exploratory, and free. The men spent most of their time in ceremonial houses on the lake, carving, painting, and gossiping, and working out their rivalries with each other. The small boys learned this male way of life at an early age.
It was during this period that Mead began to develop her ideas about the cultural standardization of temperament, and the role of social conditioning that selected certain characteristics to reinforce and neglected or punished others. That these were not necessarily based on sex was apparent from the unisex models of the Arapesh and the Mundugumor. Such models, however, applied to ways of expressing feeling, to permissible manifestations of basic drives. The fact that these were independent of sex did not mean that the sexes were otherwise not differentiated. Beliefs about them, rituals and occupations assigned to them, were different. All cultures distinguished roles based on biological sex. But personality could be ascribed, and humans as groups could learn ways of being, on the basis of their membership in the group, or their membership in some category, such as sex.
Mead therefore concluded that human behavior expressed in personality characteristics is malleable beyond anything previously suspected. The differences between individuals who are members of different cultures are almost entirely attributable to differences in conditioning, and the form of this conditioning is determined by the culture. “Standardized personality differences between the sexes are of this order, cultural creations to which each generation, male and female, is trained to conform” (p. 280).
This emphasis upon the power of culture in shaping personality did not mean a complete denial of constitutionally determined individual differences.. Mead’s position was not the extreme environmentalist position of the psychologist John B. Watson (1924). Watson’s notion that the infant was a tabula rasa, a blank tablet, upon which personality would be inscribed by experience suggested a homogeneity of potential totally responsive to social conditioning. Mead saw the same range of temperamental variation in all the groups. The culturally selected normative personality was an overlay through which one could still perceive the idiosyncratic character even though it was attenuated by the imposition of the cultural personality. What happened was that the culture selected some aspects of the possible range of individual temperamental variation, either for everyone or for all members of the same category, such as sex, age, or race. For example, if warfare is a highly valued activity in a society, then all male children are expected to suppress any display of fear. The traits required for the occupation of males become identified as male personality; traits which may naturally be strong components of some individual personalities are developed as the norm for all, as key elements of a masculine personality. Likewise, Mead observed, if great importance is attached to the role of nurturing children by women, then the culture selects the trait of nurturance (even though the strength of it varies in individual women), reinforces it, and defines it as an essential component of feminine personality.
In societies where personality types are specialized by sex, that is, where certain ways of being and behaving are held to be appropriate for one sex and not the other, then, conditions favor the appearance of the deviant—the man or woman who temperamentally is unable to conform to the prescribed norms and behaviorally is more like the other sex. Such a maladaptive adjustment appears when the society has decreed an approved personality that is rigidly limited to one sex and considered unnatural for the other. As Mead pointed out, in societies such as our own and the Tchambuli where such sex-typing of personality is the rule, the appearance of deviants is inevitable. She found a compelling example of this among an American Indian group, which insisted that the ability to withstand any danger or hardship was a masculine characteristic, and small boys were relentlessly prohibited from crying, clinging, playing with younger children, or showing any sign of fear. Boys who did these things inspired the fear that they would turn out to be, not real men, but berdaches, transvestites who went about with the women and did women’s work. The presence of the berdaches was a constant threat to parents, causing them to obsessively reinforce in their boys the behaviors identified with masculinity.
Later we shall see that women have more leeway in our society with regard to expression of personality than men have. Thus one would expect a greater tendency to see norm-violating men as deviant, with greater tolerance of women who behave in atypical ways. That this can be true among primitive people also was shown by another anthropologist, Oscar Lewis, who described “manly-hearted” women in a Blackfoot tribe in Canada (1941). Whereas the ideal woman was submissive, reserved, and obedient, the manly-hearted women were aggressive, independent, ambitious, and boldly sexual. They owned property, took part in religious rituals, and chose their own mates. In a male-dominated culture, these women were clearly deviant, but in a special, favored way. Manly-heartedness was associated with having been a favored child who had been given special privileges such as playing with boys and assuming a leadership role. Being deviants from cultural norms, such women were strong enough to break away from sex-role restrictions, to capitalize on their assets, and to take the place they wanted in society. They went from favored child to favored woman—a rare model indeed in the patterns of culture.
What about the relations between the sexes in societies with rigid sex role dichotomies? Even for one who has incorporated the model personality for one’s sex there are repercussions. For example, if dominance and self-assertion are prescribed for males, the male having such characteristics requires submissiveness in others for reassurance of his own distinctiveness. When he encounters a woman who is as dominant as he is, doubt of his own manhood is set up in his mind. This is why, Mead said, that the man who conforms most closely to the masculine norm is the most suspicious and hostile towards deviating women. The male’s conviction of his own sex membership depends upon the non-occurrence of “his” traits in the other sex.
Her observations of these primitive groups, and the theoretical concepts relating cultural conditioning to sex-linked personality types, led Mead at that time, forty years ago, to a far-reaching proposal for the socialization of children. She observed that there are three possible courses for societies to take in developing the personalities of their children. The first is to specialize personality based on sex, as the Tchambuli did, and as most Western societies do. The second is to value a personality type that is indifferent to sex, a unisex model, as she found among the Arapesh and the Mundugumor. Either of these, however, results in unconforming persons being labeled as deviants, and thus cause unhappiness for some of its members.
There is a third way that Mead thought would reflect greater respect for individual freedom and dignity. The society could make room for the development of many different kinds of temperamental endowments. It could actively build upon the different potentials which it tries to train out of some individuals and to encourage and insist upon in others. Beneath the superficial category of sex the same potentialities exist, recurring in every generation. But they cannot develop if the society defines them as inappropriate for the person. For example, if only males can make music, then the musical aptitude of the most talented woman will never be cultivated. The temperamental variations which appear in both sexes could be encouraged, so that the differences among the individuals in the society would be real differences, not artificially created ones. Such a society would abandon attempts to make boys aggressive and girls passive, or to make all children aggressive. It would instead permit the development of the boy who is nurturant and the girl who is stimulated by fighting against obstacles. No skill or talent would go unrecognized because the child who had it was of the wrong sex. No child would be shaped to one pattern of behavior, for there would be many patterns, with each individual allowed to grow into the one that was most congenial to her or his innate temperament. Thus would the fabric of society lose its arbitrary character, and become a place where every human gift would be valued.
From our perspective today we recognize in such ideas contemporary values of individual freedom and self-actualization which, however ideal, are still far from being the usual experience for most people. Historically, some avenues of development have been open to some persons and not to others, as a function of sex.[13] The removal of barriers and the “letting be” as far as personality is concerned would allow for the fullest development of individual potential. Such a plan would not obliterate sex differences, nor would it simply promote a model whereby boys and girls were conditioned to the same pattern. Rather, individual differences, regardless of sex, would become manifest, and sexual category would no longer be a determinant of personality, except to the extent that the contribution of biological sex differences, as yet unknown, would have its effect.
Mead’s prophetic vision is reflected today in the goals of some members of our society. Stimulated by the feminist movement and counterculture values, it is now more possible for the male to renounce the old macho attitudes and values, and for the female to insist upon her right to be any way she wishes. If temperament is no longer standardized along sex lines, then we can expect to see more women exhibiting temperamental attributes heretofore called masculine, and more men who are free to manifest aspects of personality which an earlier age called feminine. If this comes about, one would expect it to be accompanied by changes in roles and institutions. For example, children might be cared for by nurturant, expressive men, and laws might be made by competent, determined women. At the present time, the impetus for change seems to be stronger among women than among men. This is understandable if one remembers that men, more surely than women, have had to expunge from their natures every hint of the other sex. Given the low esteem in which women and their traits have historically been held, it will take a major reappraisal of values for men, whether collectively or individually, to partake of their “feminine” selves, and to permit their sons to play with dolls if they wish. As for institutions, such as government, education, business, and the family, they could be maintained by persons who were temperamentally suited to fill the required roles, regardless of sex.
In 1974, Mead returned again to the issue in a critique of Freud’s last paper on the psychology of women. Discounting the penis-envy concept as hopelessly culture bound, she points out that the possibility of biologically determined psychological sex differences cannot be totally dismissed until more information is available. Since it is only very recently in human history that women’s reproductive functions have been modified, with fewer pregnancies, legal abortions, medical deliveries, and artifical feeding of infants, it is not possible to know what effects these and other such interventions will have on such ancient biological facts of a woman’s life. Mead suggests that it would be surprising if millions of years of cyclic changes and other features associated with childbearing did not have some effect on female personality. “The rhythms of human development, patterned during a million years, are ignored at our peril, and understood, give us wisdom” (p. 105). While this may sound like a softening of her earlier position on the malleability of personality, it is really a wise reminder of how little we know, and a caution against making interpretations that may be tinged with prejudice and wishful thinking at the expense of objectivity and truth.
The views of Horney, Thompson, Adler, Hollingworth, and Mead are unified by the recognition that women’s personalities are not necessarily determined by their biological functions. Their behavior and personality have been shaped, as men’s have, by both their bodies and their cultural assignments. Each theorist emphasized the crucial importance of the social roles of women and the attitudes toward women for the development of women’s psychology. They saw the effects also of the disparate valuing of the sexes and their respective attributes and achievements. They represent the appearance of a new way of looking at human behavior and point out new paths in the search for understanding of human personality. They are our bridge between the past of myths and misunderstandings, and newly emerging knowledge that better informs our thinking about ourselves.”
4. Sexual dimorphism, biology, and behavior
Biology can be said to define possibilities but not determine them; it is nevei irrelevant but it is also not determinant. For each person, brain-body-mind-behavior-environment form a complex entity the parts of which are inextricable from each other; the parts and the whole are ceaselessly interacting and changing and cany within themselves the entire history of their interactions.
—Ruth Bleier, Science and Gender, 1984
The historical record of beliefs about female behavior, its origins and its role in society, has varied greatly across generations and cultures. At one extreme was the frail, corseted Victorian lady in England, who required the chivalrous male to do those things for her that she could not do for herself. At the other is the desert-dwelling IKung woman in southern Africa who walks the ten miles back to camp after a day’s foraging, carrying as much as thirty pounds of plant foods on her back, as well as a child. Women’s behavior and social roles have varied so greatly that one marvels at the temerity of anyone, scientist or layperson, who attempts to formulate a general theory that can account for such diversity. In Western society, as we have seen, the most resilient explanation for women’s roles with their feature of universal subordination to men relies on the biological differences between males and females. Since these differences are real, the theory holds that the behavioral differences that appear to be identified with them are natural and inevitable. But whether based on biological determinism, cultural requirements, myths, or religious beliefs, theories and explanations of female behavior have had to take into account the biological dichotomy of sex, a dichotomy that, interacting with environmental influences, typically generates psychological and behavioral distinctions of unmatched importance for the individual and for society.[14] Assumptions about the connections between the biological dichotomy of human sexual identification and gender roles and personality are almost as old as psychology is. Later we shall consider current research that examines the relationship between body and behavior, an area that continues to be one of the most controversial in the psychological and biological sciences.
The differentiation of humans into two sexes, female and male, and the culturally defined meanings of this differentiation are universally observable. Although the mechanisms of biological sexual differentiation are well understood, their influence on those later behaviors that we associate with gender are far from clear. Thus in order to evaluate theories of female personality and behavior, we must begin with the phenomenon of sexual differentiation itself, the influences that bring it about, and the quality of the evidence for its effects on gender-related behavior in children and adults.
The conventional wisdom that the biological sex of the individual is determined once and for all at conception, the union of an ovum and a sperm cell, is an inaccurate oversimplification. After conception important intrauterine events occur that usually permit an unambiguous assignment of the baby’s sex at birth. This identification of the infant as boy or girl immediately affects the perceptions and behaviors of others as they relate to it. Thus myriad sequences of events related to its sex category begin to shape the course of its development toward a differentiated psychosexual or gender identity, the individual’s awareness of herself or himself as a member of one sex category and not the other. The gender identity of the individual is the result of a process of biosocial differentiation that begins at conception, proceeds along a course determined by intrauterine influences, and continues after birth in accordance with the sex of assignment and the gender-related socialization practices of the culture into which the child is born.
Both sexual dimorphism and gender dimorphism are usually congruent and invariant for humans. This means that a child who is biologically female will almost always differentiate a female gender identity, as a male will differentiate a male gender identity; and, with certain rare exceptions, which will be discussed later, both sexual and gender identity will be constant for life. Thus most members of all human groups are biologically and psychologically either female or male.
Gender identity, reinforced by interactions with others, behavioral prescriptions, and role assignments, is perhaps the most basic element of one’s self-awareness. The cultural components of its reinforcement, however, are not the same among all human groups. 1 he Tchambuli of New Guinea, for example, prescribed behaviors and roles for females and males that in some respects were the reverse of those traditionally observed in Western society. Though such gender-role assignments may vary from one society to another, all capitalize upon the principles of sexual and gender differentiation, assigning gender-congruent role behaviors to their members and proscribing some behaviors defines as incongruent with the sex assignment of the person. Both sexual and gender dimorphism, then, and their underlying determinants, both biological and cultural, have far-reaching consequences for individuals and for the societies in which they live.
Determinants of Sexual Differentiation
Sexually dimorphic biological development in humans and other mammals follows highly similar patterns and stages, such that accumulated animal research as well as studies of human clinical populations have resulted in an extensive body of knowledge on sexual differentiation. The development of sexual differentiation in humans and animals follows predictable stages that are roughly chronological and are under the influence of two major determinants, genetic and hormonal. The genetic determinant brings about the differentiation of the fetal gonad into either a testis or an ovary. Gonadal hormonal secretions in utero then influence the development of the sex-appropriate set of internal reproductive structures and cause the embryonic genital tissue to differentiate into either male or female external genitalia. A line of research on animals has suggested that the mammalian brain itself is affected by the influence of prenatal hormones so that certain behaviors are more likely to be displayed by one sex than the other (Goy and McEwen, 1980). The extrapolation of this finding to humans, suggesting that some gender-related behaviors, such as nurturance and aggression, are mediated by hormonally induced brain changes, has once again raised the old nature-nurture controversy. Later we shall look at the recent commentaries on this issue (e.g., Bleier, 1984).
Usually the sexual differentiation of the fetus is unambiguous and leads to a clear-cut assignment of sex category at birth. A biological female, then, will be assigned to the female sex at birth, will be reared as a female, and will differentiate a female gender identity. Occasionally, however, genetic and hormonal anomalies occur that place the person in an intermediate or indeterminant sexual category. These cases have been instructive in revealing more about the relative effects of the biological and social determinants of gender identity.
In addition to the prenatal biological determinants of sexual differentiation are the further differentiating effects of puberty with its distinctive body changes and the onset of the menstrual cycle in girls. These developments are also under genetic and hormonal control, and their programs are laid down before birth. By the time they occur in the life cycle, however, gender identity has been firmly established and their appearance simply confirms what the child already knows: for the girl, that she is becoming a woman; for the boy, that he is becoming a man. As the woman ages, her menstrual cycle and her fertility terminate during the climacterium with the ebbing of her ovarian hormones. The hormonal variations of the cycle and its cessation in menopause have also generated controversial interpretations of their importance in the psychology of women.
Genetic determinants
All cells of the human body with the exception of one type normally have twenty-three pairs of chromosomes of which one member of each pair was contributed by the father, the other by the mother. Twenty-two of these pairs, the autosomes, carry genes which determine the various features of the individual. The remaining pair are the sex chromosomes, which are designated XX in the female and XY in the male. It is these chromosomes which carry the genetic material responsible for the genetic sex of the individual. The germ cells, the ova and the sperm, are the exceptions. Produced by the ovaries and the testes, these cells when mature have twenty-three chromosomes, including an X in the ovum and either an X or a Y in the sperm. When conception occurs, the resulting zygote, the fertilized ovum, has its full complement of chromosomes and may be designated 46,XX or 46,XY as the case may be. If the ovum is fertilized by an X-bearing sperm the offspring will be female; by a Y-bearing sperm, male. Thus it is the father who determines the genetic sex of the child. The X chromosome is one of the largest of all the chromosomes, whereas the Y is often the smallest, carrying practically no genetic material. It does, however, have one important function. The Y chromosome causes the embryonic gonad to differentiate into a testis instead of an ovary.
Although the mechanism whereby this occurs is not fully understood, recent studies indicate that a single gene on the Y chromosome may be responsible. This gene produces H-Y antigen, a substance that adheres to the surface of male mammalian cells, including the Y-bearing sperm cells, and is responsible for programming the undifferentiated gonads into testes (Silvers and Wachtel, 1977).
Technically, the genetic determination of sex affects only the gonads—the testes and the ovaries. All other sexual differentiation is under hormonal control. If a Y-chromosome is present in the human zygote, the embryonic gonad will differentiate as a testis. If the Y is absent, as in the normal XX female, it will differentiate as an ovary. In the presence of Y, the critical period for the differentiation of the gonad into a testis is the seventh week after conception. If it does not occur at this time, the gonad will differentiate into an ovary.
It sometimes happens that in the process of cell division culminating in the mature ovum or sperm, the X or Y chromosome may be lost, or the cell may have one or more extra X’s or Y’s. If a zygote has such a chromosomal anomaly, the resulting individual will be a genetic variant from the normal XX female or XY male. Several such variants resulting from lost or supernumerary sex chromosomes have been identified. Two of these are 45,XO, Turner’s syndrome, and 47,XXY, Klinefelter’s syndrome. These variants best exemplify the principle that the absence of Y, rather than the presence of the second X, results in female differentiation. Conversely, if Y is present, the result will be a male (Table 4.1).
The child with Turner’s syndrome has only one sex chromosome, an X, which may have been provided either by her father or her mother. She may appear at birth as a normal female with female genitalia; therefore she is assigned and reared as a female. She is without functional gonads, which has two important effects related to the absence of ovarian function. The ovaries produce ova and female sex hormones, which bring about the body changes at puberty, the secondary sex characteristics of breast development, body hair, and female body form, and also initiate and regulate the menstrual cycle. Without ovaries, the Turner’s girl is sterile though she may have a normal uterus and thus can menstruate if provided with female sex hormones at puberty. She tends to be short in stature, usually under five feet. For this reason, the administration of estrogen is often delayed until she is sixteen or seventeen years old to permit her to grow as tall as she can, since estrogen tends to inhibit the growth of the long bones of the body. Under these circumstances, she will have a late puberty, and will be late in developing the female secondary sex characteristics, depending upon when her hormonal deficiency is corrected. The significant fact is that Turner’s girls and women are unequivocally female, even though their body cells have only one X-chromosome. Without the missing chromosome, be it X or Y, no functional gonads are present and the body differentiates as a female. (The absence of sex hormones is also significant for this differentiation, and will be discussed in the next section.) In addition, Turner’s girls differentiate a female psychosexual identity, and have especially strong “feminine” interest patterns and behavior (Ehrhardt, Greenberg, and Money, 1970). The implications of this Ending will be discussed later.
Table 4.1 Sexual differentiation and gender in four human syndromes
| Turner’s syndrome | Klinefelter’s syndrome | Congenital adrenal hyperplasia syndrome | Androgen insensitivity syndrome | |
| Sex chromosomes | XO | XXY | XX | XY |
| Gonads | Undifferentiated streak | Undeveloped tubules; variable | Ovaries | Testes |
| Hormones | Little or no gonadal | Low androgen | Elevated adrenal androgens | High androgen; cellular insensitivity |
| Internal reproductive system | Mullerian | Wolffian | Mullerian | Undifferentiated |
| External reproductive system (genitalia) | Female | Undersized male | Ambiguous | Female |
| Gender identity | Female | Male | Female | Female |
The individual with Klinefelter’s syndrome has both the double X of the normal female and the XY of the normal male. However, he differentiates as a male with testes, a penis, and a scrotum, though the penis may be small, and the testes undersized and sterile. The body type is clearly masculine, however, though psychosexual identity problems are not infrequent (Money, 1972a). The presence of the Y chromosome in this case mediates a male differentiation in spite of the two X’s. Variants of Klinefelter’s may have more than two X’s, but will still differentiate as males because of the single Y.
Thus the genetic determinants are crucial in starting the process of sexual differentiation of the embryo along a male or female line of development.
Hormonal determinants
After the genetic effects on biological sexual differentiation, the most important determinants are hormonal, directly affecting the differentiation of the internal system and the external genitalia (Fig. 4.1). The primitive gonad is unimorphic, that is, it is undifferentiated as to sex. Structurally, it consists of two parts, the inner part, or medulla, and the outer part, or cortex. If the genetic program calls for the gonad to become a testis, it is the medulla which proliferates, while the cortex becomes vestigial. If the gonad becomes an ovary, the cortex proliferates and the medulla regresses. While the testis begins to differentiate in the seventh week, the ovary begins much later around the twelfth week. This early differentiation of the testis allows it to begin secreting the hormones critical to the continued development of a male fetus with male internal reproductive structures and male external genitalia.
The human fetus is equipped with the primordia of both male and female internal reproductive structures. These are, respectively, the Wolfhan and Mullerian ducts. In male development, the Wolfhan ducts differentiate into the vas deferens, the seminal vesicles, and the ejaculatory ducts. In the female the Mullerian ducts differentiate into the uterus, the fallopian tubes or oviducts, and the upper part of the vagina. In the usual course, one or the other of these systems develops and the other becomes vestigial. Thus each sex carries in its body leftover remnants of the other. The decisive factor in determining which of these two systems will develop is the role of the secretions from the fetal testes.
The fetal testes secrete two hormones which promote the further development of the fetus in a male direction. One of these substances has the effect of inhibiting the development of the Mullerian system which otherwise would grow into a uterus, oviducts, and vagina. This substance is called simply “Mullerian inhibiting substance” after its only known function.
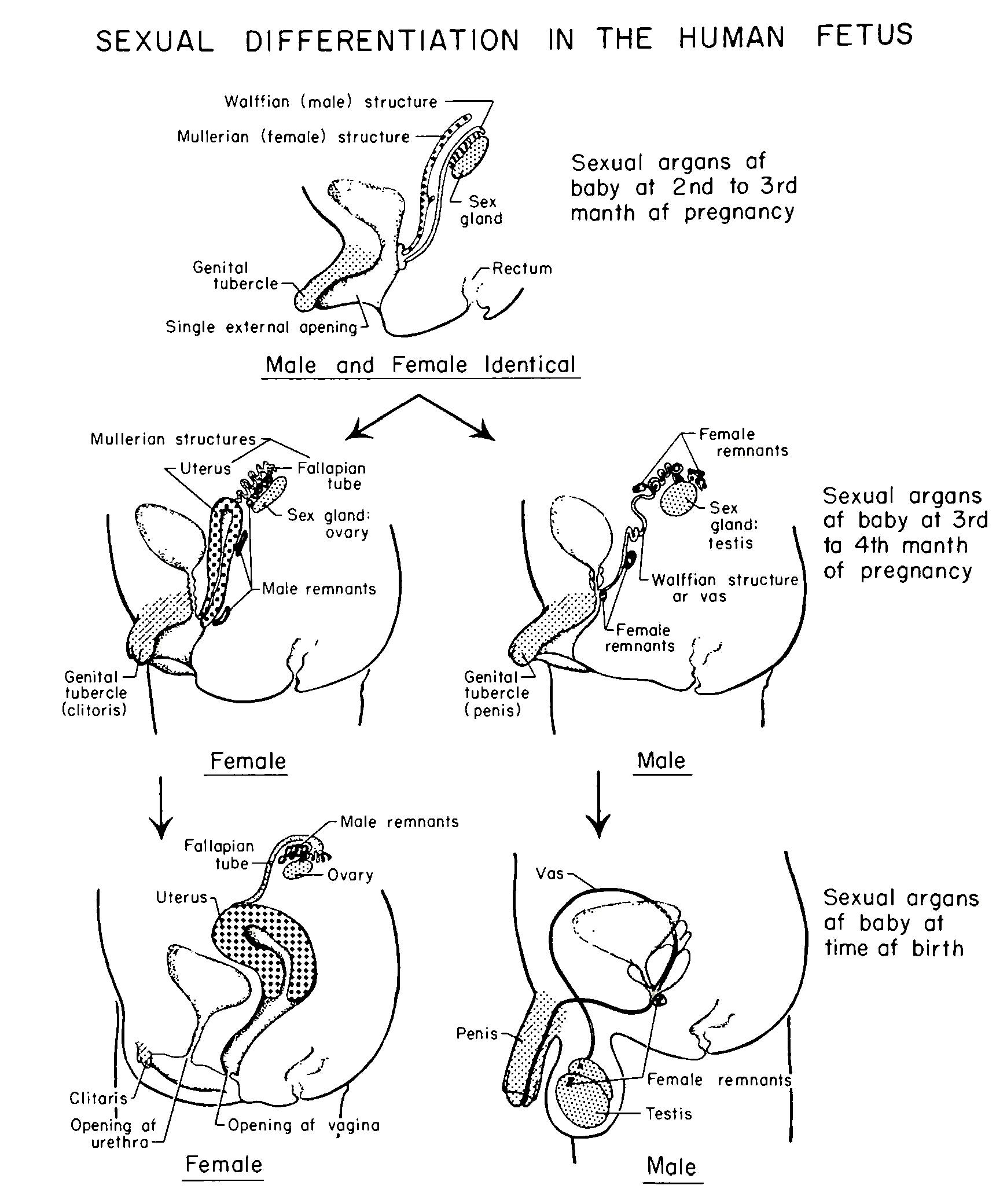
The other secretion of the fetal testes is the androgenic hormone testosterone. The androgenic hormones of which testosterone is the most potent are referred to as the male sex hormones because of their importance in male biological and sexual development. At this stage, testosterone promotes the development of the Wolffian system into the male reproductive structures. Thus the suppression of the female duct system is complemented by the elaboration of the male duct system. These two systems are the only basically dimorphic structures of the human embryonic tract. The gonads and genitalia are all unimorphic in the beginning, later differentiating into either female or male structures.
In the absence of testes or of these fetal testicular products, the Mullerian system will develop and the Wolffian system will become vestigial. The presence of ovaries or of ovarian hormones is not necessary for development of the Mullerian system into the internal reproductive apparatus of the female. In other words, in the XX embryo, there is no counterpart to the Mullerian inhibiting substance secreted by the fetal testes. If the fetal gonads, be they testes or ovaries, are removed before the critical period when one or the other of these systems becomes prepotent, then the Mullerian system will develop, and the Wolffian system will degenerate, regardless of genetic sex.
Rarely, the testes of a male embryo will fail to produce the Mullerian inhibitor. Such a situation will result in a male who is normal in all respects, except that he has a uterus and oviducts in addition to the usual male internal accessories. These extra organs can be removed surgically. The principle here, as with the Y chromosome, is that in the absence of the fetal testicular hormones, the differentiation of the internal reproductive organs will be female. This is true whether that “absence” is the result of surgical or chemical castration, or of non-secretion of the material if the gonads are ovaries. In the female no Wolffian inhibitor is present, and that system will degenerate just because there is no testosterone to promote its development.
The external male and female genitalia develop from common embryonic structures; thus they are unimorphic in the beginning. Before the eighth week of gestation, these structures are undifferentiated, and have the potential to develop in either a male or a female direction (Fig. 4.2). At this stage they consist of a genital tubercle which is situated above the urogenital groove. On each side of this groove are urethral folds beside which are labioscrotal swellings. In the female, the genital tubercle becomes the clitoris, the urethral folds become the labia minora (minor lips), and the labioscrotal swellings become the labia majora (major lips). In the male, the genital tubercle becomes the body and the glans, or tip, of the penis, the urethral folds fuse around the urethra, and the labioscrotal swellings fuse to form the scrotum.
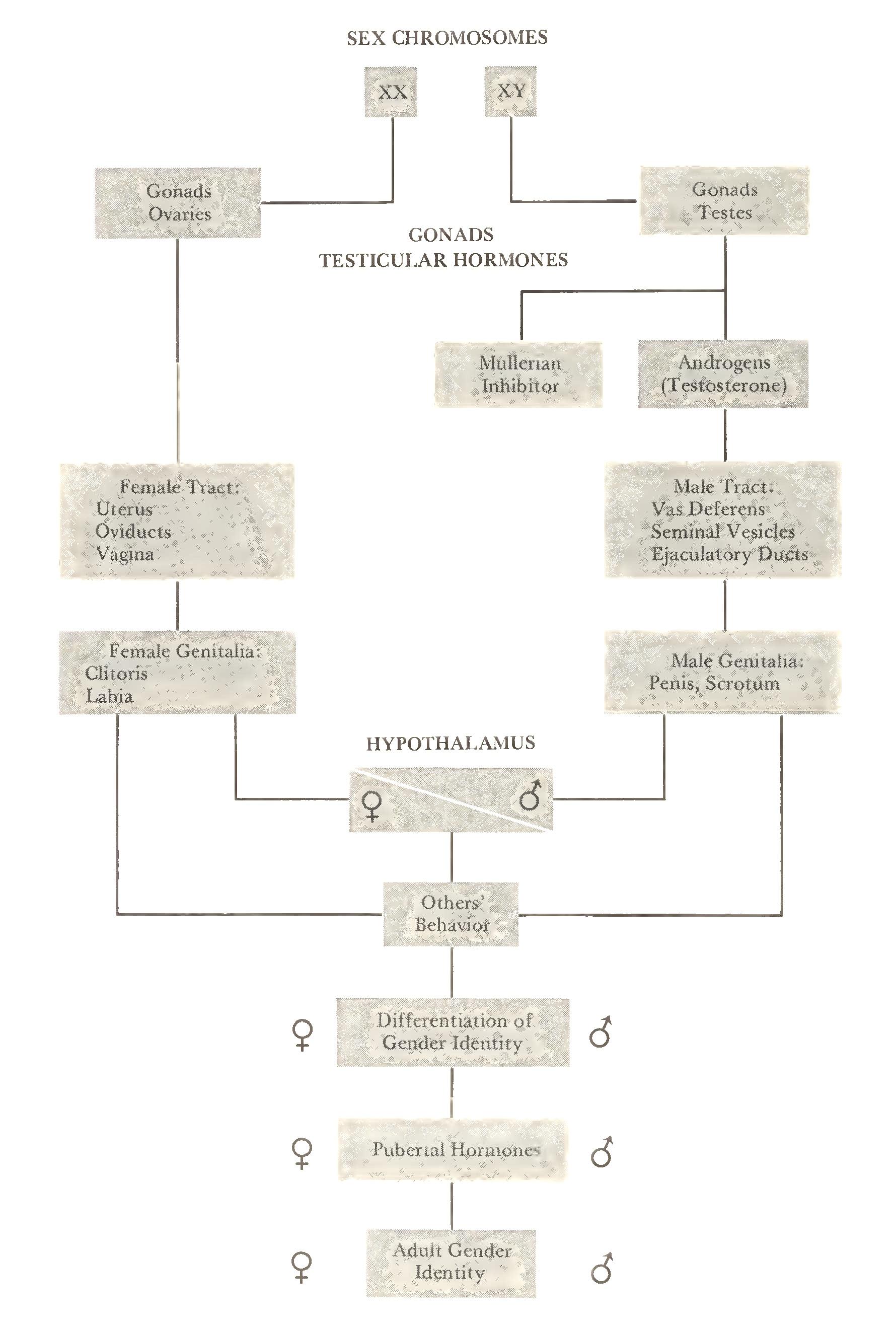
The differentiation of these structures as either male or female has been shown to be a function of the presence or absence of androgenic hormones. In the absence of these hormones, principally testosterone, they will develop into female genitalia regardless of genetic sex or sex of gonads.
Numerous experiments on rats, rabbits, and other mammals have confirmed that differentiation of the internal reproductive structures and the external genitalia is under the hormonal control of functioning testes (Jost, 1972). If the testes are removed from male embryos before these structures begin to differentiate as male, complete feminization of their development will ensue. Removal of ovaries from the female embryo has no effect upon female differentiation. Estrogen and progesterone, the female sex hormones produced by the ovaries, are not involved in the sexual differentiation of the female in utero.
The principle that sexual differentiation is mediated by the action of testicular hormones has been amply demonstrated in experimental studies on animals (Baker, 1980). In humans, the effects have been studied primarily on individuals born with ambiguous biological sex or with external genitalia and other characteristics which are discordant with the genetic sex. Examples of the condition which result respectively in the feminization of males and the masculinization of females will be described to elucidate the principle in humans.
The Erst condition is the androgen insensitivity syndrome, also called the testicular feminizing syndrome (Table 4.1). In this case, a genetic male (46,XY) is born with female genitalia, and subsequently develops a female morphology with female secondary sex characteristics in puberty, although functioning testes are present, producing the characteristic male hormones described earlier. The condition results from a recessive genetic defect which renders the body’s cells insensitive to the androgenic hormones provided by the fetal testes, so that all the structures that are dependent upon these hormones, primarily testosterone, for their normal male development differentiate as female. The functioning testes actually feminize the body at puberty, since estrogen, which is normally produced by the testes in small quantities, has full play to promote the development of the secondary sex characteristics typical of normal females. Such individuals may grow up as females, unrecognized as genetic and gonadal males until failure of appearance of the menses or discovery of the testes in the groin reveal the problem. The Wolfhan system, also dependent upon androgens for its differentiation, remains vestigial. The individual, in appearance a normal female, does not have a uterus and oviducts, however, because though the body was insensitive to the fetal androgens, it was not insensitive to the Mullerian inhibiting substance. Therefore, the differentiation of the Mullerian system was inhibited as in a normal male. Such persons are usually assigned and reared as females and develop a female psychosexual identity in spite of the discrepancy between their morphology and their genetic or gonadal sex (Money and Ehrhardt, 1972). They cannot be successfully corrected as males, since their bodies cannot utilize the androgens which are necessary for masculinization at puberty; that is, the development of secondary sex characteristics such as male body form, deepening of the voice, and the growth of beard and body hair. Since their bodies are unable to respond to androgens, they develop as if no androgens were present, that is, as if they had no testes. Without androgens, the body follows the female line of development.
The role of androgens in masculinizing the fetus is demonstrated in genetic females who have congenital adrenal hyperplasia (CAH) (Table 4.1). This condition is the result of a recessive genetic defect which causes the adrenal glands to malfunction beginning about the twelfth week of fetal life (Money and Ehrhardt, 1972). The adrenals, two of the body’s endocrine glands, are located on the kidneys. Their cortex or outer layers produces cortisol, a hormone that is necessary to life. In persons, male or female, afflicted with CAH, the adrenals are unable to produce the correct amount of cortisol. Instead, they produce large quantities of substances which are precursors to the synthesis of cortisol, and these substances are androgenic hormones. In most cases these hormones enter the bloodstream too late in fetal life to bring about development of the Wolffian system in females, and the development of the Mullerian system is unaffected, so that the internal reproductive structures are usually normal. The main effect is masculinization of the external genitalia, so that in extreme cases the female infant is born with a penis and an empty scrotum. In less extreme cases, the clitoris is enlarged and the labia partly fused. Since the cortisol deficit can be life-threatening, the disorder is usually recognized at birth or soon after, and the adrenal malfunction is treated with cortisone, a synthetic hormone which the body converts into cortisol. In some cases, the genitalia can be modified to the female form by surgery, and fertility and biological motherhood are possible. Others are not recognized as females, are assigned as boys and develop a male psychosexual identity. At puberty, however, the ovarian hormones will induce feminization of the body, and menstrual bleeding can occur through the urethra. These events can be treated hormonally to maintain the male identification, though suppression of the menses requires removal of the ovaries and the uterus.
The significance of such cases is twofold. The first is to demonstrate the effects of androgens on sexual differentiation of the body, elucidating the principle that without these hormones the fetus will differentiate as a female regardless of genetic sex. The development of male morphology depends upon their presence in body tissues capable of responding to them.
The second is that they provide the opportunity to study in humans the effect of such hormonal anomalies on behavior. Do the sex hormones circulating in the fetal bloodstream, affecting at certain critical periods the differentiation of the sexual-reproductive system, affect also the development of the central nervous system, resulting in certain differences in male and female behavior?
Data relevant to this question come from two sources: experimental studies of mammals other than humans in which prenatal hormones were manipulated by the experimenter to see the later effects on behavior; and longitudinal studies of humans with the hormonal anomalies described above. These studies provide a basis for understanding behavioral dimorphism, the extent to which biological influences program animals to behave differentially in accordance with biological sex, and, in humans, their relationship to the differentiation of gender identity, gender-role behavior, and sexual orientation (Baker, 1980).
Biology and Behavior
We have seen how differentiation of humans and other mammals into two biologic forms, female and male, is facilitated by the prenatal action of genetic and hormonal influences. Since these physical factors are so potent as shapers of the body and some of its physical functions, such as reproduction, research into their effects on behavior has been of great interest to scientists for decades. The basic question of these studies is, do prenatal gonadal hormones affect the developing fetal brain in such a way as to predispose females and males toward gender dimorphic behavior. For example, does the sex difference in levels of circulating testosterone in utero affect cortical neurons, causing morphologic differences in male and female brains that would account for greater dominance behavior in males and a greater readiness of females to nurture the young? And if such differences are observed in nonhuman species by experimentally manipulating hormonal levels, can it be assumed that similar mechanisms apply to human behavior?
Research into these and related questions has attracted much attention in recent decades, for reasons that are not entirely identified with the scientific pursuit of knowledge. As we saw in Chapter 1, theorists of the functionalist school of psychology attributed women’s maternalism and greater male variability in achievement to innate factors, thereby explaining on grounds of biological inevitability women’s universal involvement in child care as well as the greater numbers of males among the creators of culture. Today methods of research on brain development and hormonal effects are much more sophisticated, and the search continues unabated for connections, however fragile, between body chemistry and subsequent gender-related behavior. Some theorists have taken great leaps of extrapolation from animal studies to human behavior, attributing to our genes and hormones all kinds of “adaptive” behavior, such as “coyness” in women and polygamous tendencies in men (Wilson, 1978). Feminist scientists have responded vigorously to this new biological determinism, seeing it as today’s version of the use of science to “explain” social mechanisms that keep women in subordinate and confined roles (Bleier, 1984; Longino and Doell, 1983; Baker, 1980). Later we shall examine this controversy in more detail. The next two sections will review some animal and human studies relevant to the issues involved.
The animal model: experimental studies
Experimental studies of the effects of the gonadal hormones on behavior have used a variety of species, among them the rhesus monkey (Goy, 1970), beagle dog (Beach, 1970), hamster (Swanson, 1971), and rat (Ward, 1972). These studies use such techniques as removal of the gonads (castration) in utero, in infancy, and in adulthood to see the effects on behavior of deprivation of the gonadal hormones; administering opposite-sex hormones to young and mature animals; and treating pregnant animals with testosterone to observe the behavioral effects on the masculinized daughters. The focus of such studies is usually upon mating, maternal, and play behavior because they are most readily identified as sex-specific in nonhuman mammals. In general, it has been shown that gonadal hormones organize the nervous system so that certain behaviors will be dimorphically differentiated according to sex. For example, in a study using rhesus monkeys, females with masculinized genitals were produced by administering androgen to their pregnant mothers. The social behavior of these masculinized females was then compared to a control group of normal females. The effect of the androgen was not confined to the genitals. The treated monkeys exhibited behavior more typical of males of that species: they threatened, initiated play, and engaged in rough-and-tumble play more often than the controls did. When placed with an untreated female, they more often attempted to mount, showing pelvic thrusting and phallic erection. Their behavior as well as their genitals had been affected by the early exposure of their neural tissues to androgen (Young et al., 1965).
Another study involved the effects on behavior of masculinization of female beagles in utero. When they grew up, their social and sexual behavior toward a female dog in heat was like that of males, although the effect was stronger if they continued to be treated with androgen after birth. Pattern of urination was also affected. Like males, they lifted a hind leg and urinated more frequently than females did (Beach, 1970).
Effects of deprivation of gonadal hormones on male mammals have been extensively studied. Hamsters, castrated shortly after birth and given ovarian transplants, displayed cyclic female mating behavior when placed as adults with normal males (Swanson, 1970), and the sexual behavior of neonatally castrated male rats can be manipulated in either a female or male direction by the administration of female or male sex hormones (Grady and Young, 1965).
The results of such experiments on the mating behavior of lower mammals have led to the hypothesis that fetal androgens have an organizing effect on the brain, predisposing males and females to develop different patterns of reproductive and mating behavior, depending on the presence or absence of the hormones in utero. Various investigators have identified the hypothalamus as one brain area which is affected (Money, 1972a). The hypothalamus has an important regulatory effect on the vital functions of the body. It controls the activity of the pituitary gland at the base of the brain, which in turn directs the release of gonadal hormones from the ovaries and the testes. In lower mammalian species, the sexual-reproductive activity of the female becomes cyclical at maturity. The estrous cycle, as it is called, determines when the female is fertile and willing to mate. This cyclicity is a function of the hormonal regulation of the hypothalamus and is a primary disposition of estrous species. That is, the cyclicity proceeds innately in the female and is destroyed in the male by the action of androgen on the hypothalamus. The critical period at which this occurs varies in dif ferent species, being either fetal or immediately postnatal. In any case, the effect is permanent and irreversible in estrous species.
Primate female sexual behavior, however, is not regulated by any such mechanism. The menstrual cycle of humans and other primates is related to reproduction and not to sexual receptivity per se. Studies on the effects of androgens on the reproductive behavior of prenatally exposed human as well as nonhuman primates have shown that cyclicity, ovulation, menstruation, and pregnancy are not suppressed in these species. Thus the fetal androgens do not appear to affect the female primate brain as they do in nonmammalian species (Bleier, 1984). In addition, it has been shown that the mating behavior of nonhuman primates is affected by “social” conditions. Female rhesus monkeys reared without males exhibited more mounting and less presenting behavior with each other, while males reared without females exhibited less mounting and more presenting behavior (Goldfoot et al., 1983). This indicates that, while mating behaviors are influenced by pre- and postnatal hormones, the expressions of these behaviors in nonhuman primates is affected by social interaction with peers (Bleier, 1984).
The difficulties of drawing conclusions from the extensive literature on hormonal effects on brain and behavior in nonhuman mammals, as well as in other species, were pointed out in a recent review of the research (Goy and McEwen, 1980). In any such experimental study, results will depend upon such important variables as sex, species, age when treated, nature of the treatment, and behavior under investigation, to mention only a few. Species vary greatly in the kind and extent of their response to the presence or absence of the gonadal hormones. In addition, many of the sexually dimorphic behaviors which are mediated by the hormones are species-specific, that is, they occur in one or a few species and are not found in others. For example, in the research on the influence of the gonadal hormones on sexual-reproductive behavior, such as lordosis and mounting, the most frequently studied animals are the rat and the hamster—both rodents. Yet consistent differences exist between these species with regard to their response to hormonal treatment. Lordosis, for instance, can be induced in castrated adult male hamsters by treating them with ovarian hormones. Lordosis is not induced by similar treatment of adult male rats. Similarly, testosterone induces mounting in castrated female rats but not in hamsters.
It has been shown that gonadal hormones also influence non-reproductive behavior, such as activity level and aggression, in many species. Female rats are more active on the running wheel and in open-field tests, behaviors which are activated by estrogen. Castration reduces the levels of these activities in both sexes and eliminates the sex difference.
The effects of gonadal hormones on aggressive behavior differ markedly among species. Adult male mice are very aggressive toward one another until dominance relations have been established, whereas female rats rarely fight. Such behavior is related to levels of androgenic hormones, principally testosterone. Among hamsters, females are more aggressive than males are, though castrations reduces aggression in both sexes. Treatment of castrated females with ovarian hormones suppresses fighting, whereas in castrated males aggression can be increased by ovarian transplants and testosterone injections. (Goy and McEwen, 1980).
Studies of the relationship between testosterone level and dominance rank and aggression in nonhuman primates have yielded conflicting results. It has been tempting for scientists to hypothesize that high testosterone levels would be linked to rank and to aggressive behavior in primate groups, but a review indicates that no clear-cut finding has emerged (Steklis el al., 1985). One recent study suggests that part of the problem is in the highly variable levels of testosterone within individuals at daily intervals. Such fluctuations could mean that any correlations among variables might be spuriously positive or negative, depending on when the blood sample was taken. Testosterone was measured in the blood of twenty male vervet monkeys on several successive days, and fluctuations as high as five- to ten-fold were observed. In addition, observations were made on the dominance rank of the monkeys within their social group and on frequency of aggression. Interestingly, mean testosterone level was not significantly related to dominance rank. Rate of aggression was significantly correlated with same-day testosterone for dominant but not for subordinate males. Thus while dominance status per se was unrelated to testosterone level, occupation of the dominant position did affect hormonal-behavioral relationships. As the authors point out, such studies in this and other species underscore the impact of social status on physiological processes (Steklis el al., 1985). This important observation reminds us once again of the fallacy of looking for the single cause as explanation for complex behaviors. Even among nonhuman species, biology and the social environment interact in as yet poorly understood ways to affect behavior.
Findings from these experimental studies and many more indicate that no fundamental uniformity exists across species with regard to effects on behavior of the gonadal hormones. Though their influences are widely represented for both sexual-reproductive and nonreproductive behavior, their effects may be highly dissimilar, even reversed, across species. Similarly, a hormonally induced sexual dimorphism found in one species may not be present in others, or may be reversed. In fact, “... the boundless variation of behavioral and morphological sexual dimorphisms is one of the richest challenges to empirical science ...” (Goy and McEwen, 1980, p. 11).
Human studies
To study the effects of prenatal gonadal hormones on human behavior, one must look to errors of nature. For the past two decades a line of research has concentrated on girls masculinized in utero by congenital adrenal hyperplasia (CAH), a condition described earlier in which the cortex of the adrenal glands produces excessive amounts of androgenlike hormones during the critical period in which the genitalia are differentiating in a male or female direction. Such cases offered the opportunity to study the effects, if any, of androgen on the female human brain and possible ultimate effects on behavior, particularly on behaviors that are usually seen as gender-linked, as “masculine” or “feminine” (Money and Ehrhardt, 1972; Ehrhardt and Meyer-Bahlburg, 1981).
One of these studies compared twenty-five fetally androgenized girls, ranging in age from four to sixteen, with twenty-five nonandrogenized girls who were matched with them for age, IQ, socioeconomic level, and race. All had been given early corrective surgery if needed, and all had been reared as girls. The subjects in both groups and their mothers were interviewed on standard topics relevant to the research, and the gender-role preferences of the girls were tested.
The results of this study indicated that the androgenized girls were more likely to display certain characteristics called collectively “tomboyism.” Both they and their mothers identified them as tomboys, a status of which the girls were proud. However, they were not necessarily dissatisfied with being a girl, though some were ambivalent as to whether it was better to be a boy or a girl. None wished to change her sex.
Their tomboyism consisted of several elements of behavior and preference which distinguished them from the control group. They had a high level of physical energy expenditure in vigorous outdoor activity and boys’ sports. Unlike the androgenized female monkeys, however, they were not more aggressive in the sense of being hostile or threatening toward others. Their preference in clothing and hairstyles was for utility rather than for personal adornment, and they related little interest in doll-playing or baby-sitting. They were less involved in rehearsals for motherhood which seem to appeal to many girls, and were more likely to express the intention of having a nondomestic career, or of combining a career with a family.
Reported childhood sexual activity did not differ for the two groups, in that neither the androgenized girls nor the control girls manifested much sexual behavior. Whereas the masculinized female monkeys exhibited sexual behavior which was closer to the male pattern, the androgenized girls were not observably affected. They had adopted the cultural norms to the same extent that the non-androgenized girls had. A follow-up study when the girls had reached a mean age of sixteen found that heterosexual activities such as dating, petting, and intercourse were delayed by three to nine years. Only one woman reported homosexual fantasies, as well as both homosexual and heterosexual experiences. Since most were heterosexual in orientation, it appeared that their histories of androgenization and boyish role behavior did not determine a homosexual orientation in adolescence (Baker, 1980).
The results of this study led to the hypothesis that the tomboyism displayed by these girls was an effect of the masculinization of the fetal brain. These researchers suggested that the effect may apply to neural pathways that mediate dominance assertion, manifested in high energy expenditure, and in the inhibition of pathways that would eventually serve the development of caretaking behavior. Those paths mediating eroticism were apparently not affected. There was an important difference .between the results of such studies on humans and on lower species. The sex-specific behavior of lower mammals may be reversed by adding or removing androgen to the fetal environment. No such automatic effect occurs in humans, and any prenatally affected dispositions, such as the ones observed in these girls, can readily be incorporated into the postnatally developed psychosexual identity (Ehrhardt and Meyer-Bahlburg, 1981).
Studies of fetally androgenized girls that relate their exposure to sex hormones to later behavior characterized as “masculine” have been sharply criticized on methodological grounds by some reviewers (Bleier, 1984; Longino and Doell, 1983). For example, observation of the girls’ behavior was supplied by parents, teachers, and by the girls themselves. Since all of these sources knew of the girls’ problem condition, their reports may have been influenced by their expectations. An additional problem is the attribution of the CAH girls’ behavior to biological rather than to cultural factors. This attribution seems to derive from research on other species that shows that some sex-linked behaviors are hormonally influenced. But to show a causal mechanism in one species is not adequate to permit an extrapolation to humans, who have far more complex brains than any of the other species studied. Most gender-related behaviors in humans, such as participation in sports, dress, and the elements of domestic and “career” roles are strongly influenced by culture. It is a great inferential leap to suggest, for example, that hormones could dispose a girl to state a preference for a stay-at-home life of domesticity in contrast to having a career, given that such a model has been a reality for only a miniscule number of women during our evolutionary tenure on earth. Logically, too, the hormonal explanation must rule out such alternative explanations as environmental influences and this has not yet occurred (Longino and Doell, 1983).
To reinforce this point, and to put the study in proper perspective, several other observations should be made. If fetal androgen has an effect on the brains of lower species, facilitating the later differentiation of certain kinds of behavior along sexually dimorphic lines, then it is likely that it has some degree of effect on human brains as well. Studies of humans, however, do not support the conclusion that human role behavior is sexually dimorphic, that some behaviors such as competitive sports are “masculine” and others such as caretaking are “feminine” and that the brain is programmed before birth to facilitate the appearance of one kind and not the other, depending on the sex of the person. The elements of tomboyism, for example, are very common, even normative (and certainly normal) for American girls. Such behaviors are acceptable alternatives for girls. While the girls in Money and Ehrhardt’s sample had interests which were closer to the masculine stereotype than to the conventional feminine model, their psychosexual identity was unequivocally female. If they had displayed a high level of erotic interest in other girls, similar to that displayed by adolescent boys, or if they had identified with the male sex and had wished to change their sex as transsexuals do, then the effect of the fetal androgenization would be more impressive.
The evidence indicates, then, that prenatal androgen affects the central nervous system of mammals at a critical period when some pathways of the brain are organizing along sexually dimorphic lines, thus facilitating the development of some behaviors that are more likely to be manifested by males of some species, such as dominance and sexual approach. In humans, the effects of prenatal gonadal hormones are much less observable in behavior, and by themselves do not bring about the differentiation of human behavior along sex lines.
Though societies may prescribe different roles for males and females, the content of these roles may differ from one group to another, as we saw in Chapter 3. Such boundaries on behavior are artificial, however, since no absolute dichotomy of non-reproductive behavior by sex exists. According to John Money, a pioneer researcher in the area of hormones and behavior, only four human functions are invariably related to sex: males impregnate, and females menstruate, gestate, and lactate. All other criteria of sexual dimorphism of behavior are either derivatives of these or are optional according to time and place and, we might add, culture (Money, 1972b).
So, to the question, do fetal gonadal hormones directly affect the sexual differentiation of human behavior in later life, we can say that it is possible that they do, but that the effect may not be very important. The critical factors for the differentiation of human behavior and of human gender identity, the knowledge of who and what one is sexually, are those which impinge on the individual beginning at birth, which inform her and him by thousands of acts and subtle ways, of their membership in one sexual category or the other.
Gender Identity
We need now to look at some evidence for the overwhelming importance in humans of the sex of assignment and rearing on the behavior and on the formation of gender identity. To do so, one studies individuals who because of human error or developmental anomaly required sex reassignment and who were subsequently reared in accordance with that reassignment (Money and Ehrhardt, 1972). Such cases include genetic male infants who were assigned and reared as girls after loss of the penis, or owing to malformation of the penis; and CAH females as described above, some of whom were assigned and reared as boys and some as girls. These studies show the plasticity of human gender identity early in life, and its relative independence, under certain circumstances, of biological determinants of sex differentiation.
The first case involved a normal male infant, an identical twin, who lost his penis at age seven months in a circumcision accident. At age seventeen months the decision was made to reassign him as a girl, and a few months later genital reconstruction as a female was begun. The plan included hormonal therapy with estrogen at puberty. This case is especially interesting because the patient had an identical twin brother, thus providing an ideal situation for observation of differential childrearing practices based on sex. The mother, no doubt more sensitive than normal to the innuendos of developing a female identity in a child who had begun life as a boy, consistently promoted the child’s initiation into a feminine life style. Hair, clothing, toys, and training in domesticity and preparation for motherhood all became part of the conversion of being a girl. The mother was especially aware that she was consciously trying to introduce sexual differentiation between the boy twin and his new sister: “... of course, I’ve tried to teach her not to be rough ... she doesn’t seem to be as rough as him ... of course, I discouraged that” (p. 122). By the time this child was in school her behavior as a little girl was in remarkable contrast to the “little boy” behavior of her twin brother.
In the second case of reassignment of a genetic male infant, the baby was born with a penis about the size of a clitoris, with no urinary canal. The scrotum was partly fused and contained two testes. The decision was made to reassign the child when he was seventeen months, and treatment similar to the first case was begun. In this case, the child had an older brother to whom explanation had to be made, and whose changed behavior to his new sister could be observed. He began, according to the father, to exhibit a much more protective attitude toward her, and to treat her more gently than he had when she was his brother. The parents both began to report that the child was becoming “feminine,” and they were able to verbalize the difference in their treatment of her. The father no longer wrestled with her, but held her more and danced with her, while the mother encouraged her in imitative housekeeping activity. By the time the child was three, she was asking for a doll and Cinderella slippers for Christmas. Presumably, her transformation to female gender was complete.
These studies are interesting for two reasons. First, they show the extent to which gender identity can be acquired independent of the sex of genes and fetal hormones, and how sexually differentiated behavior can be shaped in accordance with cultural definition. Second, they demonstrate vividly the differential treatment of sons and daughters along the lines approved for each by the culture.
In another series of studies, the subjects were matched pairs of CAH females with ovaries who at birth had masculinized external genitalia. Each pair consisted of individuals with the same genetic and gonadal sex, but one was assigned as a girl, the other as a boy. Although reassignment of these cases was made at varying ages, their medical biographies all included surgical and hormonal corrections so that subsequent physical development would proceed in harmony with assigned sex. These cases, like the first two, differentiated gender identities in accordance with their sex of assignment.
The significance of this research lies in the finding that, where chromosomes and gonads are discordant with the sex of assignment and rearing, which are the results of decisions made by the caretakers of the child, the latter determinants will prevail. “To use the Pygmalion allegory, one may begin with the same clay and fashion a god or a goddess” (p. 152). If the corrections are made early and the parents have resolved their ambiguity as to whether they are raising a son or a daughter, then it is predictable that the child will differentiate a gender identity which accords with her or his assigned sex. “The evidence of human hermaphroditism makes abundantly clear that nature has ordained a major part of human genderidentity differentiation to be accomplished in the postnatal period” (Money and Ehrhardt, 1972, p. 18).
Most agree that the differentiation begins during the second year of life and is virtually complete by age five or six (Brown and Lynn, 1966; Money and Ehrhardt, 1972). Gender identity is imprinted during a critical period between eighteen months and three years, and after this period an elective change is not only rare, but, if attempted, may result in psychosexual difficulties for the child (Money and Ehrhardt, 1972).
The differentiation of gender identity is less likely to cause problems for girls. Just as in embryonic development, it seems that postnatally, also, the course of females runs more smoothly. Variations of gender identity from the expected biological bases are far more frequent among males. Such phenomena as transsexualism, the individual’s conviction that he is trapped in the wrong-sexed body, and transvestism, a compulsive need to wear clothing associated with the other sex, occur at least four and perhaps as many as ten times more often in the adult male population (Bermant, 1972). From myriad cues the child differentiates a dominant gender identity of male or female, and the other recedes in importance without vanishing altogether. Typically girls have greater latitude than boys in gender identification and the display of gender-related behavior—for example, tomboyism, whereas boys’ identification is more narrowly and rigidly prescribed. For males, it is more critical to repress the feminine traces. Thus the boy’s developmental task is made more difficult, and the outcome less certainly consistent with the templates of nature and culture.
Puberty: Physical and Hormonal Changes
Puberty is the developmental period between childhood and maturity during which hormonal events regulated by the hypothalamus bring about a rapid acceleration of growth, the appearance of the secondary sex characteristics, and the maturation of the sexual-reproductive system in both sexes. While there is a great deal of variation in the age at which these events occur, in general girls begin their growth spurt a year or two ahead of boys and reach physical maturity earlier. Early physical signs of puberty include the increase in rate of growth, budding of the breasts, and appearance of pubic hair. 1 hese may begin to appear as early as the ninth year in some girls, though the average age is around eleven (Tanner, 1978). Later developments include the maturing of feminine body contours, its fat distribution and muscle-fat ratio distinguishing it from the male, a slight increase in skin pigmentation, and deepening of the voice. The ovaries and uterus increase in size, and the menarche, the first appearance of uterine bleeding which is the onset of the menses, occurs. Menarche is a late event in puberty, occurring usually after the peak of the growth spurt has passed. Even then, reproductive maturity may come later, as the first menstrual periods are often infertile and irregular. Here again, however, individual variability is the rule, and menarche as well as fertility may occur in normal girls from the twelfth to the seventeenth year.
Male development during puberty includes, in addition to the growth spurt, the appearance of pubic, body, and facial hair, deepening of the voice, and the maturation of the reproductive system. The testes, penis, and internal reproductive structures enlarge rapidly. Sperm production begins, and the first seminal ejaculation occurs about a year after the acceleration of penis growth (Tanner, 1978).
The timing of puberty is a function of the hypothalamus, a brain structure which, among other things, stimulates the pituitary gland to secrete hormones that regulate the activity of the ovaries in the female, and the testes in the male (Fig. 4.3). Beginning before puberty, the action of the hypothalamus of the female becomes cyclic with respect to the pituitary and its relation with the gonads but remains non-cyclic in the male. The potential for cyclicity in the mammalian brain is apparently innate, being preserved in the female and demolished in the male by the action of fetal androgens. In other words, the hypothalamus is programmed in utero to become cyclic or non-cyclic in puberty, depending on the presence of fetal androgens.
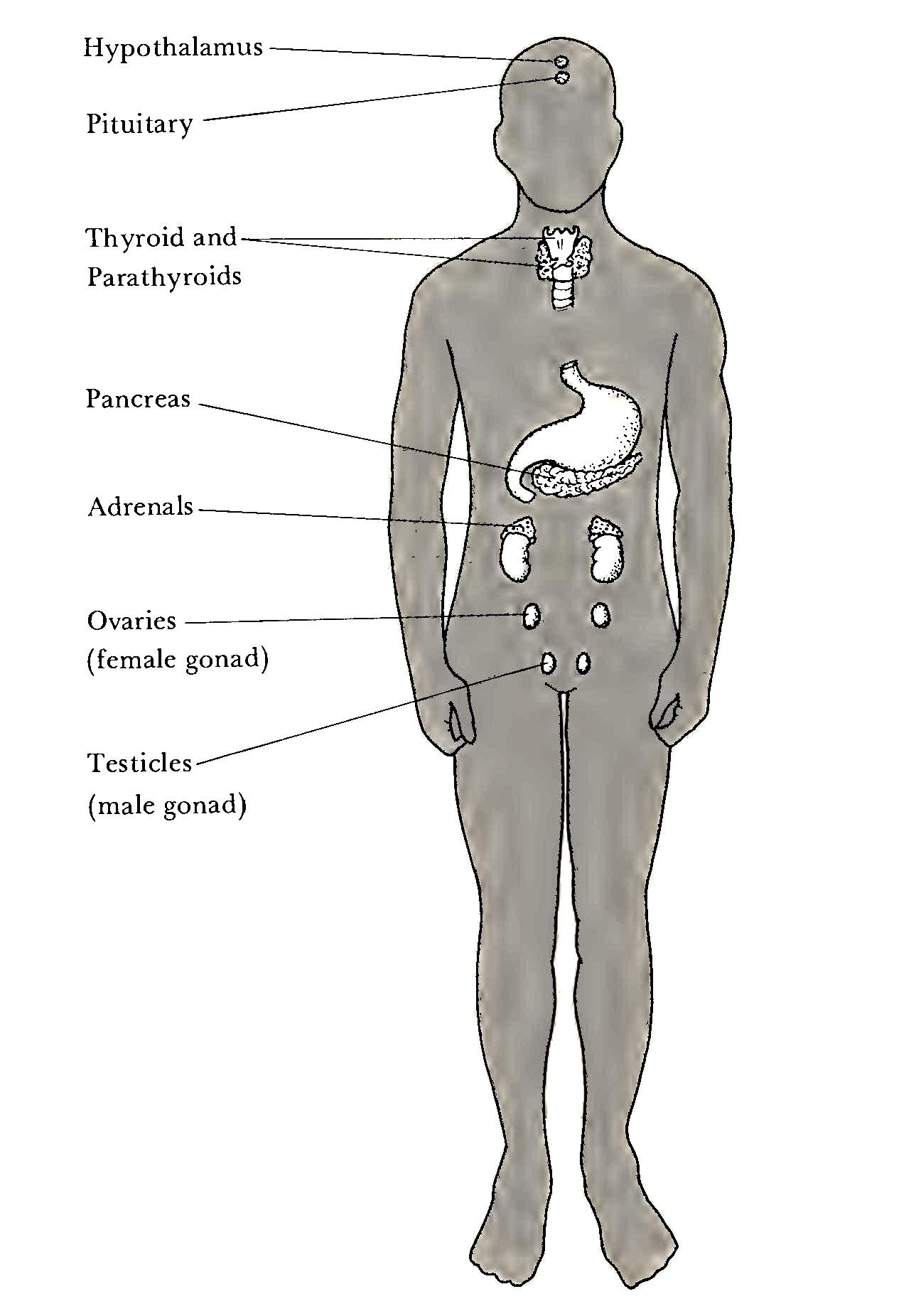
During childhood both sexes secrete small amounts of both estrogen and androgen. The girl’s androgen and the boy’s estrogen come chiefly from the adrenal cortex. In late childhood the pituitary increases its secretion of certain hormones which cause the ovaries and the testes to sharply increase their production of estrogen and androgen (mostly testosterone), respectively. At about this time, the pituitary and ovarian secretions in the female take on their cyclic pattern which becomes the basis later for the menstrual cycle. In the male no such cycle is known.
The onset of puberty cannot be dated exactly, since the changes in hormone levels and the resultant physical changes develop gradually over several years. Usually, the beginning of breast development and the growth of pubic hair precede the first menstruation. In Western countries the age of menarche has progressively decreased over the past several decades, probably owing to better nutrition and health care. In the United States the average age is about thirteen.
Rarely, tumors or lesions of the hypothalamus or gonads will cause an excessive production of hormones in young children, resulting in precocious sexual and reproductive development. When this happens to a female child, the result is early breast development and menarche, sometimes at the age of five or six years. Pregnancy can occur in such cases. An example was Lina Medina, a Peruvian child, who gave birth by Caesarian section to a six-and-one-half pound male infant at the age of five and a half years. This birth, on May 15, 1939, received much publicity, and was attended by several physicians from the United States. Lina was reported to have menstruated from the age of three.
Menarche and the Menstrual Cycle
Those biological events which are in women’s repertoire exclusively—menstruation, pregnancy, childbirth—have inspired myth and ritual for millennia. In particular, menarche and menstruation have mobilized man’s fears of the evil powers of women, and it has not been uncommon in human history for women to be “put away” at such times, and to be severely restricted in their contacts with men, animals, food, and utensils. In Borneo, for example, one tribe confines girls in dark cells raised on piles, sometimes for many months. When they reach womanhood, they are brought out and shown the sun, the earth, the water, and flowers as if they were newly born. Two common rules seem to apply in nonliterate societies: the menarcheal girl must not touch the earth or see the sun. “The general effect of these rules is to keep her suspended, so to say, between heaven and earth. Whether enveloped in her hammock and slung up to the roof, as in South America, or raised above the ground in a dark and narrow cage, as in New Ireland, she may be considered to be out of the way of doing mischief, since, being shut off both from the earth and from the sun, she can poison neither of these great sources of life by her deadly contagion” (Frazer, 1951, p. 702).
Societies all over the world, both nonliterate and civilized, have believed in the power of the menstruating woman to pollute and to contaminate. A South African cattle-rearing tribe believed that their cattle would die if they passed over ground where even a drop of menstrual blood had fallen. To prevent such a calamity, the women of the village had special paths they must use in order to avoid the ground in the middle of the village where the cattle stood or lay down.
Such beliefs persist today in certain parts of the country. For example, one male student told about an episode which occurred during a visit he made to some relatives in the mountain country of eastern Kentucky. The mother of the family was hard at work in the kitchen “putting up” vegetables. The student was talking to her when her daughter entered the room. The mother shook her apron at her, telling her not to come near the food “in that condition.” As the daughter ran from the room, two of the mason jars, filled with hot vegetables, exploded, thus confirming forever the mother’s belief in the power of a woman in her period!
Once established, the menstrual cycle in human females is a periodic interval of approximately twenty-eight days, though it may typically vary from twenty-five to thirty-four days, depending on the individual. The period of uterine bleeding is usually from three to seven days for most women.
The entire cycle is controlled by an elaborate feedback system involving the hypothalamus, the anterior lobe of the pituitary and its hormones, and the ovaries and their hormones. The hypothalamus monitors the level of the ovarian hormones in the bloodstream. Early in the cycle, counting the onset of the menses as day one, the estrogen level is at its lowest (Fig. 4.4). During these few days the endometrium, or lining of the uterus, is shed in the typical menstrual flow. Subsequently, in response to the low estrogen level, the hypothalamus signals the pituitary gland to release FSH (follicle stimulating hormone), which stimulates the maturation of one of the ova-containing ovarian follicles and also the increased production of estrogen by the ovary. As the level of estrogen increases, the endometrium begins to build up in preparation to receive the zygote if fertilization occurs. Ovulation, the rupture of the mature ovum from its follicle, occurs approximately fourteen days before the onset of the next period. At this time, the level of circulating estrogen in the blood is at its peak. Responding to this high level of estrogen, the pituitary releases LH (luteinizing hormone) which moves into the bloodstream to the ruptured follicle, causing it to develop into a glandular structure called the corpus luteum. The corpus luteum produces both estrogen and progesterone, the “pregnancy hormones,” which together stimulate the glands of the endometrium further to prepare for the nourishment of the zygote, if it appears.
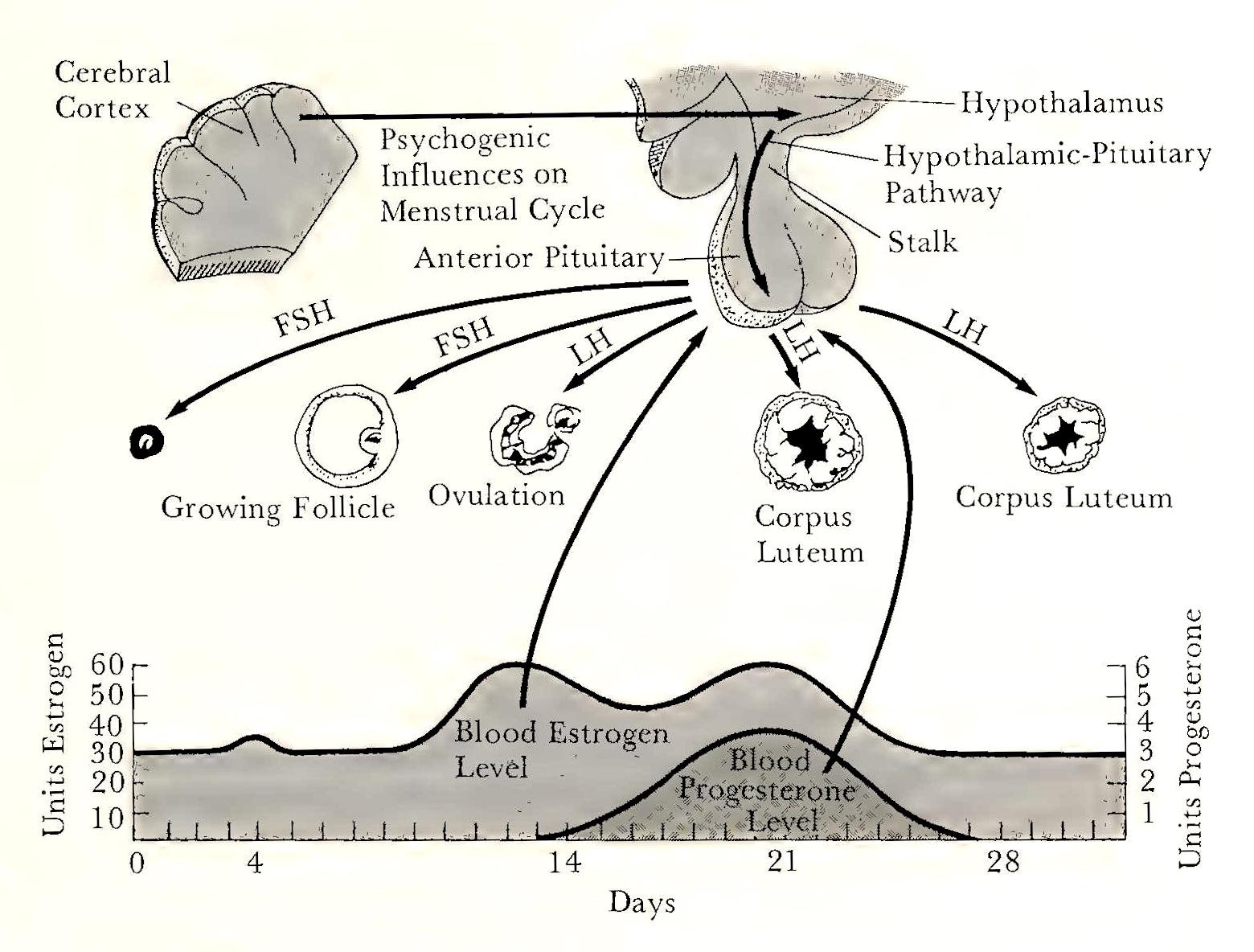
If fertilization does not occur, the pituitary ceases production of FSH and LH, and the corpus luteum becomes inactive and withers away. The subsequent gradual drop in estrogen level triggers the shedding of the endometrial proliferation, consisting of blood, mucus, and tissues, which is the menstrual discharge. In turn, the low estrogen level signals the hypothalamus to stimulate the pituitary to begin again its production of FSH, and the next cycle is under way.
Dysfunctions Associated with the Menstrual Cycle
The biological events associated with reproduction are surely of great importance in the lives of women. Even those who never experience pregnancy and motherhood are reminded of their potential every month for some thirty years. The salience of menstruation, and the frequency of its occurrence, mean that any dysfunction, whether physical or psychogenic, may provoke concern and even dread, to say nothing of the physical discomfort sometimes experienced. Disorders of menstruation, until recently poorly understood, have variously been held to be a manifestation of hysteria, hypochondriasis, stress, rejection of femininity, or the natural inferiority of the female. “Women,” said the eighteenth-century Italian writer Ferdinando Galiani, in Dialogue sur les Femmes, “only have intervals of health in the course of a continual disease.” Although some women do experience discomfort associated with their menstrual periods, this morbid diagnosis hardly fits most women.
There are three major kinds of menstrual dysfunction: dysmenorrhea or painful menstruation (cramps), amenorrhea or the absence of menstruation, and the premenstrual syndrome (PMS), a phrase used to describe a variety of symptoms experienced by some women during the few days before the onset of menses.
Dysmenorrhea, or cramps, is a well-defined clinical entity which occurs in about fifty percent of women at some time in their lives. The pain is reported in the pelvic area, and is caused by spasmodic contractions of the uterus. Usually, the pain is absent during the first periods, and it seldom persists after the birth of the first child or past the age of twenty-five (Lennane & Lennane, 1973). The cause of “childbirth cures” is not known. Dysmenorrhea has been found to be dependent on the occurrence of ovulation, and is usually removed or relieved by the suppression of ovulation with estrogen.
Primary amenorrhea means that the woman has never menstruated. In secondary, or functional, amenorrhea, menstruation has once begun but then ceased, or is very irregular. In either case, the condition may be caused by a variety of factors: congenital (absent ovaries, uterus, or vagina); physical (diabetes, trauma); or hormonal (diseases of the ovary, pituitary, or adrenal glands). It is not unusual for menstruation to cease as a reaction to emotional stress or drastic environmental change. In one study, 25 percent of a group of sixty-four American girls training in Israel developed amenorrhea of three months’ duration (Shanan et al., 1965).
Both primary and secondary amenorrhea have been shown to be related to the maintenance of a minimum weight for height. Studies of athletes and dancers and of women with anorexia nervosa (selfinduced undernutrition) indicate that weight loss in the range of 10 to 15 percent of normal weight for height, which represents a loss of about a third of body fat, results in amenorrhea. There are suggestions in the literature that a very low fat to body weight ratio may affect hypothalamic function and thus disrupt pituitary secretion of FSH and LH, thereby inhibiting ovulation (Frisch, 1983).
Premenstrual syndrome is a loosely defined collection of symptoms associated with the premenstrual period. The symptoms include swelling of body tissues and weight gain owing to water retention, emotional irritability, depression, feelings of anxiety and tension, and headache. Some women experience considerable distress from one or more of these symptoms each month, and others never experience them at all. The incidence of premenstrual symptoms varies from 25 to 100 percent of women, depending upon how they are defined and the population studied. Although large numbers of women spontaneously report awareness of the imminence of their period because of characteristic symptoms, the concept of a premenstrual syndrome itself is highly ambiguous, and there is no clear-cut agreement on causative factors. The only common denominator to such symptoms is that when they do occur, they do so at regular intervals (Sutherland and Stewart, 1965). Explanations of the phenomenon usually implicate hormonal activity, such as estrogen-progesterone imbalance, alterations of adrenal cortical functioning, sodium and water retention due to hormone changes, and so on. If the syndrome itself is not well established or clearly defined, identification of causative factors is a difficult enterprise (Parlee, 1973).
Behavior and the Menstrual Cycle
The preceding discussion of menstrual dysfunctions raises two related questions. Do psychological factors cause or contribute to menstrual disorders? What effect does the physiological phenomenon of the cycle have on behavior?
It is almost certain that the various symptoms associated with menstruation have a basis in physical factors; the view that such problems are “all in the mind” can no longer be held seriously by anyone. Even so, menstrual discomforts continue to be regarded as psychogenic, as symptoms of emotional problems, rejection of the feminine role, or the result of a faulty outlook on life.
The question of the effects of the menstrual cycle on behavior are only beginning to be understood. Numerous studies have reported correlations between the premenstrual phase of the cycle and such behaviors as crimes of violence, suicide, admission to psychiatric wards, and accidents (Dalton, 1964). However, most of these studies have methodological problems. The time of a behavioral act, such as commission of a crime, is readily identifiable, but information as to the phase of the woman’s cycle at that time is less reliable (Parlee, 1973). For example, one study found that two-thirds of violent crimes committed by women occurred in the premenstrual week, but does not say specifically how the phase of the cycle was determined (Morton et al., 1953). Another example correlated the test performance of schoolgirls with their menstrual cycle. Twentyseven percent declined in test performance during the premenstrual period. However, seventeen percent increased premenstrually, and fifty-six percent did not change (Dalton, 1960). Obviously, this is not impressive evidence linking hormone levels to school performance.
The past few years have seen an escalation of interest in PMS, though definitive results and alleviation of the problem continue to be elusive. The lack of a clear-cut set of symptoms identifiable as a syndrome makes definition difficult for purposes of research. Symptom information relies for the most part on subjective reports of afflicted women, and these may be affected by sociocultural effects as well as personality variables. Hormonal studies have problems with reliability owing to normal fluctuations in women on a daily basis as well as cyclic shifts related to the menstrual cycle.
Studies of normal women indicate that age is a factor in the experience of PMS. A group of high-school women showed no changes in measures of anxiety and depression across their menstrual cycles, including the premenstrual period, even though they did complain about menstrual distress (Golub, 1981). By contrast, a study of fifty women aged forty to forty-five found significantly elevated anxiety and depressed scores in the premenstrual phase compared to the intermenstrual part of the cycle (Golub, 1976).
Treatment approaches for PMS have varied, probably owing to the protean nature of the disorder and to differing opinions as to its causes. Psychotherapy, self-help groups, and drugs are all used, and some programs combine psychological, medical, and sociological approaches (Turkington, 1984). Based on the belief that PMS is caused by a deficit of progesterone during the premenstruum, physicians in Britain have been prescribing progesterone for many years and reporting good results. Researchers in this country are more skeptical, though some believe that it should be an option for American women (Turkington, 1984).
While there is little consensus in this field, most would agree that PMS symptoms are the result of interacting hormonal and psychological influences that vary among individuals and that women in whom only one factor is responsible for their symptoms are rarely found (Rubin et al., 1981).
One study of premenstrual effects on fifty normal women brings the issue into perspective:
The premenstrual mood change appears to be of the same order as afternoon lassitude, hurt feelings, or Monday morning blues. The anxiety ... is dramatically different in magnitude from that found in psychiatric disorders.... [F]or most women, the premenstrual hormonal changes impose little psychological burden. Women readily cope with premenstrual mood changes, and are sometimes not even aware of them (Golub, 1973, pp. 8–9).
The Climacterium
As women age, they enter the developmental period of the climacterium, when ovarian function gradually declines and finally ceases. An important event of this period is the menopause, the cessation of menstruation. The psychological events associated with this period are discussed in Chapter 13. Here the concern is only with those aspects of it that are sexually dimorphic, that is, where the course of events is different for women and men. The differences are in two related areas, hormonal and reproductive.
Estrogen and progesterone secretion begins to decline as ovarian functioning decreases, beginning gradually in the fourth decade and progressing more rapidly in the fifth and sixth. As the ovaries cease to respond to the pituitary hormone FSH, ovulation ceases to occur. With the greatly reduced output of estrogen and progesterone, the periodicity of the menstrual cycle disappears and eventually the woman becomes infertile. Both the cessation of menstruation and the decline of ovarian function, including ovulation, develop gradually in most women. Typically, a woman in her late forties will begin to experience missed periods or diminished flow over several months until finally the cycle no longer occurs. The eventual decrease in estrogen production to about one-sixth its earlier level is associated with physical changes in the body as well as with such symptoms as the hot flush. Among the effects on the body are the thinning of the vaginal tissues, reduced lubrication in the vagina, loss of hair, and loss of muscle tone with consequent drooping and flabbiness of the breasts and other tissues. The hot flush is a brief episode of feelings of warmth and flushing, accompanied by perspiration. Its frequency and duration are quite variable. Some women report great discomfort and others none at all. Other symptoms reported by women at this time include vertigo (dizziness), insomnia, headaches, tingling sensations, and anxiety. As in the premenstrual syndrome, the range and variability of these symptoms is so great that no well-defined menopausal syndrome exists. The body changes and the hot flush are predictable, however, being less dependent on personality and cultural beliefs and attitudes about how one ought to feel at such a time. Hot flushes and vaginal dryness can be alleviated by the exogenous administration of synthetic estrogen to replace the deficit caused by ovarian atrophy, though such treatment is used conservatively today owing to its risks for some women (see Chapter 13).
The virtual cessation of estrogen production of the ovaries brings about a drastic change in the hypothalamus-pituitary-ovary equilibrium which was maintained by the feedback mechanism discussed earlier. The final result is the absence of modulated periodicity: the menstrual cycle is extinct. If the postmenopausal woman takes estrogen daily, some endometrial buildup will occur. If she stops taking it for a few days, vaginal bleeding may result as the endometrium responds to the decrease in estrogen. This “withdrawal” bleeding is not a true period, however. The administration of synthetic estrogen does not bring about ovulation or restore fertility.
The male does not experience any single event analagous to the menopause although certain psychological symptoms of middle-aged males have been referred to as the male climacterium. These are mostly affective and behavioral, however, such as changes in selfconcept, mood swings, and abrupt changes in personality or life style, events which may reflect reactions to the perception of the aging process but not to any rapid change in gonadal functioning. Sperm production is affected only slightly by pituitary hormones, and the male theoretically remains fertile throughout his life span. The production of testosterone undergoes a gradual, continuous decline with aging: thus, the physiological mechanism is quite different from that of women. Male potency, the sexual capacity to sustain erection, declines with age but this is not directly related to spermatogenesis.
The biological fate of male and female differs in another important respect. Sexual differentiation extends to include different life expectancies throughout the life cycle, from conception to death. The importance of this statistical difference for the psychology of women, and its meaning, will be discussed in later chapters.
The Sex Ratio
The fact that humans are sexually dimorphic makes possible the collection of some interesting data on the relative prevalence of males and females at any particular age. The sex ratio is a statistic which is conventionally expressed as the ratio of males to females, times 100. The primary sex ratio, then, is an estimate of the number of male conceptuses per 100 females. Since many zygotes and early embryoes do not survive, the primary sex ratio must be inferred from the fact that sex ratios of the stillborn in the first four months have been variously observed as 200–400; that is, such a fetus is tjvo to four times more likely to be male (Lerner and Libby, 1976). Given even this enormous loss of males in utero, the secondary sex ratio, at the time of birth, is still 106 for live white babies in the United States. The tertiary sex ratio, which may be taken at any specified time after birth, shows a steady decline with age. For example:
Table 4.2 Sex ratios{2}
| Age | Sex ratio: secondary |
| Birth (live) | 106 |
| Age | Sex ratio: tertiary |
| 18 years | 100 |
| 50 years | 95 |
| 57 years | 90 |
| 67 years | 70 |
| 87 years | 50 |
| 100 years plus | 21 |
Furthermore, of the fifty-nine causes of death relevant to both sexes and listed by the U.S. Census, only two show a higher rate for females: diabetes and pernicious anemia. Thus, there is little reason to doubt the observation that females have a biological advantage.
Why Do Women Live Longer Than Men?
The average woman in the United States today can expect to outlive the average man by about eight years. This sex difference has increased dramatically in the past fifty years owing in part to rising male mortality from cardiovascular diseases and lung cancer and to declining female mortality from causes related to pregnancy and childbearing. But data showing higher male fetal mortality and higher male mortality during the first years of life suggest that endogenous factors play a part too.
A review of the literature on sex differences in mortality concluded that excess male mortality can be attributed to two major causes: behavior patterns that are more typical for males than for females and genetic factors (Waldron, 1976).
Compared to women, men are more than twice as likely to die from seven major causes: coronary heart disease, lung cancer, emphysema, motor vehicle and other types of accidents, cirrhosis of the liver, and suicide. These causes account for three-fourths of the sex dif ference in mortality in the United States. More than half of the sex difference in mortality from these seven causes is accounted for by men’s higher rate of cigarette smoking (related to coronary heart disease, lung cancer, and emphysema); type A behavior (a pattern of aggressive, competitive striving that is related to coronary heart disease in men); men’s higher alcohol consumption (related to increased accidents and cirrhosis of the liver); and physically hazardous employment, more likely to engage men than women. Each of these factors that contribute to males’ excess mortality involves behaviors that have traditionally been more acceptable for men than for women. Even if these behavioral sex differences have genetic contributions, cross-cultural studies show that child-rearing practices and cultural influences largely account for their expression. Type A behavior, for example, is rare in nonindustrialized countries, and drinking and smoking are proscribed among some people.
Lifestyle and behavior patterns cannot account for the higher mortality rate of male fetuses and infants, however, Through childhood, too, girls are healthier than boys, who, until about age ten, have more illnesses, more days of restricted activity, and more doctor visits. Males have less resistance to disease than females have, in part because the X chromosome carries genes for the production of immunity agents. In addition, estrogen and progesterone stimulate certain blood cells to destroy infectious agents, while testosterone does not. A small part of the excess of male deaths results from the more than fifty pathological conditions that occur almost exclusively in males because they are carried by X-linked recessive genes.[15] Most of these conditions, however, are not lethal.
Recent evidence indicates that the male to female ratio is decreasing for the major causes of death listed above, owing to rises in the female death rales for these causes. This reflects a trend for women to incorporate more life-threatening elements, formerly more common among men, into their lifestyles, such as smoking, alcohol consumption, and stressful employment, combined with domestic responsibilities.
If, as appears likely, the major reasons for the excess in male mortality, and the increase in female mortality in some areas, are related to behavior, then change is possible through increased knowledge from research and through education. The exercise of choice and taking responsibility for one’s health can lead not only to longer life but also to enhancement of quality of life as well.
To conclude this chapter on sexual dimorphism, biology, and behavior, we shall next consider a theory that has excited controversy among psychologists, biologists, and feminists in both disciplines.
Sociobiology: The New Biological Determinism
Sociobiology is a field of science that studies the social behavior of animals. In 1975 E. O. Wilson, a Harvard scientist who specializes in insect behavior, published Sociobiology: The New Synthesis, in which he set forth his theory that human behavior and social organization have evolved, as have our bodies, such that “adaptive” behaviors are genetically based and constitute “human nature.” Wilsonian sociobiologists (as contrasted to traditional sociobiologists, who confine themselves to animal behavior) propose that all kinds of complex human behavior, such as altruism, militarism, maternalism, rape, flirting, and hatred of those different from oneself (xenophobia), have become genetically encoded because they serve the adaptive purpose of increasing the “fitness” of individuals, that is, their ability to spread their genes, to leave as many descendants as possible, thereby insuring the survival of their own genes and their effective adaptations.
Sociobiologists, then, believe that culture is only a thin veneer over the basic “core” of human nature, which is grounded in evolutionary biology (Barash, 1979). Important elements of this “core” of human nature include reproductive behavior and the different social roles of women and men. Maximizing fitness would mean a genetic disposition to maximize the number of offspring. This goal would require different reproductive strategies for men and women. Men produce millions of gene-bearing sperm each day; therefore it is genetically strategic for them to impregnate as many women as possible with little biological investment in any one offspring. Women by contrast produce only about four hundred ova in a lifetime and can bear relatively few children because of the long periods of gestation and lactation. Since so few offspring will inherit her genes, it is adaptive for her to be choosy, compared to the male, for whom, according to the theory, promiscuity is the best strategy:
It pays males to be aggressive, hasty, fickle, and undiscriminating. In theory it is more profitable for females to be coy, to hold back until they can identify males with the best genes.... Human beings obey this biological principle faithfully (Wilson, 1978, p. 125).
Thus the biological differences between sperm and egg production are taken to lead to a genetic explanation for such social phenomena as the codes of virginity and chastity for women, and the expectation of male infidelity, polygyny, harems, rape, and so on.
Wilsonian sociobiologists also believe that important social roles of women and men ultimately have a genetic basis. Women are the primary caretakers of infants and children because, given that an individual woman can have only a few children, she has a much greater biological investment in the precious carrier of her genes than its father has; therefore its survival is more important to her. She may pass her genes to only a handful of children while he, theoretically, could biologically father countless numbers of offspring.
The relative scarcity of ova compared to sperm led to male competition for females, according to the theory. Since the larger, stronger, and more aggressive males would be more successful in this struggle, their genes would be more likely to survive, and these characteristics would provide the biological basis for such social phenomena as male dominance over females, competitiveness between males, male violence, and the willingness of males to fight wars (Barash, 1979).
Sociobiologists who have moved from studying animal behavior to theorizing about the potency of biology in determining complex human behavior have revived once again the old nature/nurture controversy that has flared up periodically during the history of Western science. Predictably, feminist scientists have reacted against the deterministic assumptions of Wilson and his colleagues, which support the subordination of women on the grounds of biological inevitability. Several problems have been identified. One is their ethnocentricity, describing social relationships “in the white Western industrial capitalist world” as if they are universal: “Sociobiologists make unwarranted generalizations about characteristic human behaviors, such as that ‘men would rather believe than know’ (Wilson, 1975, p. 561) or that women are coy and marry for upward social mobility” (Bleier, 1984, p. 23). The notion that women maximize their “fitness” by being particular about the men they are willing to mate led some sociobiologists to postulate a biological tendency in women to marry men of wealth and power. Since only a very few women ever get the opportunity to do this, given the scarcity of wealthy and powerful men anywhere in the world, the universality of even a tendency, let alone its expression, falls short of proof.
Another problem is the lack of identification of the mechanism by which genes would be expressed in complex behavior such as altruism or coyness. Not only are these behaviors not precisely defined as required by scientific method, but no genes accountable for them have been identified. Related to this is the observation that human evolution has occurred over hundreds of thousands of years, whereas social behavior and culture are highly variable in both time and place and may change drastically in a decade or a generation. In other words, there is far more universality of our bodies than there is of our behavior.
A basic issue in biological determinist theories of human behavior is the attribution to genes of a straightforward cause-and-effect relationship to behavior. This posits a dichotomy between biology and culture as they both impinge on the individual from conception. Most behaviors, even in animals, represent interactions between learning and biological mechanisms:
What has evolved in response to environmental challenge is the brain and its capacities for learning and culture, not behaviors themselves. Behaviors are products of the brain’s functioning in interaction with the external world, and the innumerable patterns of social behaviors, relationships, and organization that characterize human societies have evolved through cultural transmission within specific historical contexts (Bleier, 1984, p. 46).
Finally, feminist sociologist Alice Rossi argues not for sociobiology, but for a biosocial perspective. While genes do not determine what women and men can do, biological factors do create differences in their readiness to learn certain things. She believes that it makes sense from an evolutionary point of view for women to have a more positive response and a greater attachment to their infants, compared to men. The helplessness and dependence of human infants requires intensive caretaking for their survival, and women, as biological mothers, have a built-in predisposition to meet these needs more than fathers do, whose attachment to their infants is socially learned. The role of father around the world, says Rossi, is extremely diverse (as it is practiced even in our own culture), whereas the role of mother, with its cultural rule of close bonding, is universal (1978).
So the controversy continues, Women today, at least in Western society, have greater freedom from biological imperatives than any women have ever had. Perhaps this freedom will permit us the recognition that our behavior is the result of complex interactions between our biology, including our genetic heritage, and our environmental milieu, including socialization and cultural patterns, and the particularities of life chances, all of which shape our behavior, individually and collectively.
5. The emergence of gender differences
The very small amount of difference between the sexes in those functions open to experimentation, the contradictory results obtained from different series of investigations, and the nature of the differences which prove to be the most constant, have led to the belief that the psychological differences of sex are of sociological rather than of biological origin.
—Helen Thompson Wooley, Psychological Bulletin, 1910
Since learned or environmental factors affect the structure of the brain itself beginning prenatally and especially postnatally and also mold behaviors and attitudes from the time of birth, hulnan behavior is always fundamentally social and cultural and cannot be pared dozen to reveal a core of untouched or essential basic biological mechanisms.
—Ruth Bleier, Science and Gender, 1984
Almost eight decades have passed since Helen Thompson Wooley commented on the status of research into gender differences in her 1910 review. Since then research interest and the quest for more and better evidence of such differences, and theoretical explanations for them where they seem to exist, have continued unabated, such that today this is one of the largest literatures in psychology. Even though techniques and methods of measuring psychological processes are much more sophisticated than they were in Wooley’s day, the basic questions remain the same: do systematic, measurable gender differences exist? If so, what is their size, nature, and importance? And what are the mechanisms that create them and bring about their expression? In this chapter, we shall consider the evidence for the nature, extent, and importance of gender differences and some practical and theoretical issues raised by the research.
Sex and Gender
At birth infants are assigned to a biological sex category of female or male. This is one of the most important categories to which humans can be assigned, and it is constant throughout life, except in certain rare instances. Why is this characteristic of the person so important? It is because societies invest sex categories with meanings, such that from birth males and females will begin to have different kinds of experiences that to some extent will influence who and what they will become and the nature of their life courses.
In the last chapter, we looked at sex differences, that is, biological differences, between males and females. In this chapter we are interested in gender differences as they emerge in the behavioral repertoires of persons of both sexes. Gender refers to psychological attributes, characteristics, and behaviors that are acquired within a social context and that are related to the social meanings of sexual categories in a given society. For example, males and females are distinguished not only by their biological sex, but also by behavior, as, for example, the kinds of clothes they wear, the kinds of work they do, and so on. Such differences, where they exist, are not mandated by sex category, but rather are social constructions that can vary greatly from one culture to another. Psychologists have long been interested in gender differences between males and females, that is, psychological and behavioral differences that are not absolute as sex is, but that reflect some systematic difference in the performance of groups of one sex compared to the other. Thus when we speak of a gender difference we mean a difference in the average performance of females and males in a given area of behavior. Such measures of psychological characteristics are not categorical as sex is, but rather are distributed like the normal curve (Fig. 5.1), and a person’s’s performance is evaluated by where it is on the curve, relative to the average score. For example, a difference in spelling ability means that the average performance of one sex is higher than the average performance of the other. The performance of individuals of each sex varies around the average for that sex so that some persons in the high group score lower than some persons in the low group. The two sexes overlap in this way on all human intellectual and behavior characteristics. Therefore, the important general rule is that a given psychological gender difference is never absolute, in the sense that one sex has the characteristic and the other does not. Rather, individuals regardless of sex vary greatly in the extent to which they manifest a particular characteristic, such as verbal ability or dependency behavior. This means that when we look at measures of such behavior we invariably find that differences within a sex category, for example, differences among women, are greater than differences between women and men.
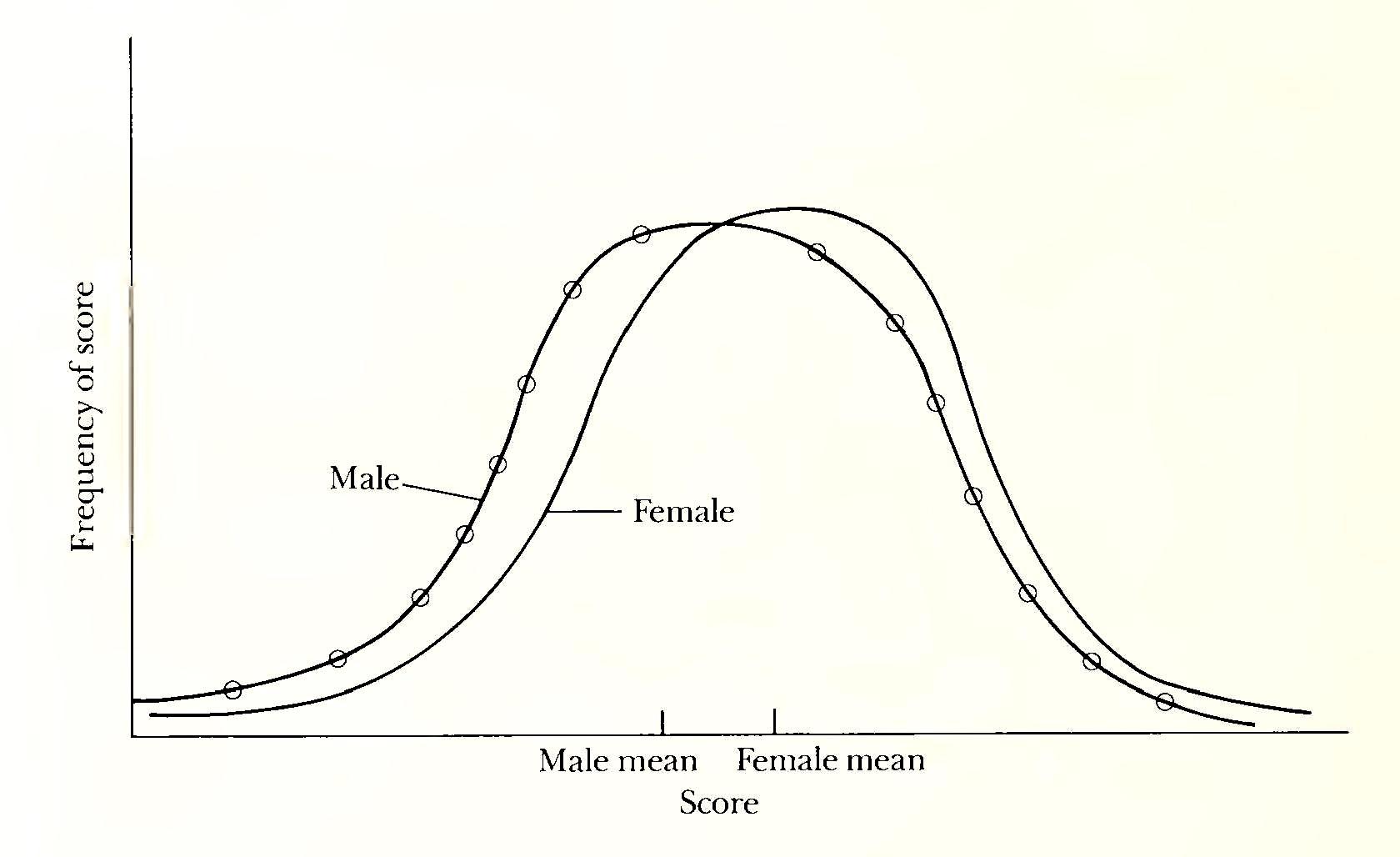
In addition, there are certain limitations to the literature on gender differences that can make interpretation problematic (Hoffman, 1972). First, judgments about the behavior of a particular individual or individuals may be relevant to a given group. For example, if some girls in a nursery school setting are rated high on “aggressiveness” it may mean that they are high compared to other girls in the group, or to the rater’s conception of what constitutes aggressiveness among girls in general. Similar behaviors by boys in the group might be seen as average, since aggressive behavior, as we shall see later, is more normative for boys than for girls. Second, it is risky to generalize results obtained from one sample or population to another. Most generalizations are valid only within certain contexts and under certain conditions. It has been found, for instance, that under certain conditions white females are more easily influenced by others than are white males; yet the case is reversed for black females and males, such that white females and black males are more easily influenced by others than are their counterparts. This and other studies indicate that race, social class, family structure, and other variables can make generalizations from one group to another inappropriate and misleading.
A third problem in interpreting gender differences is the differential maturity rate of boys and girls. Girls are physically and developmentally more mature than boys are from birth through puberty, and this difference complicates comparisons between the sexes. Finally, there is the problem, common to many fields, of the definition of concepts. Studies of dependency behavior, for example, may use different definitions of dependency, so that they are actually looking at different phenomena, leading to inconsistencies in the interpretations of the results (Hoffman, 1972). These problems and limitations will be pointed out in appropriate contexts as we go along.
Infancy
Few aspects of human development are so impressive as the growth and individuation of the infant during the first year of life. Observing the relatively helpless, supine, and asocial neonate[16] whose behavioral repertoire consists of a small collection of unlearned responses, one is awed by the transformation a few months later into a mobile, curious, imitative, and socially responsive young person who often wields a Promethean power to shape the behavior of others and to manipulate the environment. As a function of maturation and interaction with the contingencies of the environment, the infant’s behavior becomes increasingly diversified, differentiated, and complex. Do certain aspects of this behavior become differentiated along sexually dimorphic lines in infancy? Do boys and girls differ behaviorally from birth?
Physical development
Although few of us would have much confidence in our ability to identify the sex of each diaper-clad occupant of cribs in a nursery for neonates, there do exist biological sex differences in infancy in addition to those discussed in the last chapter. Girls are developmentally older at birth than boys are. Even though the gestation period is slightly shorter for girls, their skeletal maturation,[17] measured by the shape and degree of ossification or hardening of the bones, is four to six weeks advanced compared to boys. It has been suggested that the central nervous system of girls is also precociously developed giving them a greater readiness to function (Kagan, 1972).
Boys tend to be heavier and longer at birth than girls are, and this difference is maintained through childhood. They also have a greater lung capacity and, beginning soon after birth, a higher caloric intake.
Another important biological sex difference is found in the viability of females compared to males. The female manifests fewer defects and has a demonstrably greater capacity to maintain life. In the last chapter we observed the dramatic decline in the sex ratio beginning before birth. The prenatal death rate from miscarriages and stillbirths is considerably higher for males, and almost 33 percent more boys than girls die in the first year of life in the United States (Garai and Scheinfeld, 1968).
Studies of premature infants at a large New York hospital found that while boys and girls were about equal in incidence and severity of neonatal complications, the boys at 131/2 months were inferior on mental and motor tests (Braine et al., 1966). The same male infants at age 30 months had a higher incidence compared to the girls of neurological abnormalities and significantly lower IQs (Cutler et al., 1965).
The biological advantage of the female persisting through the lifespan has been attributed in part to the fact that she has two X-chromosomes, one from her mother and one from her father. Since the X-chromosome is larger and carries more genes than the Y, the girl can benefit from a greater variety of genetic material. Also, certain disorders[18] can be carried by genes on the X-chromosomes and will affect the individual unless they are offset by normal genes on a second X-chromosome. Thus the girl has a better chance of escaping such sex-linked disorders. The possibility of an immunological incompatibility between some male fetuses and their mothers may be related to productions controlled by the genes on the Y-chromosome (Singer et al., 1968). This would explain the spontaneous abortion of greater numbers of male fetuses. Such an effect might cause non-lethal damage to the male fetus with mental and physical effects later in life.
Neonatal behavior
In general, it is reasonable to assume that the earlier a behavior occurs the more probable that it reflects the biological heritage, shared by the individual with other members of the species. This is one compelling reason for studying the infant, in whom one might expect to find precursors of later behaviors in their pure forms uncontaminated by knowledge of consequences, ulterior motives, or other descriptors of the loss of innocence. For studies of gender differences, especially since numerous examples have been held to exist in childhood and maturity, we wish to know such things as: How early do such differences or their precursors manifest themselves? To what extent do they depend upon biological processes? How does such a substratum interact with subsequent environmental events to produce the increasing divergence observable both in roles and in personality traits which develop across the life span?
An important problem in studying the responses of very young infants for clues to etiology or sequelae of behavior is that in the neonate especially the behavioral repertoire is relatively small and its components are often not discriminately linked to specific eliciting stimuli. The neonate can sleep, cry, suck, flex arms and legs, move head and eyes, grasp, and respond to stimulation of its various senses. But a given response may be undifferentiated with regard to a stimulus. For example, crying may occur in response to hunger, discomfort, loud noise, loss of support, or no discernible cause. Because of these characteristics of the response repertoire, studies of male and female neonates have dealt mostly with sensorimotor reactions such as activity level or pain threshold and spontaneously emitted behaviors such as crying.
Though a few early studies reported gender differences in such variables as tactile sensitivity (Bell and Costello, 1964) and activity level (Bell, 1960), such results have not been substantiated. An analysis of thirty-six comparisons of neonates revealed that six favored boys (a subjective judgment as to desirability of the direction of the difference), seven favored girls, and the rest showed no differences (Shepherd and Peterson, 1973).
Older babies, still relatively free of the restraints and modifications that experience will teach them later, have a larger repertoire of behavior. It is more differentiated; its components are more reliably linked to stimulating conditions and are therefore more easily observed and measured. Consequently there is a sizeable body of literature on the developmental behavior of infants in the first and second year of life. Two areas which are important for understanding the emergence of gender differences are the development of cognitive and intellectual abilities, and the development of social and affective behavior.
Cognitive development
Cognition is the process by which the individual acquires knowledge. Modern cognitive psychologists study perceiving, recognizing, judging, and sensing—the ways of knowing. The efficiency and level of the acquisition of knowledge are usually measured in older children and adults by the use of tests which require language. Studies of infant cognition, of what and how babies “know,” have begun to appear only in the last decade, with the development of new techniques that provide insights into what and how babies learn.
In spite of the persistent belief that babies differ along sex lines— for example, that girl babies vocalize more and boy babies are more active—such differences in cognitive functions in the first two years of life have not been demonstrated (Maccoby and Jacklin, 1974). Measurements of intellectual ability, learning, and memory do not differ on the average for boys and girls. However, patterns of performances are different for the two sexes, as is the consistency (thus the predictability) of the measures as the infants get older. A longitudinal study of 180 white, first-born infants, 91 boys and 89 girls, each of whom was tested in the laboratory at four, eight, thirteen, and twenty-seven months offers some evidence concerning these patterns (Kagan, 1971). One of the behaviors for which different patterns were observed for boys and girls was vocalization, the infant’s response when aroused or excited by an unusual or discrepant stimulus.
The infant, in the third or fourth month, has developed schemata for recurring events in its life. A schema is a cognitive representation of an experience or an event. For example, the baby has a schema for the human face, or for its own room or crib. In everyday language, the baby “recognizes” its mother, or “knows” when it is put down on a strange bed. A strange face or bed is a discrepant event. Such a discrepant event in the life of an infant may provoke a variety of reactions, such as crying, fussing, smiling, or vocalization (a short burst of positive vocal activity), reflecting a state of arousal or excitement. It is this last reaction which concerns us now.
Stimuli presented to the infants included slides of human faces and taped auditory speech sequences. Some differences were found in the significance of the vocalizations of boys and girls to these stimuli. The boys’ vocalizations seemed part of a general restlessness, which included motoric behavior such as twisting and moving about. The girls, on the other hand, were responding to excitement generated by the attempt to assimilate an interesting, or discrepant, event. This special state of arousal was more closely related to vocalization for girls than for boys. Also, measures of attentiveness and subsequent vocalization were more closely related for girls. The girl who listened attentively to an auditory stimulus was more likely to vocalize when it ended. No such relation was found for boys (Kagan, 1971).
Jerome Kagan (1972) proposed two possible explanations for these differences. One relates the patterns of the girls’ vocalization and attentiveness to greater maturity of their central nervous system, especially with respect to speech functions. The other suggests that mothers spend more time in reciprocal verbalization with daughters, thus connecting vocal responses to human faces, whereas mothers (or fathers) of sons might engage in more motoric play with them. The absolute amount of vocalization did not differ for the girls and boys; rather, it was the significance of the vocalization that differed, as it related more to arousal state in girls and more to a general restlessness in boys.
Social class and cognitive development
Though gender differences in cognitive abilities in infancy have not been reliably established, one variable that interacts with sex to produce different effects for boys and girls from early life is social class. That is, social class has a greater relation to the cognitive development of girls than it has to boys.
The positive relationship between social class and intelligence as measured by IQ tests has been recognized since the early days of intelligence testing, and is one of the most stable findings in psychology. Although the trend of the correlation is the same for boys and for girls, the correlation for girls is higher. In the longitudinal study of infants described earlier, such cognitive measures as visual attention, increases in vocalization, vocabulary, and ability to identify embedded figures were all more clearly linked for girls, to parental social class (Kagan, 1971). Why should social class have a greater effect on the cognitive development of girls than of boys?
Maternal behavior differs by class toward boys and girls. Social class has less effect on maternal behavior toward sons than toward daughters. Mothers of all classes have in common the belief that sons should be independent, self-sufficient, and achieving, and they behave in ways that facilitate the development of such behaviors in them. Greater variability occurs across social classes in maternal behavior with daughters. Upper-middle-class mothers have greater faith in their ability to affect their daughters’ destinies, and spend more time talking to and entertaining them (Rothbart, 1971). Also, these mothers were much more concerned with the learning of task competence by their daughters than were the lower-class mothers. No comparable class difference was found for sons.
Now, if females are more mature developmentally from birth onward through early childhood, one would expect them to assimilate more readily whatever stimulation the environment offers, whereas boys would not show such effects until later. Given that uppermiddle-class mothers offer more intellectual stimulation to their infants, it follows that females would reflect this earlier than males would. Males of a given age, then, would show fewer effects across social class than females in infancy; such effects would be manifest later, as the cognitive development of the infant males became more responsive to the differential stimulation offered by mothers of different social classes.
Social and affective behavior
The earliest manifestations of affect, or emotional response, in infants are crying, including fretfulness and irritability, and smiling to social stimulation. Studies based on naturalistic observation of infants in their homes tend to report that boys sleep less than girls and cry more during the first three months (Moss, 1967). The difference in irritable crying diminishes, however, as a function of age, and later crying in older babies is more likely to be a reaction to fear, anxiety induced by separation, or some other exogenous event.
There is an interesting difference in maternal response to crying of boy and girl babies at three weeks and three months. Mothers were more likely to respond to irritability in girl babies at both ages, whereas at three weeks maternal contact did not vary with irritability of boy babies; in fact, by three months, mothers were less likely to contact the more irritable boys (Moss, 1967). Such a negative relationship may reflect the mother’s belief that boys should learn to endure discomfort, to rely less on comforting. Such a belief in the desirability of fostering toughness in boys could mediate maternal stoicism to their early wailing.
The so-called social smile appears in infants between two and eight weeks old. It is most often elicited by the human face and voice, and peaks in frequency around four months. There is no indication of a gender difference in readiness or frequency of smiling; rather, smiling seems to be a function of temperament interacting with experience.
The data on susceptibility to fear arousal in male and female infants are indeterminant. How does one infer fearfulness in a preverbal infant? Typically, the behaviors include crying, “freezing,” clinging to mother, or trying to reach her if separated. Are these reactions to fear-eliciting stimuli more typical of female than male infants? A few studies bear on this, and show the ambiguity of the results of the research. For example, one study considered reaction to separation in sixty-seven babies of each sex at age eight months. The child was placed on the floor with a toy. When the child was involved with it, the mother, on signal, rose and left the room, closing the door behind her. The child was observed for two minutes. During this period, 52 percent of the girls and 47 percent of the boys continued to play happily with the toy. While gender differences in irritability or fear did not occur within age groups, there were differences in the derivatives of these reactions when the infants were studied at twenty-seven months. Boys who had been most irritable at four months had lower vocabulary scores and less well-developed speech. Boys who were fearful at eight months were later more inhibited and apprehensive, staying closer to their mothers, than were the nonfearful controls. By contrast, girls who were irritable at four months became restless and active two-year-olds, and girls who were fearful at eight months were more verbal than the controls at twenty-seven months, and showed no need to stay close to their mothers. Thus irritability and distress seemed to have different meanings and different derivatives for the sexes. The crying, fearful boys became inhibited, shy two-year-olds; the same behaviors in four-month-girls were predictive of verbal, outgoing, precocious two-year-olds. Mothers perhaps react differently to fearful boys than to fearful girls, and this may account for the later observed differences (Kagan, 1971).
Dependency is an extensively researched behavioral concept which has been widely held to characterize females more than males (Mischel, 1970). To ask the question, Are infant girls more dependent than infant boys? points up a problem in evaluating the research on child development. Different observations may have quite different behaviors in mind when they are studying dependency in young children, so that the results may not be directly comparable to each other. For example, clinging, help-seeking, staying close to the mother, touching, wanting to be babied, crying in response to strangers, may all be part of a concept of dependency, but researchers may emphasize different aspects of it. Also, two hypothetical children might be equally dependent but one might manifest it by staying near the mother, the other by attention-getting behavior. In general, studies of dependency in young children have focused on proximity seeking, touching, and resistance to separation as indications of a child’s need for reassurance in an anxiety-provoking situation.
When such studies use infants as subjects, they are usually conducted in a test situation in which the child’s behavior and the motherchild interaction can be observed. Almost no studies include fathers. A review of studies of touching and proximity to parent and resistance to separation from parent included twenty-two studies of children aged three months to two years. Two-thirds of the measures showed no gender differences. Of the rest, girls had higher scores in the dependency direction on five measures, while boys had higher scores on six (Maccoby and Jacklin, 1974). Clearly, for these kinds of infant dependence behaviors, boys and girls are more alike than they are different.
Some studies have sought the precursors of gender differences in later life in mothers’ affective behavior toward boy and girl babies. Attachment behavior was studied between mothers and their infants at age twelve weeks, six months, and thirteen months. The researcher distinguished between two classes of attachment behavior: proximal and distal. Proximal behavior included physical contact, such as holding, kissing, touching, and caressing; distal behavior was contact other than physical, such as talking, smiling, and looking at each other. In these studies, mothers looked at and talked to their girl infants more from the earliest age. For the first six months they had more proximal contact with boy infants, perhaps because of their greater wakefulness. But after six months a reversal occurred, and girl babies had more of both proximal and distal contact with their mothers. By age thirteen months, the boys ventured farther from their mothers, stayed away longer, and returned to touch her less frequently. In the same situation, girls vocalized more, stayed closer, and touched their mothers more often (Lewis, 1972). The results appeared to show a stronger tendency for mothers of sons to encourage separation, exploration, and autonomy, while maintaining a closer interpersonal bond with daughters.
On factors such as warmth, nurturance, and acceptance, however, mothers evidently treat boy and girl babies about the same. Studies of parental warmth toward children, including twelve studies in which the children ranged in age from newborn to two years have been reviewed. Some of the studies measured more than one kind of parental behavior, such as affectionate touching, smiling at infant, and expression of positive attitude. Of eighteen measures of such behavior, no difference was observed for twelve. Of the remaining six, three were in favor of girls and three of boys (Maccoby and Jacklin, 1974).
In infancy, then, the conclusion is that gender differences in social and affective behaviors, including irritability, smiling, fear and anxiety, and dependency, have not been demonstrated. In early infancy boys may be awake more and be more fretful, but his difference does not persist. The derivatives of early behavior may differ, however, for the two sexes; for example, fearful eight-month-old boys were fearful two-year-olds, but the same was not true for girls (Kagan, 1971). Perhaps because of different developmental timetables a given behavior may have a different meaning for boys and girls at the same age.
Childhood
We want to look now at that period in the life span which includes childhood and early adolescence. By this time the young person has formulated an identity, and is discernibly different in personality and behavior from all other persons. Contributions from the uniquely given biological features and the uniquely experienced environmental events are inextricably meshed by this time, and one can hope only to discern the relative importance of one or the other to the observed manifestations of behavior.
Physical development
Throughout childhood boys tend to be slightly taller and heavier than girls are. This situation changes dramatically around age eleven, when girls start the growth spurt which signals the onset of puberty a full two years, on the average, before boys. For a year or two, around age twelve to thirteen, girls are on the average taller and heavier than boys are. The differences in skeletal maturity that were present at birth continue until adulthood, with boys having about 80 percent of the skeletal age of girls at any given age (Tanner, 1978). Few other body differences are observable, except for the genitalia, during the prepubertal period. Girls have slightly more subcutaneous fat, a difference which begins to increase around age eight.
Probably because of differences in central nervous system maturity, girls develop motor skills a little earlier and achieve sphincter control before boys do. In a national study in Britain, 12.1 percent of boys over five were still wetting the bed, compared to 9.7 percent of girls, a highly significant difference in such a large sample (Pringle, Butler, and Davie, 1966).
For a given body size, girls and boys are similar in strength during childhood. Girls reach their maximum strength, measured by arm pull and arm thrust, around menarche, while the strength of boys accelerates rapidly from age thirteen to adulthood. Boys’ greater lung capacity and caloric intake, which began at birth, and their higher basal metabolic rate prepare them to expend more energy and to burn up calories faster (Tanner, 1978).
These differences in physical development, like those of puberty described in the preceding chapters, are determined by biological factors. Within each sex, however, there is a wide range of individual differences in the ages at which the various events occur. The accelerated maturation of girls is observed also in the females of other primate species. Its biological significance is not at present obvious (Tanner, 1978).
Cognitive abilities
A very large literature on gender differences in intellectual abilities has accumulated during the last five or six decades, since techniques and methodology for measuring them have been developed. As in other areas of psychological research, consensus is not common, since different studies often yield dissimilar results owing to differences in characteristics of the sample, research methods, type of tests, definitions of concepts, and so on. Because of this characteristic of psychological research, it is possible to find support in the literature for a variety of positions on an issue. In the area of gender differences for any given characteristic one can find some studies that favor girls, some that favor boys, and some that find no difference. To date the most important survey of gender difference studies is The Psychology of Sex Differences, by Eleanor Maccoby and Carol Jacklin (1974); their focus was on gender differences among children younger than the age of twelve.
In their examination of the literature since 1966 on intellectual and cognitive abilities, they found areas where gender differences are fairly well established: verbal ability, mathematical ability, and spatial ability. The first favors girls, and the second and third favor boys. These three abilities, with others, are included in a global concept of mental ability, or intelligence. Verbal and mathematical ability are more closely related to general intelligence than is spatial ability, which is usually classified as a special ability, such as mechanical or artistic aptitude. Since intelligence is not a single measurable trait in an individual, the question of which sex is brighter is meaningless. Intelligence tests are made up of many items. If a test is heavily weighted with verbal items, then girls would be expected to score higher; if it is loaded with mathematical or spatial items, boys would do better. Most tests of general intelligence are constructed to eliminate such bias, so that gender differences are not expected to occur. However, of twenty-nine studies of intelligence covering the age range we are interested in,. Maccoby and Jacklin reported that ten favored girls, one favored boys, and the remainder found no difference. Even so, they conclude that gender differences in general intelligence have not been demonstrated, since those tests in which girls did better relied on verbal skills.
Though Maccoby and Jacklin’s work has long been regarded as a classic in the field of gender differences, it has attracted cogent criticism as well (Block, 1976; Caplan, 1979; Frodi et al., 1977). Maccoby and Jacklin used a “box score” approach such that, for example, they looked at all the studies of verbal ability and tabulated those that resulted in higher performance for girls versus those in which boys did better. This method does not take into account differences in quality of the studies, sizes of samples, and sizes of differences found. Also, since the majority of the studies surveyed used subjects under age twelve, the analysis could not reflect gender differences that might emerge later in life (Block, 1976). In any case, it is a useful entry point into the literature. Other Endings and commentaries will be included where relevant.
Verbal ability. Verbal ability is a generic term that includes vocabulary, speech fluency, understanding language, and reading achievement and comprehension. We have already seen that differences between the sexes were not demonstrated before age two. Until very recently, it has been widely held that the difference in verbal ability began very early in life, and was well established in early childhood. However, data from a large number of studies dating from 1966 do not support such a belief (Maccoby and Jacklin, 1974). These studies, using standardized tests, do not reveal consistent results favoring girls until middle childhood, beginning around age ten or eleven. Throughout the school years girls outscore boys on tests of verbal skills.
We should emphasize that these results are based on tests of verbal ability. Few studies have measured the verbal behavior of children younger than three, although those that exist either find no difference or favor girls. While girls have a possible early advantage in the onset of speech and are ahead until about age three, boys do catch up. However, by middle childhood girls move ahead again and maintain their lead from then on. The magnitude of the girls’ advantage varies, depending on the nature of the task and other variables. An exception to the equality that begins to prevail at age three is found in studies of underprivileged children, where the girls maintain their advantage longer. It is suggested that, because of male vulnerability, a poor environment will contain more boys with systemic damage, which would tend to lower the average performance for their group.
Mathematical ability. Tests of mathematical ability include arithmetic operations, mathematical reasoning, and achievement in the formal topics of mathematics, such as algebra and geometry. Unlike verbal ability, mathematical or quantitative ability cannot be systematically observed before the fourth year, when such skills as counting or number comparisons can be measured. From this time through the preschool years, no gender differences appear. However, as with verbal ability, girls in disadvantaged populations are ahead of boys. Most of the studies tabulated by Maccoby and Jacklin found no gender differences before adolescence. When differences appeared they tended to favor boys consistently thereafter.
In recent years, the issue of gender differences in mathematics ability has continued to attract research and controversy. Tests of girls and boys in Grade 8 and again in Grade 11 found gender differences in Grade 11 where none had existed in Grade 8. Rather than attributing the girls’ decline to superior male ability, it was suggested that attitudinal factors, such as girls’ confidence in learning math and their perception of math as useful, accounted for the difference (Sherman, 1980). When these and other relevant factors, such as number of math courses taken, are controlled, “sex-related differences in favor of males do not appear often, and when they do, they are not large” (Fennema and Sherman, 1978, p. 201).
Of special interest are findings of the Study of Mathematically Precocius Youth conducted by Johns Hopkins University. Conducted in the Middle Atlantic area, the study participants were almost forty thousand seventh graders (twelve- and thirteen-year-olds) who scored in the top 3 percent on standard tests of verbal, mathematics, or overall intellectual ability. These highly selected children were administered the College Board Scholastic Aptitude Test (SAT), normally taken by juniors and seniors in high school. In addition, a nationwide talent search was conducted for Which any child under thirteen who was willing could take the SAT. The results of these procedures disclosed that, for this very large sample of children aged thirteen and under, far more males than females scored extremely high on SAT-M, the mathematics section of the SAT.
For the Middle Atlantic group, the average score for the males was thirty points higher than for the females. More striking, however, was the ratio of boys to girls among the high scorers. For example, for those scoring six hundred or higher (SAT-M scores range from two hundred to eight hundred) the ratio of boys to girls was 4.1 to 1. Scores above seven hundred on the SAT-M before age thirteen are quite rare. In the combined regional and national sample, the number of such boys was 260 and the number of girls was 20, a ratio of 13 to 1.
Such environmental explanations as social expectations, differential course-taking, and attitudes toward math to account for this very large gender difference are discounted by the authors of the study. Though they say that reasons for the difference are “unclear,” they strongly suggest that “endogenous influences” (i.e., biological) are responsible (Benbow and Stanley, 1983).
Reports of the Johns Hopkins studies have attracted considerable attention. Responding to an earlier report with similar results, two women mathematicians objected to the hypothesis of innate male superiority in mathematics, saying that environmental and cultural factors have not been ruled out. “Anyone who thinks that seventh graders are free from environmental influences can hardly be living in the real world.... [T]he issues of who helps with mathematics homework, of what sort of toys and games children are exposed to, of what the expectations of parents and teachers are, and of a multitude of other factors cannot lightly be set aside” (Schafer and Gray, 1981, p. 113). They also point out that the SAT is not a measure of “fixed capacities,” but is intended to measure aspects of “developed ability.” In addition, high SAT-M scores have not been shown to predict creative ability or later achievement in mathematics.
Finally, in spite of all the attention given to the surplus of males among the high scorers in the Johns Hopkins studies of mathematically talented youth, let us note that the same studies also discovered thousands of highly talented girls, who scored higher than most boys do. So, whatever the causes of the gender difference turn out to be, it is clear that mathematics and the female brain can be quite compatible. Some examples include an eleven-year-old girl who got the highest score in the mathematics entrance examinations at Oxford University in 1982; a seventeen-year-old who scored a perfect eight hundred on both the math and verbal parts of the SAT in the same year; and an eighteen-year-old who received her master’s degree in mathematics from John Hopkins in 1982 and became one of the youngest recipients ever to receive a Rhodes Scholarship to Oxford (Bleier, 1984, p. 104).
Spatial ability. Spatial ability is not simple to define, because it has been used to characterize performance on a wide variety of tasks. Usually it is held to mean the ability to see the relationships between shapes or objects or to visualize what a shape would look like if its orientation in space were changed. Tests for spatial ability use mazes, form matching, puzzles, copying block designs, or problems. Field dependence is a related cognitive characteristic which is considered to reflect mostly a spatial factor. It refers to a subject’s ability to separate or disembed an element in a display from its field, or background. The most familiar task used to measure field dependence is the Embedded Figure Test (EFT), in which the subject tries to find a certain figure hidden in a complicated background or picture. Persons who do well on such tasks are said to be field-independent. Of the studies reviewed by Maccoby and Jacklin, few found any gender differences in spatial performance in childhood. By age eight or nine, boys began scoring higher, and they were ahead from adolescence on.
Like other cognitive areas where gender differences appear to exist, the research on spatial visualization has likewise come under critical scrutiny. It.is pointed out that the “observed differences are very small, the overlap large, and abundant biological theories are supported with very slender or no evidence” (Kimball, 1981, p. 333). Some have questioned the legitimacy of research on gender differences in an ability so variously defined and measured as spatial visualization is (Caplan et al., 1985). This criticism is especially cogent when one realizes that spatial ability is held to be important for some occupations, such as architecture and engineering, and that scores on tests purporting to measure the ability might be used in career guidance.
Concerning other gender differences in intellectual and cognitive processes, three myths have persisted until recently. First, it was thought that girls were better than boys at rote learning and simple repetitive tasks, while boys were better at high-level cognitive processes. Second, many believed that boys were better than girls at analyzing and selecting elements needed for the solution of a problem. Third, it was believed that the intelligence of girls is more affected by heredity, of boys, by environment. However, studies show that girls and boys do not differ in any of these characteristics (Maccoby andjacklin, 1974).
Determinants of gender differences
Thus far, we have found some reported differences between males and females in the areas of verbal, mathematical, and spatial abilities. Let us now consider the explanations that have been put forward for these differences, specifically the biological and the environmental.
Biological factors. Research suggesting a possible biological basis for differences between boys and girls in verbal, mathematical, and spatial abilities concentrates on the following four influences: (1) genetic sex-linkage, (2) differential brain lateralization, (3) hormonal effects, and (4) maturation rate. Of the three areas in which cognitive gender differences have been fairly well established, spatial ability appeared to many researchers to be most likely to have a genetic component (Lambert, 1978). It was hypothesized that a genetic determinant for spatial ability was sex-linked, that is, that it was recessive and carried on the X-chromosome.
This means that if a boy receives the trait on the X-chromosome from his mother, the effect would manifest itself, since there is no dominant factor on his Y-chromosome to counteract it (remember that the Y-chromosome carries very little genetic material). On the other hand, in order for a girl to manifest the trait, she would need to receive it from both parents, in the form of matching recessive genes. If she received it from only one, the dominant factor on the other X-chromosome would suppress it. The prediction arising from this hypothesis, then, was that boys would score more like their mothers on tests for spatial ability than girls would. Numerous early studies did in fact report such parent-child correlations, but these have been shown to be flawed methodologically (Boles, 1980). In addition, the various definitions of spatial ability as well as the numerous tests used to measure it suggest that it involves complex cognitive processes that are very unlikely to be the expression of a single gene (Caplan, et al., 1985).
It now appears that, if there is a genetic component, it interacts in complex ways with socialization and cultural factors to produce the observable effect. Along this line, females’ lesser performance on spatial ability tasks has been held to account for their relative absence in such Helds as architecture, engineering, and mathematics. Yet their scarcity in these areas cannot be accounted for by the genetic hypothesis alone. By the rules of inheritance of X-linked recessive traits, half as many women as men would express the trait, yet we do not find nearly that many women in these fields (Lambert, 1978).
Since spatial ability is also important in some kinds of mathematics, it has been hypothesized that the gender difference in mathematical or quantitative ability could also be explained by the X-linked hypothesis (Stafford, 1972). But again, studies have not supported the heritability of mathematical ability; instead, they have implicated social and cultural factors (Fox et al., 1979; Sherman and Fennema, 1978).
Another suggestion of the role of biological influences in gender differences in cognitive abilities comes from research on brain lateralization. Brain lateralization refers to the extent to which the two hemispheres are specialized with regard to certain functions, for example, the extent to which language functions are processed in the left or right hemisphere or are bilaterally represented. There are competing theories as to the desirability of specialization of cognitive functions in one hemisphere, but the notion that spatial ability is superior when it is localized in one hemisphere has received much support in the literature. Along with this is the long-held belief that male brains are more lateralized than female brains are. These two notions, then, that “unilaterality is better” and that “males are more unilateral,” would account in part for male superiority in spatial, and possibly in mathematical, ability (Levy, 1972).
Both these ideas have been challenged in the contemporary research. For example, one study found that both hemispheres contribute to performance on the spatial task of copying a cube (Warrington et al., 1966). It has even been suggested that no skill is unilaterally based, but that both hemispheres appear to operate in all tasks (McGuinness, 1980). Another researcher said: “Many complex psychological functions depend on active cooperation between the hemispheres.... [T]he functional interaction between the hemispheres is cooperative rather than competitive” (Wolff, 1980, p. 251). The notion that the male brain is more unilateral and the female brain is more bilateral (less specialized) has also been eroded. For example, females recover better than males from loss of speech following a stroke, and this has been held out as proof of females’ greater bilaterality for verbal functions. But females often have better developed verbal ability than males have in the first place, and this could facilitate their quicker recovery following injury (Sherman, 1978). Also, if males are more lateralized for certain functions, then injury to, say, the right hemisphere should result in greater deficits for them than for women, and such has not been shown to be the case (Hier and Kaplan, 1980). In fact, one researcher has stated that “enough studies are listed favoring greater female asymmetry to justify discarding the thesis that the female brain is more bilaterally organized” (Martin, 1980, p. 243).
The possibility that the sex hormones may be implicated in the sex-related differences in cognitive abilities has also intrigued some researchers. Persons with the androgen-insensitivity syndrome and females who had been masculinized in utero by excessive amounts of androgenic hormones, both described in the last chapter, have been studied in this regard. The genetic males whose bodies are insensitive to the androgenic hormones produced by their testes have spatial scores that are more similar to those of females, whereas the androgenized girls have higher spatial scores than those of girls in general (Lambert, 1978). Some evidence suggests, however, that there is an optimum level of androgenization for maximizing spatial skills, beyond which a negative effect occurs. One study looked at the relationship of physical measures of sex hormone influence, such as body shape, the ratio of muscle to fat as they are distributed in the body, penis or breast size, and pubic hair distribution, to cognitive performance in both males and females. The more androgynous males (less stereotypically masculine on the above measures) were better at spatial skills than were their more masculine peers; likewise, the more androgynous females were better than their very feminine peers (Petersen, 1979). At the present time, the research on the relationship of hormones to cognitive functioning is limited, and some results, such as those just described, are not yet understood (Petersen, 1979).
Finally, it has been suggested that sex-related differences in some cognitive functions reflect different rates of maturation in females and males. In one study of early and late maturing girls and boys, the late maturers of both sexes scored higher on spatial ability tests. Since physical maturation is affected by endocrine function, these findings may be linked to the hormonal studies mentioned above. The maturation effect is particularly intriguing, given the observation that girls mature on the average about two years earlier than boys do. If later maturation is related to better spatial ability, this would help explain boys’ somewhat better performance on spatially-related tasks (Waber, 1979).
Thus we see that the research on four possible sources of biological influence on gender differences in cognitive abilities turns out to be either unsupported or inconclusive. The basic question underlying the issue of biological differences is, Are male and female brains different? Given the very small observable differences in cognitive performance, the obscure sources of such variation, and the problems noted with much of the research, perhaps we should ask instead, “Why do we find so much similarity?” (Martin, 1980). Above all, we remember the almost infinite malleability of human behavior as it is shaped in various environmental contexts, such that what we learn becomes competitive in importance with the contingencies of our bodies.
Environmental influence. The influence of the sociocultural environment on the psychology of women is dealt with in various connections throughout this book. At this point we are concerned only with its influence on intellectual abilities, especially those where females and males are somewhat different. Cross-cultural studies are particularly valuable for such an assessment, because of the following reason: if sociocultural factors are important influences in the development of gender differences in cognitive abilities, one would expect to find variation among different cultural groups by the fact that cultures differ. Since differences in spatial ability have been thought to be the most likely to reflect biological sex differences, let us consider its distribution by sex in other cultures.
Field independence, the ability to separate a form or object from its background, reflects primarily a spatial ability. Using the Embedded Figures Test, field independence was measured in the Temne of Sierra Leone, an African culture group, and in a group of Canadian Eskimo (Berry, 1966). The Eskimo showed greater field independence than the Temne, with no gender differences. Both Temne males and females were more field dependent, but the females were more so than the males. Two explanations exist for this interesting finding. First, field independence had survival value for the Eskimo whose environment was bleak with little variation or contrast. A group dependent upon hunting for subsistence would need to develop the ability to discriminate small differences in the visual field and to be able to orient themselves directionally with minimal cues. For ecological reasons, the Temne did not have this requirement, their setting being much more variegated, and their primary occupation, farming, required little skill to find their way around in the bush.
Second, the socialization practices of the two groups contrasted sharply with each other. The Temne emphasized severity of discipline and conformity. Wives and children were firmly controlled by the males. Eskimo children, on the other hand, received unconditional love and approval, were rarely punished, and were encouraged to assume responsibility. Both wives and children had a considerable degree of autonomy.
This study suggests the importance of both physical environment and socialization practices. The greater spatial ability as manifested in field independence of the Eskimo regardless of sex can be attributed to qualities in the physical environment which made a requirement of this ability. However, the absence of gender differences in the Eskimo, but their presence in the Temne, require further explanation. Here, the consensus seems to be that socialization practices that foster autonomy, independence, and relative freedom from parental domination also facilitate the development of field independence as a cognitive spatial ability (Kagan and Kogan, 1970). Where cultural and gender differences appear, they may reflect a difference in the distribution of power: parents versus children, male versus female. Among cultural groups in which power and dominance relationships are not an issue, spatial ability might be expected to be more evenly distributed in the population, and to be more heavily influenced by factors other than sex. In any case, crosscultural evidence suggests that socialization practices have some effect on differences in spatial ability.
Some researchers in the field have recently suggested that it is not sex but rather gender role which influences differences in intellectual functioning. Boys as well as girls who identify themselves as masculine have higher spatial scores. Likewise, when girls were asked their gender preference, those who wished to be boys had higher spatial scores than than those who preferred to be girls. The girls who wished to be boys had scores as high as did the boys who preferred to be boys. It appeared that male gender preference was associated with high spatial ability in both sexes. One explanation for this is that spatial tasks are usually male-identified, so that girls who see themselves as or wish to be masculine would be more motivated to do well on a gender-incongruent task (Nash, 1979).
Finally, gender differences in performance on the Embedded Figures Test, a spatial measure, can be eliminated by training. Pre- and post-test forms of the test were administered to males and females aged thirteen to sixteen. Though males did better on the pretest, a single practice session eliminated gender differences on the post-test (Tobin, 1982). This indicates not only the malleability of spatial abilities as measured by tests but also further calls into question any innate difference, which presumably would be more resistant to change.
We see from these contextual and environmental studies that spatial ability, however defined and measured, is multidetermined. Many factors interact to produce behavior. They may come from several sources, their contributions not all or nothing but a matter of degree. Sex alone accounts for only a small fraction of the variability in spatial ability found in any population. Here again, more meaningful results might be attained by studying the distribution of spatial abilities in girls and boys separately, and identifying those factors which are associated with, for example, high and low spatial ability in each sex independently.
The evidence for biological contributions to males’ superior performance in mathematics is weak, and the accumulating evidence is more supportive of socialization factors, particularly those related to gender role. The social worlds of boys and girls are different. With respect to mathematics, society generally assumes that males will dominate. For example, it has not been uncommon to find teachers encouraging boys more than girls in this area. This can lead to conflict and anxiety in bright girls. On the one hand they know that they could do well in mathematics, but they receive a different message from society. Because of the ensuing anxiety, girls often avoid the issue and choose instead courses that are seen as more gender-congruent for them. The stereotype that math is for boys also affects the agents of socialization: families, teachers, the media, textbooks. Pressures from these sources tend to limit girls’ options and reduce their self-confidence (Fox et al., 1979).
Studies of causal explanations for gender-related differences in verbal skills are few. Most of these focus on reading, a higher-level verbal ability. Fathers and sons tend to sex-type reading as a feminine activity; and this could lessen interest and motivation, since boys are under pressure to eschew participation in any part of the feminine role. Not surprisingly, boys who view reading as a masculine activity read better than do boys who see it as feminine. Furthermore, cross-cultural studies have yielded important data for the role of sex-typing of reading as it affects skill acquisition. In England and in Germany, both countries where reading is a male-appropriate activity and where there are more male elementary school teachers than in our country, boys have higher reading achievement scores than girls. This is very promising evidence for the part played by sociocultural variables in verbal abilities (Nash, 1979).
We have seen that sex-related differences in cognitive abilities do not emerge until late childhood or early adolescence. Also, the major differences occur in intellectual domains that are sex-typed, that is, identified with one sex more than with the other. Is there a connection between the time frame within which differences emerge and the sex-typing of the areas wherein they are found? Prior to adolescence, girls, especially, experience few sanctions against displaying cross-sex interests and behavior. But adolescence brings for both sexes stringent new role requirements as heterosexual relations emerge as salient and the meanings of one’s gender identity illuminate the whole spectrum of behavior. “Yet, uncertainty regarding numerous new role demands, the salience of sexual maturation, and a heightened self-consciousness ... results in a retreat to the safety of stereotypes learned long ago” (Nash, 1979, p. 288). So prescriptions for behavior become important as identity markers, accounting for the well-known conformity of early adolescents to their peer groups. It is reasonable to assume that this “retreat to stereotypes” can apply to the steering of interests into gender-appropriate areas, as defined by the culture.
That many resist such pressures is a reminder of the inadequacy of many of our generalizations. The point is that abilities and behavior patterns are not dimorphic for sex. To repeat, for any human psychological trait there is great overlap between the sexes, and the differences within each sex are greater than are the differences between the sexes.
Social and affective behavior
Stereotypes about the ways that males and females are or ought to be as they interact with others in the social world are even more numerous and persistent than are those held to describe their intellectual differences. In our society females are supposed to inhibit aggression and sexual urges, to be passive, nurturant, attractive, and to maintain a poised and friendly posture with others. Males should be sexually aggressive, independent, and suppressive of strong emotions, especially anxiety. This discussion will concentrate on a few areas which seem especially important for the psychology of women, areas that not only have attracted much research attention but also have served as focal areas for strongly held beliefs about the differences between males and females. These areas are fearfulness and anxiety, dependency, nurturance and maternal behavior, and aggression.
Fearfulness and anxiety. Most of the research does not make a definitive distinction between fear and anxiety. At the physiological level, they are closely related to each other. Both describe an arousal state which includes body changes, such as increased heart and respiratory rates, trembling, muscle tension, and sweating. Studies of fearfulness in children usually refer to a specific object or situation, such as fear of strangers or fear of being left alone. Anxiety often means a more generalized state of arousal, sometimes with nonspecific causes. A highly unpleasant state, anxiety is sometimes described as a feeling of impending disaster or of threat to one’s wellbeing or self-esteem. People differ in their readiness to experience anxiety. Some become anxious only rarely or in certain situations such as stage fright; others feel anxious most of the time. All persons at times experience both fear and anxiety. Those who have a generally fearful outlook on life, who are timid and hesitant in their approach to most situations, and who have frequent and intense anxiety are impaired in their psychological functioning. Research on gender difference in fearfulness and anxiety uses three basic methods: observation of subjects’ behavior in certain situations, subjects’ self-report of their feelings, and physiological measures.
Studies of children who have not learned to read and write have used reports of observations by parents and teacher rating scales. For example, one classic study had parents keep a diary for three weeks of all the occasions when their children showed fear. In another study two- to six-year-old children were asked to do “frightening” things: approach a large dog, walk on an elevated board, go into a dark place, or investigate a loud noise. In neither of these studies was there any difference in the frequency of fear responses of boys and girls. In the latter, however, the girls were seen as displaying a greater intensity of fear than the boys. In other words, those girls who were afraid were more afraid, according to the observers, than those boys who were afraid (Jersild and Holmes, 1935). More recent observational studies have not found consistent differences in fear or timidity for boys and girls (Maccoby and Jacklin, 1974).
With subjects who can read and write, the most frequently used method of assessing levels of fear and anxiety is some kind of selfreport. Typically the subject is presented with a set of items which reflect fearful and anxious feelings and behavior, such as “I am nervous about being alone at night,” or “I am afraid of dying.” There are many such inventories to measure anxiety in both children and adults. Of twenty-six such studies on subjects aged six and over, nine found no gender differences. Where differences were found, girls scored higher (Maccoby and Jacklin, 1974).
There are several possible explanations for these results. The first is that females are more fearful and anxious than males. But there are at least two reasons why this conclusion may not be valid. The first is the possibility that girls are more willing to admit to such feelings than boys are (Hill and Sarason, 1966). Related to this is also the possibility that some of the tests are weighted with items that are closer to the kinds of things that boys get anxious about, thus arousing their defenses more and eliciting negative answers. For example, an item such as “Are you afraid something might happen to your body?” might arouse castration fears in more boys than girls, but the boys’ defensiveness about castration fears could cause them to respond in the negative. Another suggestion is that the tests might be weighted with items that are more likely to elicit anxiety responses from girls. Girls are constantly being warned about strange men, lonely places, and other possible risks of sexual molestation. Such warnings and the fear they generate could generalize to other men, such as the doctor, and to a variety of unusual settings. One forty-five-item test had ten items that were believed to elicit such fears. Such a test would be biased in favor of higher scores for girls (Maccoby and Jacklin, 1974).
Whether girls are in fact more fearful or anxious than boys are, or whether they are just more willing to admit to such feelings, there is no evidence for any innate gender difference in this characteristic. Rather, socialization factors emerge as quite salient. Caretakers may have a more protective attitude toward girls, and their expressions of fear may be more tolerated because of cultural stereotypes about female timidity and relative weakness. Boys, by contrast, are taught early on to inhibit fear responses and to be brave in the face of danger.
Some attempts have been made to learn about gender differences in anxiety by measuring the physiological responses of the body to induced fear. Subjects in the laboratory may be told that they are going to receive an electric shock or that they must take an important intelligence test. The body changes associated with anxiety are then measured. While some differences in physiological arousal have been reported, their relationship to fear states is not known (Duffy, 1962). Such measures are not strongly related to self-report measures; that is, subjects with the strongest body arousal do not necessarily make the highest scores on an anxiety inventory.
In conclusion, the research on fear and anxiety indicates that females report themselves as more anxious than males. While they may in fact be more susceptible to anxiety, it is also likely that greater willingness to admit feelings, and factors in the tests themselves, contribute to the findings. Observational and physiological studies have not revealed differences in behavior or body changes.
Dependency. Infant studies of dependency behaviors such as seeking proximity with the mother, touching, and clinging, did not reveal gender differences. Studies of dependency in older children have dealt with a greater variety of behaviors, such as frequency of contact with teachers, help seeking, proximity to age-mates, and social interactions with adults and peers. Such studies usually rely upon observation, teacher or parent ratings, and self-report questionnaires. For example, three- and four-year-old children were given a puzzle that was too difficult for them to solve to observe their coping behavior. Boys were more likely to become emotional and disorganized, and more of them sought help with the problem. Girls asked for information, continued attempts to solve the problem alone, and sought contact with the experimenter (Zunich, 1964). It was interpreted that the girls were more dependent in this study. However, others pointed out that the girls’ contact-seeking was a coping attempt rather than an escape from threat (Maccoby and Jacklin, 1974). A review of eight observational studies of children’s dependency behavior with adults other than family revealed that five of them found no differences, while the rest were inconsistent (Maccoby and Jacklin, 1974).
Studies which use ratings as contrasted to direct observation of behavior more often find girls higher in dependency, leading these reviewers to caution against over-reliance on such measures. A culturally imposed bias to perceive girls as more dependent than boys could operate to influence ratings in that direction. For example, if a teacher is asked to rate each child in her class for dependency on a five-point scale, her cultural assumptions about dependency in girls and boys could bias her ratings so that the girls appeared more dependent than the boys. The fact that dependency is less pejorative as a descriptor of girls than of boys would tend to enhance this effect.
Studies of social interaction with peers and affiliative behavior have revealed some different trends for boys and girls. Boys have been found to have more extensive social interaction with age-mates, and to play in larger groups in middle childhood, while girls of similar age are more likely to have intense personal relationships with one or two close friends (Waldrop and Halverson, 1973). Further evidence that girls’ friendships involve greater intimacy was found in a study of self-disclosure or the willingness to be open with others in a self-revealing encounter (Rivenbark, 1971). Both sexes were more self-disclosing to their best same-sex friends than to their best opposite-sex friends, but girls were more disclosing to both male and female friends than boys were. Also, girls disclosed more to their mothers than boys did to their fathers. In a related study, it was found that girls would permit more areas of their bodies to be touched by female and male friends, and by parents, than boys would (Jourard, 1968).
These studies support a generalization that girls are more interested in the personal qualities of relationships and are more comfortable with intimacy than boys are. Other research found girls more oriented toward the gentler aspects of interpersonal relations and less toward the active aggressive possibilities. Also, they became interested in boys at an earlier age than boys became interested in them, and cared more about their personal appearance (Maccoby, 1966).
Although varying in definitions of dependency, more studies End females to be higher on measures of dependency behavior (Mischel, 1970). A longitudinal study of forty-four males and forty-five females over a twenty-five-year period found that dependency was a stable dimension for females but not for males (Kagan and Moss, 1962). That is, girls who were considered to be dependent as children continued to be seen as dependent as they matured, while dependent boys did not necessarily grow up to be dependent men. It is reasonable to assume the cultural pressures operate differentially on the sexes with regard to dependency behavior. The experimental data suggest that one sex is not more emotionally dependent than the other during the first few years of life, but a continuation or persistence of dependent behavior is less likely to be tolerated in boys. If such behavior in girls is viewed more benignly by parents and reinforced later by males who are socialized to be helpful and to alleviate distress in females, then its continuity into maturity, such that those girls who were dependent grow into women who report themselves to be less self-sufficient and higher in need to be cared for, is not surprising.
While such findings propose different trends for the two sexes in various kinds of behavior commonly thought to reflect dependency, they cannot be interpreted as conclusive evidence for sex differences in dependency. The biggest problem in understanding the meaning of the research results was mentioned in the discussion of dependency in infants. Researchers in a general area of behavior, such as dependency, include different behaviors in their conceptualization, and use different methods for obtaining knowledge about the occurrence of such behaviors, with the result that inconsistencies and inconclusive results are common. Also, there is no consistent agreement on just what behaviors under what conditions constitute dependency. Whether a greater interest in intimacy in relationships is a sign of dependency is a matter of definition.
An example of terms being defined differently is the following: sometimes attachment is used to signify those behaviors that seek to maintain proximity and to resist separation, and dependency is reserved to mean physical dependency, as of the infant (Bowlby, 1969). The term dependency has negative connotations, implying that it is culturally undesirable and should be eliminated from the child’s repertoire. Attachment behavior, by contrast, is natural and functional for humans. Its continuation into adult life does not necessarily imply psychological pathology. Separating attachment behavior from the dependency concept would allow for more precise definition and would rid the research and its interpretation of the negative meaning which dependency gives it.
This approach is of special interest to studies of gender differences. If dependency, including all the behaviors subsumed under it, has pejorative connotations and if more studies find girls dependent, then it follows that the pejorative connotations become associated with girls and their behavior. The statement, “girls are more dependent than boys,” has a certain stigma for girls, because in our society “dependent” qualities are less valued than “independent” qualities in behavior. The illogic of this is apparent when one looks at the behaviors that are considered to reflect “dependency” in the research. Some of them, such as interest in the interpersonal qualities of relationships and greater willingness to be open and self-disclosing, are positively valued even though the dependency rubric has meanings which are not. Future researchers in this area might do well to look more closely at the twin problems of definitions and values which characterize the literature on dependency.
Nurturance and maternal behavior. “Nurturance” means a readiness to give care and comfort to others, especially to those whose condition manifests such a need: the young, the weak, the sick. Much maternal behavior is nurturant involving taking care of and ministering to the needs of infants and children. Women throughout the world have always been far more likely than men to perform such a role and to be perceived as more nurturant by nature than men are. To the question, “Which sex is observably more nurturant?” on the basis of actual behavior, the answer is obvious. The question whether females have a greater readiness to be nurturant, perhaps on a biological basis, is more difficult to answer. Because of the current interest in women’s roles and questioning of the traditional assignment to women of child care, the research in this area of gender differences may be the most socially relevant of all. Do males ever display nurturant behavior, and if so, under what conditions? Is it feasible to consider a restructuring of society to include male involvement in the care of children, or is there a fateful bias that would run counter to such a shift?
Because of the biological relationships between humans and other mammals, it is interesting to study the extent to which nurturant behavior in animals is sex linked; that is, the extent to which it is inevitably linked to the female condition, by hormones or other biological mechanisms.
The development of maternal behavior in rats is partially under hormonal control, but it is also affected by experience. It was shown that virgin females treated with blood plasma from females who had just given birth would develop such maternal behaviors as nestbuilding and licking and retrieving pups in about half the time it took untreated virgin females. This study also found that pregnant rats increased their maternal behavior toward other pups, but that the increase did not appear if the ovaries were removed. But experience with the young was also a factor. Both males and virgin females, deprived of gonads, developed maternal behaviors after a few days if presented with a fresh litter of pups each day. This finding suggests that there is a base level of readiness to respond to young that is independent of hormonal control and can be elicited by the stimulus of contact with the young (Rosenblatt, 1969). Another study reported that the adult male’s aggressiveness toward pups diminished after several fresh litters were supplied, and that nurturing behavior then appeared (Rosenberg et al., 1971).
The response of preadolescent rhesus monkeys to infants revealed that when young male-female pairs were presented with an infant, the females showed four times as much positive behavior toward it, including body contact, grooming and play, as the males did. The males, by contrast, showed ten times as much hostility to the infant (Chamov et al., 1967). In an earlier study if only a male was available, the infant persisted in its attempts to make body contact and eventually the male relented and held it for long periods (Harlow, 1962).
Child-care participation by males varies much among subhuman primate species. For example, one study described a high level of involvement with juvenile care among young male hamadryas baboons. In that group, males display nurturant behavior toward the young before they themselves are adult (Kummer, 1968). This childcare rehearsal seems to be preparatory for the male adult role, which includes a protective attitude toward his first consort, a juvenile female. His “maternal” behavior toward her seems to be a continuation of earlier practiced behaviors toward the very young of the group.
Such studies of other species indicate that nurturant behavior is promoted to some degree by the sex hormones so that the females have a greater readiness to release such behavior when stimulated by the presence of young. Both sexes have the potential for appropriate child-care responses, however, and both virgin females and males can develop nurturant behavior with continued exposure to infants, although in some species male aggressiveness toward the young competes with the development of more positive behavior. When adult males participate in the care of children, as in the hamadryas, the juvenile males also show interest in them.
In humans very little is known about gender differences in nurturing potential. In most societies little girls receive early training for the mother role. In Indonesia they become surrogate mothers for their infant siblings when they are still children themselves. In our society they have dolls to play with to imitate the rituals of their mothers as they care for real babies. Given such initiations beginning early in life, it is dif ficult to learn what the contribution of nature is. Certainly among humans both sexes are able to behave in nurturing ways toward the young. Given that some base level of potential exists for both, it may be that the behaviors are simply elicited and reinforced earlier and more consistently for girls. Does male aggressiveness inhibit nurturing behavior in humans? The only hint of an answer to this question comes from observations of the androgenized girls reviewed in the last chapter (Money and Ehrhardt, 1972). These girls were reported to be less interested in dolls than their non-androgenized sisters were. Their interest in dolls was not measured systematically, however, but was based on their mothers’ report. Since the mothers knew that the daughters had been influenced by male hormones, their observations were likely to be affected. Furthermore, girls differ greatly in their interest in dolls and doll play.
One study provides a sequel to the research on the nurturant behavior in childhood. Its findings challenge the often-repeated assertion that men are naturally uninterested and inept when exposed to newborn infants. Fathers and mothers of newborns were observed in the hospital. When the baby was brought in, the nurturant behavior, looking, holding, smiling, rocking, of each parent was observed. Except for smiling, fathers exhibited more such behavior than mothers did. When the parents were observed separately with the baby, fathers were at least as nurturant in their behavior as mothers were. The sample consisted of two groups of different backgrounds. The first group was well educated; and half the fathers had attended classes in childbirth and some had been present at their child’s delivery. The second group observed was in a working-class hospital; the group was racially mixed. None of the fathers in this group had been present at his child’s birth. Yet all displayed interest in their infants, and a high level of nurturant behavior (Parke et al., 1972).
The question of the basis for and the relative strength of nurturing behavior in women compared to men continues to be the subject of vigorous debate. Since women are having fewer children, and some are choosing to have none at all, less of their lives is bound up in the nurturant role. Also, as mothers are increasingly occupied outside the home, their babies and children are being nurtured by mother surrogates, as they have traditionally been in some other parts of the world (Kitzinger, 1978). Roles, too, are blurring, so that young fathers may be more involved in the care of their children than were their own fathers. For many, these changes may be superficial and may reflect necessity rather than desire, having nothing to do with natural proclivities, let alone parental instincts.
Some wonder if these egalitarian trends, accompanied by assertions that mothering is not for women alone and that fathers too can nuture their young, are not going against nature. Even feminists have been taking a second look at possible biological contributions to women’s ubiquitous involvement in infant and child care (Lambert, 1978; Rossi, 1977, and in Goy and McEwen, 1980). Feminist sociologist Alice Rossi, noting that 99 percent of human tenure on earth has been spent in hunter-gatherer bands, has asserted that the sexual division of labor, whereby lactating women carried and cared for babies and young children, was adaptive for group survival and therefore became genetically embedded in the species (Rossi, 1977). Changes in social forms do not wipe out such predispositions. After examining the evidence for a biological potential for greater maternal investment in the child, exceeding any paternal investment, she concluded that an egalitarian ideology would run into profound difficulties when applied to child-rearing. Social and technological interventions that tend to minimize gender dimorphism in fundamental aspects of human life have the potential for interfering seriously in the process of mother-infant attachment—with critical implications for such human welfare issues as child abuse, delinquency, and other kinds of social and individual psychopathology. While not a call for a return to the asymmetries of traditional family roles, Rossi’s proposal is for a better understanding of the possible biological substrates for the primary mother-child dyad.
A further example of the widely disparate positions taken by feminists on the nature-nurture spectrum is the recent work of psychoanalyst Nancy Chodorow (1978). She examined Rossi’s (and others’) “argument from nature” and the role-training argument (girls “learn” mothering by observation, imitation, and subtle ideological coercion) and found them either unsupported or too simplistic in their data and theoretical formulations. Instead, she has developed a psychoanalytic analysis to explain the pervasiveness of mothering by women:
Women’s capacities for mothering and abilities to get gratification from it are strongly internalized and psychologically enforced, and are built developmentally into the feminine psychic structure. Women are prepared psychologically for mothering through the developmental situation in which they grow up, and in which women have mothered them (p. 39).
She argues that development in the infantile period, particularly the resolution of the oedipus complex, entails different psychological patterns, which attentuate possibilities for parenting in boys, and enhance and extend them in girls. Because mothers have themselves been girls and have been mothered by women, they tend to sense a oneness and continuity with daughters, experiencing a daughter as an extension or double of the mother herself. Thus girls continue to remain part of the primary mother-child relationship longer, continuing the preoedipal attachment characterized by primary identification with the mother. Boys, by contrast, are experienced by their mothers as “male opposites,” and are more likely to have been pushed out of the preoedipal relationship, having to curtail their empathic tie with their mother and to develop a more differentiated self.
Girls’ identification processes are more continuously mediated by their ongoing relationship with their mother, whereas boys’ are discontinuous owing to the necessity for them of earlier resolution of the oedipal conflict. Since girls do not need so strongly to deny preoedipal relational modes, continuation of or regression to these modes is not such a threat to their egos. They emerge, according to Chodorow’s theory, with a basis for “empathy” built into their definition of self in a way that boys do not: “Because women are themselves mothered by women, they grow up with the relational capacities and needs, and psychological definition of self-in-relationship, which commits them to mothering. Men, because they are mothered by women, do not. Women mother daughters who, when they become women, mother” (p. 209).
Finally, in an early precursor to Chodorow’s work, Margaret Mead, writing about the distinctions that societies make between boys and girls, suggested how boys raised by women must renounce their early experiences; and, poignantly, how girls raised with boys and men may hunger for theirs:
girls as well as boys may spend most of their time with men, busying themselves with masculine activities and pastimes. Or the children may spend most of their time with women. Then the boys also will learn to care for babies and cook, and they will go with their mothers and sisters to visit the newborn and mourn the dead. Later, all men will be left with a nostalgia for the childhood they shared with girls and women, but they will guard against it by renouncing all forms of tenderness, by speaking in loud, harsh voices, by making their stance aggressively masculine.... Or women may be left hungry for activity, ... restless when they are confined to their homes, and chafing against their feminine tasks of tending the hearth and caring for the children.... (Mead and Heyman, 1965, p. 100).
Aggression. The term aggression is used to apply loosely to a collection of behaviors whose general intent is to threaten or hurt another individual. In animal studies it usually covers acts of physical threat or attack, while in human studies it can mean these as well as negativistic, hostile acts, quarreling, and verbal abuse. The conditions under which aggressive behavior will occur and the sanctions for and against it vary widely across species, individuals, and cultures. A given individual often is inconsistent from time to time in his aggressive behavior even under similar conditions. Therefore an examination of the gender differences in aggressive behavior must begin with an understanding that such behavior, like other classes of behavior, has many sources of variation, of which sex is only one.
The evidence is very persuasive that males are more aggressive than females are. This generalization is supported by a large body of research including studies of a variety of human cultures and animal species. Reviews of more than a hundred studies of human sex differences in aggression revealed that males were more aggressive beginning around age two (Oetzel, 1966; Maccoby and Jacklin, 1974). In a cross-cultural analysis of differences in the behavior of children aged three to eleven, it was found that boys engaged in more rough- and-tumble play than girls, were more verbally aggressive, and were likely to react to an attack with counteraggression (Whiting and Pope, 1973).
Males are not only the instigators but also the recipients of both mock and serious fighting. Four-year-old nursery-school children were observed in a setting that included a large, inflated punching doll, a trampoline, and other stimulus toys. In this experiment, designed to elicit rough-and-tumble play, males were much more likely to playfully assault one another, wrestle, and hit the doll. Girls were more likely to play with the toys in nonviolent ways, suggest responsible rules, and await their turns with thè toys. Boys’ interactions had less verbal structuring and more unrestrained roughhousing, while girls’ contact with one another tended to be verbal rather than physical. The author thought that an interaction of social and biological factors could cause males both to emit and to respond to cues that are invitations to roughhouse, while girls might perceive the same cues as threatening (DiPietro, 1981).
Evidence from primate studies echoes observations on humans. Male ground-dwelling Old World monkeys observed in their natural habitat engaged in much more rough-and-tumble play than females did (De Vore, 1965). Such play in monkeys is a rehearsal for the adult role of dominance-seeking and defense of the group. Young male macaques (monkeys) reacted more aggressively to attack than young females did (Harlow, 1962).
At this point let’s insert a note of caution about extrapolating from such findings. The recent literature on primate behavior reveals much diversity in such behaviors as aggression and dominance among primate species, troops within species, and individuals, making generalizations about nonhuman primates almost as risky as it is with humans. A woman primatologist has written that female primates often do not conform to the “male-protected mother” stereotype, which ignores modern research that shows many female apes and monkeys to be “highly competitive, socially involved, and sexually assertive individuals” (Hrdy, 1981, p. 189) who protect territory, fight for their young, and, with other females, stand up to aggressive males. The point is not that female primates are as aggressive as male primates are, but that clear-cut differences, as with humans, do not exist, and that intra- and inter-species differences abound.
It has been suggested that differences in aggression are brought about by differential treatment of children (Feshbach, 1970). This argument rests upon the idea that aggression is an acceptable component of the masculine model in our society but is not desirable or appropriate when incorporated by females. It is thought that because of this differential valuing, parents reinforce or at least permit the display of aggression in boys and punish or discourage it in girls. This explanation for the observed gender differences in aggression has been challenged. A review of studies on parental permissiveness for aggression (Maccoby and Jacklin, 1974) revealed that there was no consistent evidence that parents were more tolerant of aggression in boys. There were some cross-sex effects, however. Fathers were especially severe in reprimanding sons for aggressive behavior, and were more permissive with daughters. Mothers, on the other hand, were more lenient with sons’ aggression or insolence than with daughters’. On the whole, the evidence does not support the hypothesis that differences in aggression are primarily the result of socialization practices. But if girls’ universally observed lower level of verbal and physical aggressive behavior is not altogether or mostly the result of social inhibitions, then what is its origin? One alternative explanation is that these differences between the sexes, variable and modifiable as they are, come from a biological substratum. Though not as potent a determinant for human behavior as for animal behavior, the theory could account for the consistency of the gender differences in aggression across cultures and human groups.
The contention that the differences in aggression have a biological basis is centered on the following points: first of all, males are more aggressive than females in all societies for which evidence is available; second, the differences appear early in life, around age two to two and a half at a time when the available evidence indicates no differences in parental reward or punishment for aggressive behavior; third, similar differences are found in both human and nonhuman species; and fourth, aggression is related to levels of sex hormones and can be changed by changing the levels of these hormones (Maccoby and Jacklin, 1974). We have already considered material relating to the first three of these points. Evidence for the last point comes mostly from animal studies of the relationship between the sex hormones and behavior (Lunde, .1973, and Money and Ehrhardt, 1972). A few examples are presented here to suggest a possible parallel between animal and human behavior.
As we saw in the last chapter, when pregnant females are administered male sex hormones, their female offspring show masculine patterns of behavior. For example, masculinized female rhesus monkeys engaged in more rough-and-tumble play than is usual for the young female of that species (Young, Goy, and Phoenix 1965). Such play is functionally related to later aggressiveness in animals, although no such relationship has been established for humans. In the “tomboy” syndrome of girls androgenized in utero, an increased level of such play was observed (Money and Ehrhardt, 1972). But the girls were not more aggressive in the sense of being antagonistic or hostile. The main component seemed to be an increased activity level with liking for vigorous outdoor play. In these studies, prenatal androgenization did not result in a higher level of threatening or assaultive acts toward others, the kind of aggression more frequently shown by boys.
The aggressive response of female monkeys treated with the male hormone testosterone from age 6/2 months has been recorded (Joslyn, 1973). Three treated females and three untreated males were placed together and observed for thirty minutes a day during three time periods, at ages 5–914 months, 1314–16 months, and 25–2714 months. Before the testosterone treatment of the females, the males were dominant and more aggressive than the females. After the treatment began, the females became more aggressive, and two of them attacked and subdued the two most dominant males. These two females maintained their dominance until the end of the study, long after the administration of testosterone was discontinued. Although the females became more aggressive vis-à-vis the males, their rough-and-tumble play did not increase; rather, the male rough-and-tumble play decreased from its earlier level. Thus the treatment of the female did not change her rough-and-tumble play, but did change that of her male playmate. A possible explanation for this is that the increase in aggression and dominance by the females had the effect of subduing the normal ebullience of the young males.
Some studies have shown correlations between levels of testosterone and aggression in males; that is, higher levels of testosterone have been found in more aggressive males, and vice versa. For example, one study revealed that male prisoners with higher testosterone levels had committed more violent crimes (Kreuz and Rose, 1972). On the other hand, there is some evidence that behavior affects testosterone level. When single male monkeys were placed with all-female groups, they immediately assumed the dominant role. Tested later, their testosterone level had risen to about four times its pre-experimental level. When these same males were placed separately with mixed-sex groups where the dominance hierarchy was already established and they had to assume a peripheral nondominant role, their testosterone levels dropped sharply (Rose et al., 1972). Thus in males the relationship between testosterone and aggression can work both ways. High levels of aggression can be both an effect and a cause of elevated levels of testosterone.
What do these data mean for explanations of gender differences in aggression in humans? The differences are real, but they cannot be accounted for by placing the sole responsibility on differential socialization nor by deducing a proposition that testosterone rules all. Aggression, like spatial ability, is not something that males have and females do not have. There exist aggressive and unaggressive persons, and in-between variations, in both male and female populations. The suggestion from the data on gender differences in aggression is that a biological substratum exists that predisposes males to be more aggressive in situations that elicit such behavior. The threshold for aggressiveness in males seems to be lower so that under certain stimulus conditions aggressive behavior is more likely to appear. The empirically demonstrated link between male hormones and active aggression, and the physical superiority of males in build, strength, and muscle mass provide a biological basis for a readiness to behave aggressively.
Yet in humans it is obvious that much behavior is acquired. Specific aggressive acts are learned, and the inhibition of such acts is also learned. Boys are probably more primed to learn them and in some environments are less likely to be taught to inhibit, while the reverse may be true for girls. Again, cross-cultural studies are helpful in gaining perspective on the issue. Although children regardless of sex are reported to show aggressive behavior in most societies, each society has its own way of dealing with it (Whiting and Child, 1953). And children, again regardless of sex, reflect their culture’s approach. As Margaret Mead showed, the Mundugumor reared aggressive, hostile children of both sexes. By contrast, today’s Chinese children, reared in state-run nurseries, are taught cooperative behavior and are not punished physically (Sidel, 1973). Observers marvel at the absence of hostile and aggressive behavior in their play groups.
Further evidence for the role of environmental influences in the acquisition of aggression as a personality trait in boys and girls appeared in a longitudinal study (Eron, 1980). Begun in 1960, this study of 875 third graders and their parents living in a semirural county in New York State demonstrated that the aggressive behavior displayed by the children in school was related to the learning conditions for aggression that were present in the home. The less nurturant and accepting the parents were, the more aggressive the child was in school; the more a child was punished for aggression at home and the less he or she identified with either or both parents, the more aggressive the child was in school. A major contributing factor for aggression seemed to be a lack of favorable support from both parents.
Ten years later, the researchers were able to study again almost half their original sample, about equally divided among boys and girls, now about nineteen years old. One of the most striking Hildings was the persistence of aggressive behavior (or lack of it) over the years. Children who had been rated aggressive by their peers at age eight continued to be rated as more aggressive by their peers ten years later (see Fig. 5.2). At this follow-up, although parental behaviors continued to be important, the single best predictor of aggressiveness for the nineteen-year-old young men was the rated violence of the television programs they had watched as eight-year-olds.
The differences between the boys and girls in this series of studies are especially interesting. Consistent with the other studies we have reviewed, the girls were much less aggressive at all times than the boys were. Also, the effect of early viewing of television violence and later aggressive behavior was either nonexistent for the girls, or went in the opposite direction; that is, girls who viewed more violence on television as children tended to be rated less aggressive as they matured. The authors thought that reasons for this gender difference include differential socialization whereby girls are less responsive to aggressive cues in the environment, and also the fact that in the 1960s there were hardly any female role models for aggression; rather, females in aggressive scenes were most likely to be victims. Related findings for girls, however, were that girls in the second wave of the study who expressed masculine interest patterns and who watched contact sports on television rated as more aggressive. In other words, when young females are aggressive, some of their interests and activities seem to deviate from those typical of their sex and to be more like those of males.
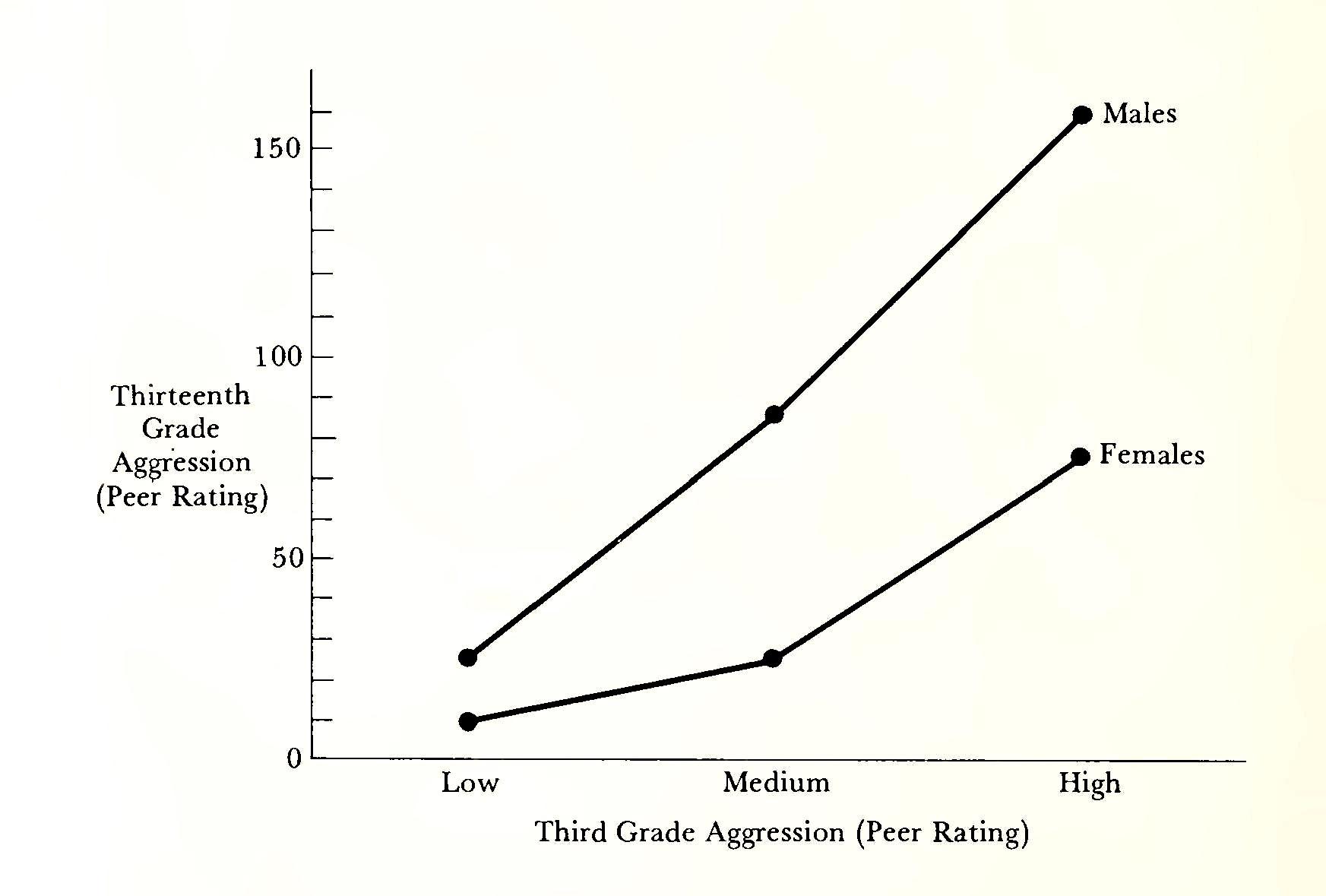
Studies currently being conducted by Eron and his colleagues on first- and third-grade children show that those who score high on preference for masculine activities, regardless of sex, are likely to be more aggressive, and that the effect is cumulative across time. One intriguing finding was that the more aggressive boys tended to have aggressive fantasies, that is, fantasies in which they daydreamed about fighting or killing someone. The more aggressive girls, however, had few if any such fantasies; rather, they fantasized about action—heroes and heroines, winning games, and achievement.
The author concludes from these studies that if we want to reduce the level of aggression in society we should begin to reward boys for unaggressive behaviors; that we should, in fact, socialize boys more like girls, encouraging the development of socially positive qualities such as tenderness, sensitivity to feelings, nurturance, and cooperation (Eron, 1980, p. 251).
What Do We Know about Gender Differences?
The foregoing discussion of psychological differences between the sexes has presented current knowledge in areas where differences have been shown to exist, and in a few others, where the findings are not conclusive and where misconceptions are common. Differences in other areas, such as achievement, will be discussed in other contexts later on. In general, then, we can conclude that:
-
Behavioral differences between boy and girl neonates have not been demonstrated.
-
Clearcut differences in cognitive ability and in social and affective behavior in the first two years have not been conclusively demonstrated. However, patterning of cognitive development is more consistent with age for girls, and is more strongly related to social class. Irritability and fearfulness are more consistent with age for boys. Mothers are equally warm, nurturing, and accepting of boy and girl babies.
-
Gender differences in cognitive abilities emerge in middle to late childhood. Girls have higher verbal abilities, and boys have higher mathematical and spatial abilities. Controversial explanations include both environmental influences and possible innate factors. The differences are so small, however, and the amount of overlap between females and males is so large, that most believe that they can be accounted for by the differential experiential histories and socialization of boys and girls.
-
The evidence for gender differences in fearfulness, dependency, and nurturance is inconclusive. Teacher ratings and selfreports tend to show girls more fearful, but it is not known to what extent cultural expectations and girls’ greater willingness to admit feelings affect these results. Girls seem to be more oriented toward intimacy in interpersonal relations, but they do not exhibit more of the behaviors usually included in definitions of dependency in the research. While girls are more often in a nurturant role, as in doll play, it is not known to what extent nurturant behavior is innate in females. Both males and females can display nurturant behavior. There is some evidence that early exposure of males to infants and child care enhances their nurturant behavior as they mature.
-
From early childhood, boys have a higher level of aggressive behavior than girls. This difference has been observed in other cultures as well as in animal species. It is possible that a hormonally induced pattern of readiness to respond aggressively, as well as other physical characteristics, contribute initially to this difference. Human behavior, however, is highly malleable, and within-sex and cross-cultural differences are significant also.
A Final Word
Including a chapter on gender differences in a book on the psychology of women risks reinforcing old stereotypes about boys and girls, men and women. But studies on such differences have a century-old history in psychology, which attests to their interest to social scientists as well as to laypersons. The reason for this may be that the dichotomy of biological sex makes irresistible the search for other absolutes that would neatly fit into the categories of male and female. But such absolutes in psychology do not exist. Regarding the areas we have looked at in this chapter, male-female differences account for only 1 to 5 percent of the variance in the population, so that sex is a very poor predictor (worthless, in fact), of what an individual’s performance in any of the areas would be (Deaux, 1984). More significant is the tremendous variability that exists within sex categories, such that the differences among females, for example, are many times greater than are the differences between females and males. More attention should be paid to individual differences within sex categories.
The next chapter will take up the role of society and socialization practices in the further development of gender differences and in the differentiation of social roles. But for now, we might best put our discussion of gender differences into perspective by considering the response of the eighteenth-century British writer Samuel Johnson, who when asked who was smarter, man or woman, replied, “Which man—which woman?”
6. Growing up female
I do not know a single girl who’s really satisfied with how she looks. Some toss their hair and smooth their skirts and stride like models, and I’ll start out envying them and mentally exchanging faces or shapes or hair color, but then I’ll watch them looking at other girls as they stride by tossing their hair, and I’ll see, in the faces I admired, the same sizing-up look that’s on mine (How much does she weigh? Does she color her hair? Curl her eyelashes?) and realize that not one of us feels really safe.
—Joyce Maynard. Looking Back: A Chronicle of Growing up Old in the Sixties, 1983
That night I dream I am dancing to Stevie Wonder’s song “Always” (the name of the song is really “As,” but I hear it as “Always”). As I dance, whirling and joyous, happier than I’ve ever been in my life, another bright-faced dancer joins me. We dance and kiss each other and hold each other through the night. The other dancer has obviously come through all right, as I have done. She is beautiful, whole and free. And she is also me.
—Alice Walker, In Search of Our Mothers’ Gardens, 1983
In India, a small Rajput girl plays at making bread. She builds herself a little hearth of three stones, pats and shapes her mud cakes, and fries them in a pan. When they are done, she stacks them on a dish, washes the pan, and sweeps up the floor where she has been working, all her motions an exact replica of those she has seen her mother use many times. Outside, her brother is “plowing” the ground with a stick. He says, “burr,” “burr,” which is what his father says as he walks behind the cattle (Minturn and Hitchcock, 1963).
Across the world a behavioral scientist comes upon a small Sioux girl sitting behind a tree. She is bent over a toy typewriter, and he notices that both her lips and her fingernails are painted red. Nearby, a young boy is lassoing a tree-stump buffalo (Erikson, 1963).
Everyone who has observed children from about age three on has seen such imitations of and rehearsals for adult roles, little girls doing what women do, little boys practicing to be men. Such behavior is sex-typed, that is, it is behavior that is considered appropriate to the child’s gender. All known societies prescribe certain behaviors for women, others for men, and these define not only gender roles but also concepts of masculinity and femininity. In Chapter 4 we saw that children learn their gender identity during their second year of life. By age three, they know what sex they are and also are able to classify others by sex. Subsequently they incorporate into their identities the preferences, interests, and behaviors that are identified with their sex in their society. Gender role identification is distinguished from parental identification, which is the internalization of the personality characteristics of a parent and the development of reactions and behavior similar to those of the parent. The process by which gender-identification and parental identification are acquired and the content of the socialization experiences that differentiate girls from boys are the subjects of this chapter.
How Children Learn
While there may be underlying biological predispositions for the acquisition of some sex-typed behaviors, we assume that the role of learning in a social context is far more important for developing gender-role identification. Given that the society has different gender-role models for males and females, how are these acquired by children? What factors facilitate or retard the identification with a gender role apparent so early in life? At the present time there is no consensual answer among learning theorists to these questions. Instead there are three major proposals to explain the learning of gender roles. The first emphasizes the role of reinforcement by rewards and punishments in establishing behavior. The second attaches importance to modeling, or imitating, the behavior of others. The third is a cognitive-developmental approach which stresses the child’s growth of understanding both of her or his sexual identity and the content of the gender roles prescribed by the society.
These three explanatory concepts of how children learn gender roles are not mutually exclusive. It is quite possible that all three contribute to the child’s acquisition and performance of sex-typed behavior. Also, although we are discussing them as they apply to sextyping, it should be understood that as causal principles they can apply equally to the learning of other social behaviors. There is no reason to believe that gender roles are learned under any different conditions than are other complex behaviors.
Reinforcement
Behavior, including gender-related behavior, can be acquired under conditions of reward and punishment. The term reinforcement is not easy to define, as it can be applied to a variety of events which may have little in common. For example: When a child learns not to use certain prohibited words because her mother spanks her for it, the spanking is the reinforcement. When a child appears before company clean, combed, and dressed up and is told that she looks very pretty, the phrase, “You look very pretty,” is the reinforcement. When a child brings home her first report card with all T’s and is given a new bicycle, the bicycle is the reinforcement.
Even though the spanking, the praise, and the bicycle seem to have little in common, they all act as reinforcers to facilitate learning. Reinforcers are considered to be positive if they represent desirable goals, so that the child will repeat the behavior which resulted in the reward. They are considered to be negative if they have aversive effects on the child’s behavior, so that she will refrain from the behavior in order to avoid the negative consequences.
An explanation of the acquisition of gender roles through reward and punishment would propose that as children try out various behaviors, they are rewarded for those that are appropriate and punished for those that are not. While there is no doubt that reinforcement is very important in the acquisition of behavior, it is too simplistic to account, by itself, for children’s learning of gender roles. The rate at which these roles are learned, and the scope of their content, require additional processes. Gender roles not only encompass broad areas of behavior but are often quite subtle as well: “It would be difficult to imagine that any kind of direct tuition could provide for the learning of such elaborate behavioral, attitudinal, and manneristic patterns as are subsumed under the rubrics of masculinity and femininity. Furthermore, these qualities are absorbed quite early and are highly resistant to modification” (Sears et al., 1965, p. 171).
Modeling
Modeling, or imitation, in the acquisition of sex-typed behavior is dependent upon observational and cognitive processes and can occur without any direct reinforcement. “People learn sex roles through their eyes and ears and by observing other persons and events and not merely from the consequences they get directly for their own overt behavior” (Mischel, 1970, p. 29). Such learning may occur from watching what other people do, observing the consequences of their behavior, attending to environmental events and to symbolic material such as stories and pictures. Through these processes the child develops the knowledge of her own gender identity, and learns the concepts of male and female, including cultural stereotypes of masculinity and femininity.
The concept of modeling as a major process in the learning of gender-related behavior implies that girls learn female role behavior by observing and imitating the behavior of other females. The hypotheses that come out of this proposal are several. First, because the mother is the most available, important, and rewarding female, she is most likely to become the role model, at least in the preschool years. Second, in selecting the mother’s behavior to imitate, the girl will become more like her than like the father; and third, same-sex models in general will be imitated more than opposite-sex models because the child perceives them as more similar to herself.
However, the importance of modeling in the learning of gender-role behavior is controversial (Maccoby and Jacklin, 1974). If the first hypothesis, contiguity of mother, is correct, it would lead to the conclusion that both sexes early in life establish their primary identification with her through observing and modeling her. But other research has shown that, when exposed to several models, children will imitate the more dominant one. Likewise, other things being equal, they will imitate the more nurturant one. If the father is dominant, then both sexes should imitate him, and if the mother is nurturant then both should imitate her. While this may actually be the case very often, it would not account for differences in acquisition of dominant or nurturant behavior by the two sexes.
Do very young girls learn feminine behavior by modeling their mothers and thus become like them? Available research does not support the hypothesis of parent-child similarity along a dimension of femininity or masculinity (Maccoby and Jacklin, 1974). A popular research technique for measuring sex-role identity and preferences in children is the IT scale. The child is given a card with a representation of a sexually ambiguous figure, asked to assign a sex to it, and to choose toys for it from objects or pictures associated with gender roles. Studies of gender-role similarities in parents and children have compared children’s performance on this scale with measures of femininity and masculinity of parents, to ascertain like-sex and crosssex identification in sex-typing of interests and preferences and so on. In one study the choice patterns of first-grade girls were unrelated to the femininity of their mothers. Likewise, boys’ responses were unrelated to their fathers’ masculinity (Mussen and Rutherford, 1963). While some studies show parent-child similarities on certain dimensions of personality, such as values and attitudes, they fail to show that the child is more likely to resemble her or his mother than father.
The third hypothesis suggests that same-sex models in general will be imitated more than opposite-sex models because of their perceived similarity to the child. Again, the research does not demonstrate this to be the case. A review of twenty studies in which children were presented with models of both sexes revealed little consistent tendency for preschool children to select same-sex models. When shown models who were displaying affection, aggression, toy choices, aesthetic preferences, and other activities, the children’s modeling was indiscriminate with regard to sex (Maccoby and Jacklin 1974).
The essential point here is that while children do learn through modeling, through observing and imitating the behavior of others, they do not limit their modeling in any systematic way to same-sex models. If they observe and imitate equally models of both sexes, then they acquire a repertory of behavior which includes both “masculine” and “feminine” components. These components, however, are not equally manifested in behavior. Girls display lower levels of aggressive behavior than boys do, prefer to play with other girls, and choose play activities that are defined as sex-appropriate. If modeling is of minor importance for such an outcome, then what are the reasons for it? Two explanations that require that the distinction be made between acquisition and performance have been suggested (Maccoby and Jacklin, 1974). We have already seen that a wide range of behavior can be acquired by direct reinforcement and by modeling. Some of these become part of the patterns of consistently occurring behavior for a particular child, and others do not. They may be tried briefly and then dropped or never tried at all. For example, the little Rajput girl may be as well able as her brother to “plow” the ground with a stick, but she does not do it. What she does do is to employ her toy dishes to make bread. The selection of such behaviors for actual performance depends on the necessary eliciting conditions, and the belief that the action is appropriate. Both the little Rajput girl and the boy had observed their mother making bread and knew what to do with the toy dishes, but the dishes had been given to the girl, not to the boy. Also, on the basis of observation and various reinforcing conditions, the child knows what is appropriate to her or his own sex. This last factor brings us to the third explanation for the way children learn about gender roles.
Cognitive-developmental theory
The cognitive view of the processes mediating the learning of gender roles states that gender-related behavior is learned neither by the simple reinforcement of discrete acts nor by the imitation of the actions of same-sex people. Instead, the child develops rules or generalizations from what she observes, and then applies these over broad classes of behavior (Kohlberg, 1966). In the early stages of this learning, the rules may be oversimplified and inaccurate, and the child may be unable to take into account the exceptions she encounters. For example, a young child who does not know yet that sex is constant has induced a rule that all persons who wear dresses are girls. When she is shown a male model in male attire, she correctly identifies him as a boy. Shown the same model in a dress, she now identifies him as a girl in accordance with her rule. Similarly, a young woman who lived for a while on a houseboat near a small country town became the object of curiosity to a five-year-old native, who did not know any adult single women, let alone any who lived on a boat. “Where’s your husband?” she asked over and over. “You gotta have a husband!”
The child’s knowledge of what constitutes masculine or feminine roles or behavior must undergo change and revision as she matures and has a greater breadth of experience. Once she learns what her own gender identity is, she then learns which other persons share that category with her. At the same time she is observing what all these persons, as well as those in the other category, have in common, within her experiential range. From these observations she learns what is appropriate to her sex, and begins to match her behavior to that gender-role standard.
These stages of identity development, learning of gender categories, and formulation of rules about gender behavior do not occur in any formal sequence. During the same time that her own gender identity is becoming firmly established, she is observing the similarities and differences in others that permit her to think of them in terms of categories with rules assigned to them. These rules are established and confirmed as a function of the consistency of her experience. Clearly the more rigidly defined are the roles in the society, the stronger her confirmation of the rules will be. Presented with an anomaly, as in the case of the five-year-old above, she must recast her whole formulation concerning adult women, from “All adult women have husbands,” to “Not all adult women have husbands,” or, “Most, but not all, adult women have husbands.”
An alternative cognitive model that includes elements of the three just described has been offered as a “working hypothesis” by Constantinople (1979). This model relies upon the young child’s ability to attend to, perceive, and remember differences in behavior that are relevant to sex. In this process the child develops expectations that carry over to new situations involving different people. Thus the child learns to extract the essential features that apply to sex as they appear in different contexts.
The first step, according to this model, is a labeling process whereby such words as boy, girl, mommy, daddy, frequently used by parents and others, would provide a structure for gender categories to develop. Such stimuli as “What a good boy,” and “What a pretty girl,” and similar identifications that the child hears over and over provide a mechanism for the development of gender identity, which is being formed during the same developmental period as language acquisition is occurring. Similarly, such labeling soon includes differential identification by verbal and nonverbal cues from others that shape the child’s behavior in the desired direction.
The major mechanism in the acquisition of these features seems to be a combination of observational learning and direct instruction, with linguistic labeling helping to organize the information in a way similar to that of pattern recognition in vision and speech. The patterned features that the child learns and refines as she gets older are then used to screen her own and others’ behavior in terms of its appropriateness to gender-role standards. With age and experience, more distinctions are learned and more subtle discriminations begin to be made. Too, the learning of gender roles may be facilitated by the child’s cognitive need for structure, which may be a reason that young children adopt stereotypes about gender roles so readily.
This model, which basically sees gender roles being learned as rules that are applicable across situations, and that are subject to refinement and testing across time, partakes of the three theories earlier described. The learning may occur directly by reinforcement or instruction, or indirectly by modeling or the deducing of generalizations. Its validity remains to be tested by research, although, as the author points out, the intriguing question, What is the source of the motivation to develop gender-role categories, seems to defy ethical resolution. It would require that children be reared without clues or cues for gender role save the basic anatomical and physiological ones, to see if those alone would be enough to enable the child to structure gender categories. But even if, hypothetically, an experimental group of children were kept in a state of innocence regarding their own sex-related gender roles, would not the ubiquity of such roles in society sooner or later entice them to make the connections that would answer for them the questions, Who am I, and How should I behave?
These theories, one emphasizing reinforcement, the second, modeling, the third, cognitive development, and the fourth, the learning of gender roles as rules, help to explain the ways that gender-related behavior, and identification with gender role, is learned. It is probable that all these processes are involved in the emergence of such behavior, in different degrees of importance, depending on the situation and the age of the child. Consider, for example, the four-year-old girl who gets “dressed up” for a brief appearance at her parents’ party. She is willing to do this because of a history of reinforcement with praise, approval, and warm compliments from adults when she “looks pretty,” a harbinger of things to come. She wears a long skirt like her mother’s and helps to pass the hors d’oeuvres, modeling from her mother the appropriate ways that a female behaves as a hostess. At the same time, she can see that all the other women are dressed similarly, and she can observe their tone of voice, their gestures, and the kinds of things they talk about. From this experience and numerous others like it she forms generalizations about the state of being female in her world. Several kinds of learning are occurring, each facilitating the other, to organize the child’s gender-role concepts and gender-related behavior.
These processes, operating together, offer potent explanations for children’s learning of gender-related behavior as it is culturally defined. But children are variable in such learning: all girls are not equally “feminine,” nor do all boys fit a “masculine” stereotype. Further, polarization of roles is greatest amount young people and decreases with age (e.g., Neugarten and Gutmann, 1968). ft may be psychologically necessary for many children and young people, who are trying to define themselves in a complex society, to discriminate themselves more rigidly from the other sex, while persons who become more sure of themselves and who they are as they mature can be more flexible and less concerned with the “appropriateness” of their behavior. Recent theorists had just such a developmental transition in mind when they proposed the idea that some women and men as they mature can transcend typical gender roles and become more flexible in their interpersonal and problem-solving behavior (Hefner et al., 1975). Behaviors once learned do not necessarily characterize the individual for all time; growth is a dynamic process, combining both stability and change.
Development of Gender-Role Identification
Three aspects are involved in the process of developing gender-role identification. They are (1) gender-role preference or the perception of the role of one sex as more desirable than the other, (2) genderrole adoption or the display of sex-related behavior, and (3) genderrole identification or the incorporation into one’s personality of the responses characteristic of a gender role (Lynn, 1959).
Gender-role preference
Gender-role preference is observed in both girls and boys beginning at about age three, and is well established by age five. Children younger than three are unlikely to show a preference for sex-related toys or activities or to attach a value to one gender role over the other. One study provided one-year-old boys and girls with a variety of toys in the presence of their mothers, including stuffed animals, a Ferris wheel decorated with pink ribbons, and robots. Except for the boys’ preference for the robots, no sex differences were found, and the mothers did not differ in their toy selections for girls and boys (Jacklin et al., 1973). By age three, however, nursery-school children show sex-related preferences for toys and activities. Little girls are in the doll corner, dressing up and playing house; boys are outside, tumbling about and fighting, and playing with cars and trucks.
In middle childhood, however, an interesting phenomenon appears, and continues to differentiate the sexes into adulthood: a widespread preference by girls of the masculine role, and greater ambivalence in girls for clear-cut identification with the feminine role. In contrast, boys do not show a cross-sex role preference, and they are more likely to identify unequivocally with the masculine role. A study of gender-role preference among Eve- and six-year-old boys and girls, using picture cards depicting various objects, figures, and activities associated with the masculine or feminine role illustrates this phenomenon (Brown, 1956). A child figure of no discernible sex (IT) was given to the subjects who then made choices for it from among the items. The study found dichotomous gender-role preference in these young children, but girls twice as often as boys showed a mixed preference pattern. The tendency to strong opposite gender-role preference was more pronounced in girls, and boys showed a significantly greater preference for the masculine role than girls showed for the feminine role.
Furthermore, when subjects could show a preference for being male or female, only One boy in ten chose female, while one girl in three chose male. This finding of preference for the male role by both sexes has been widely replicated for age groups extending into adulthood. Results suggest that between 20 and 31 percent of adult women,.compared to between 2.5 and 4 percent of adult men, recall a conscious desire to be the other sex (Brown, 1958; Sherman, 1971).
What factors contribute to this ubiquitous disenchantment with the condition of being female? Freud, of course, had a ready answer in the anatomical difference between the sexes, which he thought was clearly disadvantageous to the female and produced in her a profound envy of the male. Since the data do not support the concept of penis envy, one must look to sociocultural explanations. It is probable that girls perceive early the male role as invested with higher status and greater rewards.
Another explanation for females’ preference for the male role, however, is the fact that girls are freer to state a cross-sex preference. In addition, girls have much greater latitude to engage in a host of male activities, especially before adolescence. No onus is attached to tomboyish behavior; girls may wear pants and play softball, but no boy may wear dresses or play Barbie dolls with impunity. Thus the greater freedom girls have to display cross-sex preferences and behavior probably shows up in the research as a variable that interacts with actual preference to produce the most clear-cut results. But it is clear that the pressure is less great on girls to use sex-appropriate behavior.
Gender-role adoption
The second aspect of gender-role development, gender-role adoption, identifies observable, sex-related behavior. In girls, the adoption of the feminine role appears to occur concomitantly with gender-role identification. That is, at about the same time that the little girl begins to exhibit sex-typed behavior, she also begins to internalize the female role and its attributes. There is some evidence that for boys these processes are sequential. For example, five- to seven-year-old girls perceived similarities between themselves and their mothers, whereas boys of the same age had not yet established a like identification with their fathers (Ward, 1969). One explanation for this is that the course of the identification process is different for the two sexes.
We have already seen how role adoption, the display of gender-related behavior, is learned as a function of reinforcement, modeling, and the development of concepts about what is appropriate for one’s sex. We are now going to consider a model for the development of gender-role identification.
Gender-role identification
The first parental identification of both sexes is with the mother, who is the usual omnipresent caretaker. The boy, not the girl, must make a shift in identification with the appropriate gender-role. This shift can be difficult, since his father is typically away much of the time, and the adults of his early social world are mostly women. Thus girls continue to elaborate their early parental identification because the behavior of their mothers is female role behavior. However, boys must learn to identify with a culturally defined model whose components may be less than clear to them for a very long time. Evidence suggests that both sexes identify more clearly with the mother throughout childhood, but males’ identification with her is more likely to be revealed in personality variables that are not sex-typed. Sociability and preference for being with people as contrasted to being alone are two such examples. The girl learns her identification within a close interpersonal context, by imitating her mother as a model.
The boy has a more difficult problem. He has to define the goals of the masculine role, learn what its components are often by being told what they are not. Finally, he must abstract from this set of conditions principles that can guide a large number of behaviors. Because of the different conditions under which girls and boys learn their identifications, girls have fewer problems in learning their samesex identifications and succeed more completely with less probability of an opposite-sex identification. Because of the more favorable conditions under which girls learn to be women, they are less anxious about gender-role identity than males are. Since girls are less often punished for boyish behavior than boys are for girlish behavior, they develop less hostility for males and male activity than males do for females and female activity.
Since the acquisition of feminine role behavior is learned under less stringent contingencies of punishment and reinforcement, girls are less rigidly identified with their role. When boys do surmount their difficulties and become firmly identified with the masculine role, they enjoy the status of being the dominant sex and the perquisites that attach to the status of maleness. Thus, males develop identity disturbances at a slower rate as they get older. Girls, on the other hand, grow up to discover the prejudices prevailing against them on all sides, learn that they occupy an inferior status, and become disenchanted. As we saw already, more of them than males show a preference for the role of the other. They may state this preference quite openly, as it is perfectly rational to feel envious of others whom one perceives as greatly favored in contrast to one’s own oppressed condition. But preference is not identification; girls may prefer the male role but maintain a feminine identification. Finally, because of the greater latitude for females in these matters, more of them will adopt aspects of the culturally defined male role than will males of the female role. As an example, the proportion of girls who plan to have careers is expected to be greater than the proportion of boys who prefer domesticity. Although, parenthetically, if the housewife’s job were accorded wages and high status, we might see an increasing number of males taking an interest in it.
Parental Identification in Adolescent Girls
Parental identification, the internalization of attitudes, interests, and values of a parent, interacts with gender-role identification in complex ways. Children may identify with their same-sex parent, with their opposite-sex parent, with both parents, or with neither. A parent may not be unequivocally feminine or masculine in her or his own gender-role identification, but may manifest attributes of each. A child may identify with some aspects of one parent and some of the other or may shift her identification as she moves into a different stage of her life cycle. Prediction of gender-role identification from parental identification, or vice versa, would depend upon an assessment of the interactions among the following elements: the strength of the identification with either or both parents, the extent to which the parents themselves are identified with typical gender roles, and parental reinforcement and modeling of gender-role identification. For example, a girl may develop a strong identification with a mother who is not very feminine; thus the girl’s gender-role identification would not be feminine. She might identify with a feminine mother and be rewarded for typically feminine behavior by both parents, in which case one would expect an unequivocal feminine gender-role identification.
Freud’s prototype theory of identification saw the girl resolving her Oedipal conflict by incorporating the mother, thus reducing her fear of losing the mother’s love. For daughers, identification with the mother and with the female role was the normal course, and girls who deviated from it by identifying with the father, or with the masculine role, had adopted a neurotic solution which was incompatible with a healthy personality adjustment. As we saw in Chapter 2, this formulation does not lend itself gracefully to empirical testing of all its components. Even so, its effect continues to be seen in the assumption that a girl identifying with a feminine mother has the best chance for a healthy adjustment. Paradoxically, empirical studies have failed to find a positive relationship between maternal identification and personality adjustment in girls, though father identification has been related consistently to good adjustment in boys. In fact, several studies have found that when parents present sex-typical models for their daughters, those who identify with a masculine father have a better level of personal adjustment than do those who identify with a feminine mother (Heilbrun, 1968a). Another study of sex-role identification and level of personality functioning in late adolescent girls went as follows. Behaviors were categorized into four parental models: ascendant-dominant mother, ascendant-dominant father, retiring-passive mother, and retiring-passive father. The extent to which the girl attributed the behaviors to each parent and to herself identified the model and measured the strength of her identification with it. Composite profiles for the four identification groups revealed that girls identifying with ascendant-dominant fathers had the highest level of functioning, while those identifying with retiringpassive mothers had the lowest (Williams, 1973). This, of course, is diametrically opposite to a prediction based on Freudian theory.
Other attempts have been made to explain such anomalous findings by using the constructs of expressive and instrumental orientations, seen as the essence of feminine and masculine sex roles. The expressive person is sensitive to relationships, attitudes, and feelings, and rewards others by being solicitous, warm, and understanding. The instrumental person is goal-oriented seeing relationships as means of attaining ends. Being less sensitive to the immediate emotional responses of others, he learns to tolerate the hostility which his instrumental approach sometimes elicits. It should be obvious that these styles can coexist to varying degrees in individual behavior repertoires and that a mature and healthy personality would combine both, would be both sensitive and competent, though perhaps more one than the other. Thus, a masculine father though primarily instrumental could also behave in expressive, nurturant ways, especially toward his daughter. He could model for her both instrumental and expressive behavior, thus facilitating healthy personality functioning (Heilbrun, 1968a). Presumably, if sons were exposed to a father who was both instrumental and nurturant in approach, they might develop a healthy personality as well.
In a study of the strength of expressive and instrumental tendencies in masculine and feminine girls, groups of college undergraduates worked together on a project. After three hours, they rated each other on dimensions of expressive and instrumental behavior. Their sex-types were determined by a conventional masculinityfemininity scale and were compared to their expressive-instrumental ratings. Interestingly, both masculine and feminine girls were equally expressive, but the masculine girls were also instrumental, whereas the feminine girls were not. Further, when parental identifications were examined, 62 percent of the masculine girls were masculinefather identifiers, and 64 percent of the feminine girls were feminine-mother identifiers (Heilbrun, 1968b).
Such intriguing findings support the idea that fathers can model both instrumental and expressive behaviors for their daughters, and that daughters who identify with such fathers and who adopt both kinds of styles will have more effective personalities than will those who, by identifying with feminine mothers, develop their expressive behaviors only.
Basically the sex of the parent model is not important. If the personality of the healthy person includes an integrated balance of both expressive and instrumental styles, then she or he could surely learn these competencies from a variety of people, unspecified as to sex. More men than women are likely to be instrumental because of the different role requirements in our society. More women are likely to be expressive for the same reason. Girls can learn the instrumental attitude from mothers, but they are less likely to do so.
The Daughter-Parent Relationship
The sex of the unborn and the newborn infant is a matter of great importance to parents. Much speculation is evoked by interest in the sex of the infant in utero, giving rise to all kinds of predictive attempts based on signs of one sort or another. If the baby is carried high, it’s a boy; if the mother suffers more from nausea this time than last, the sex of the baby will be different. But underlying all of this is a preference on the part of both men and women for sons over daughters, especially for their first-borns. Men generally feel stronger about this than women do. Even the influence of feminist thinking has not greatly altered women’s wishes for sons (Williamson, 1976). The preference for sons seems to be widespread and deeply rooted in culture. It is probably generated from beliefs in the superiority of males and from the desirability of having the firstborn be one who through strength, dominance, and age could serve as leader and protector of younger siblings, and even as “man of the house” should his father die. But despite all of this, researchers are now paying much more attention to daughters: their development, their education, and their relationships with their parents, especially with their mothers, (e.g., Friday, [1977]; Lynn. 1979).
The mother-daughter relationship
The bond between a mother and a daughter or a son begins at birth. During early infancy, a strong attachment develops, one that is necessary for social development. But at one point in the developmental process, it becomes clear that the son is supposed to break away; the daughter, to remain by her mother. In the words of nineteenth-century poet Dinah Craik, “Oh, my son’s my son till he gets him a wife / But my daughter’s my daughter all her life.”
Erica Jong in Fear of Flying (1973) wrote of the intensity that can define the mother-daughter bond:
A little gold chain chained my mother to her mother, and me to my mother. All our unhappiness was strung along the same (rapidly tarnishing) gold chain (p.44).
My love for her and my hate for her are so bafflingly intertwined that I can hardly see her. I never know who is who. She is me and I am she and we are all together (p. 161).
The life cycle of the mother-daughter relationship has been described as including stages of symbiosis, separation, and individuation (Magrab, 1979). The female infant may be seen by the mother as an extension of herself. A daughter may evoke a strong narcissistic need on the part of the mother to move vicariously into the life of her daughter. For the infant, the mother is the first love object and the most important attachment she will ever make. Yet the mutuality of the relationship with its intense needs flowing in both directions must give way to separateness as the daughter struggles to make her own identity and to establish herself as her own person. Though this process draws from a wider world than home—as she encounters peers, goes to school, and so on—for some the separation is delayed or resisted, giving presence to “latency girls,” (Rheingold, 1964). These are daughters who cannot liberate themselves from their mothers and so are hampered from confronting such adolescent issues as independence and developing sexuality.
As daughters grow into adolescence, even good relationships with their mothers can become stressful, filled with strife and rebellion. Values around morals and sexuality are often different across generations, and give rise to conflict. Daughters struggle for autonomy, trying to free themselves from the old bonds of childhood. Sometimes mothers overidentify with their daughters, feeling rivalrous and jealous of their youthful beauty. These mothers continue to try to live vicariously their daughters’ experiences. Such violations of boundaries between generations make it difficult for daughters to define themselves. Daughters develop strong needs for privacy. They often make others their confidante, a close friend, a friend’s mother, a special teacher. Some mothers find this separation painful, not understanding their daughters’ need to establish a separate space for themselves.
Often despite a daughter’s rebellion against her mother, she will still consider her mother as the person to whom she feels closest. Commenting on her mother, one daughter remarked,
She’s given me confidence in myself and sometimes she tries to make me understand her point of view.... I kind of listen to her even though I pretend I’m not listening, I turn my face, and she makes me believe in myself, even when I’m down (Konopka, 1976, p. 65).
Individuation is the last stage in the mother-daughter relationship. It occurs when the daughter matures, that is when she experiences some of life’s milestones, which may include marriage, motherhood, career, making a life of her own and so on. For some, these events may raise old issues of rivalry and competition. For many, they may bring mother and daughter closer as daughter assumes adult roles and has more in common with her mother’s life. This closeness is not the old symbiosis, however; it is, rather, an intimacy that comes from sharing, and from knowing each other well.
The father-daughter relationship
Although the research on fathers and daughters is sparse indeed, what we have reveals some striking differences between fathers and mothers as they relate to growing daughters. The greatest, of course, is in the amount of time that each spends with the child.
Mothers, even those who work away from home, spend many hours per day with infants and young children. Estimates of fathers’ time with babies vary from about twenty minutes to an hour a day. And generally, fathers spend more time with male infants than with females. This becomes more dramatic during a daughter’s second year of life. At this point, fathers exhibit a “withdrawal” from their daughters, and spend only half as much time with them as with their sons (Lamb and Lamb, 1976). Fathers also reward daughters for good behavior about half as often as they do sons, though mothers are the disciplinarians for most daughters (Margolin and Patterson, 1975; Sears et al., 1976).
Numerous studies have found that fathers tend to be more stereotypic in their thinking about their offspring than mothers are. Fathers are more attentive to their children’s sex category and perceive and treat them accordingly, while mothers are more likely to treat them simply as children. Some have thought that this differential treatment reinforces traditional femininity in girls and masculinity in boys. Fathers’ tendency to stereotype daughters in traditional ways may occur simply because fathers do not know their daughters very well and thus fall back on their own old learnings. Some evidence for this appeared when fathers were asked what they thought their adolescents’ problems were. Fathers of sons were fairly accurate, but the accuracy of fathers of daughters was no greater than that obtained when the ratings of parents were randomly matched with unrelated adolescents. Mothers were more accurate than fathers were, especially for daughters (Wakefield, 1970).
Many adolescent girls described their relationships with their fathers as different from those with their mothers (Konopka, 1976). Only about a quarter of them felt close to their fathers; often fathers were almost invisible in their lives. Over and over the girls said that their fathers did not want to let them grow up, wanted to keep them “daddy’s little girl.”
The relationship described by the girls varied from highly positive to highly negative. Girls who were close to their fathers saw them as wise counselors or as protectors. One girl said: “He’s an all right guy ... he’ll sit down and have long talks with me about trouble at school ... he wants to know like just what we’ll be doing, what’s going on, where we’ll be going. He worries about us (p. 68).” For some, the father is considered “invisible.” “I’m not that close to him. I just know him as the father and that’s it (p. 69).” Fathers who were seen as authoritarian, overly suspicious, or abusive elicited the most negative comments: “It’s a feeling of not really hate, but close to it. My dad is one of telling, “Do this, do that.” And that’s where my hang-up is (p. 68).”
Although fathers may be aloof and distant figures for many girls, their influence on development is significant. Fathers can model instrumental behavior for girls and encourage them toward achievement in nontraditional as well as traditional fields. These effects are stronger if daughters identify with their fathers and feel love and respect for them. Fathers can also encourage more traditional feminine behavior in girls, by their treatment both of their daughters and their wives. But in many cases, the fathers’ withdrawal from the lives of their daughters establishes mothers as key role models. Because of the fathers’ relative inaccessibility, daughters may seek to win approval from their father for feminine behavior, thus making fathers potent reinforcers of stereotypic gender-related behavior.
Other studies show that in families in which marital roles are clearly differentiated, with the father dominant over the mother, daughters are more likely to assume traditionally feminine roles and attitudes. If the adoption of traditional gender roles is seen as less adaptive in today’s society, then father-dominance could have unfortunate consequences for daughters: it could strain the father-daughter relationship by introducing distance between them; it could contribute to less favorable psychological adjustment, as with the retiringpassive daughters in the Williams (1973) study; and it could promote acceptance of the traditional feminine role (Lynn, 1979).
Sex Typing and Socialization Experiences
All societies differentiate between the sexes through the assignment of different roles. They also promote different standards for females and males in various areas of behavior and personality. In our society, females are supposed to be unaggressive physically and sexually, nurturant and caring toward others, expressive and friendly, and attentive to their appearance. Males are expected to be physically and sexually assertive, independent, competent, and emotionally tough. The behavior thought to be appropriate for females is facilitative of interpersonal relations, while that expected of males is facilitative of solving problems. Such expectations make up gender-role standards and are inculcated in children in the socialization process.
What this means is that the society through its institutions encourages the development .of different behavior patterns for boys and girls owing to beliefs about the desirability of certain attributes in boys and others in girls. Thus the socialization process by which the child is trained both formally and informally to fit the requirements of the society differs in some ways for girls and boys. Society arranges for them to have different sets of experiences in preparation for the roles they will take up as adult members of the society.
There is a difference between sex typing and sex stereotyping. Sex typing is the prescription of different qualities, activities, and behaviors to females and males in the interest of socializing them for adult roles. Sex stereotyping is the promotion or expression of commonly held beliefs about gender differences or roles, sometimes to the point of caricature. Thus, a real girl is preoccupied with her looks, unambitious, loves animals (but is afraid of mice), and cries a lot. A real boy is fearless, noisy, insensitive, interested in sports and science, and resistant to bathing. Sex typing gives rise to stereotyping, the forming of loose generalizations about categories of people, failing to make discriminations among their infinite varieties.
Gender-role stereotyping begins early in life. An extensive study of twenty-six-, thirty-one-, and thirty-six-month-old children examined their ability to categorize by sex pictures of males and females and to identify their own sex category. Their preference for sex-typed toys and their awareness of adult gender role differences were also observed. A majority of the twenty-six-month-olds could verbally label the sex of male and female pictures, while a majority of the thirty-one-month-olds could verbally state their own sex as well as identify themselves with persons of their same sex. Preference for sex-typed toys (dolls for girls, trucks for boys) was related to knowledge of gender identity; and a majority of the thirty-six-month-old children could identify adult clothes, tasks, and possessions by sex category (Weinraub et al., 1984).
Parental influences
Do gender-role standards influence the child-rearing practices of parents? Is there a “double standard” for bringing up children that is promoted by the parents’ perceptions of the child’s sexual category and their beliefs about sex differences? That parents attribute different qualities to girls and boys from birth was documented in a study of parents’ perceptions of their newborn infants. Although male and female infants did not differ in weight, length, or Apgar scores,[19] daughters were significantly more likely than sons to be described as little, beautiful, delicate, weak, and as resembling their mothers. Boys were seen as firmer, more alert, stronger, and better coordinated. Father were much more extreme in their sextyping than mothers, who tended to rate boys and girls closer together with respect to these qualities (Rubin et al., 1974). Such labeling can be expected to influence expectations about future behavior of the child and also to guide the parents’ behavior as they begin to interact with the child in the home.
Support for the early influence of parents was found also in the Weinraub et al. (1984) study of the onset of gender-role stereotyping described above. Among these children in the third year of life, those whose fathers had more conservative ideas about women, who did less “woman’s work” around the house, and whose mothers worked fewer hours away from home had higher gender-labeling scores; that is, those children from homes where gender roles were more traditional had more differentiated concepts of what was appropriate for males and females. Likewise, fathers who engaged in more “feminine” role activities and mothers who worked more hours outside the home had children who were less aware of stereotypic genderrole differences.
A related study asked parents of six-year-olds how they believed the sexes to differ in behavior, and how they thought they ought to behave (Lambert et al., 1971). Rating boys and girls on such items as “more helpful around the house,” “more likely to be rough and boisterous at play,” and “more likely to act scared,” the parents described boys as rougher, noisier, more active, more competitive, and more likely to do dangerous things. Girls were more helpful, neater and cleaner, quieter and more reserved, more sensitive, and more easily upset and frightened. However, when asked which qualities they thought it important for children to have, they differed very little in their values for girls and boys. Both should be neat and clean, helpful in the house, able to take care of themselves, and thoughtful and considerate of others. Thus their socialization goals were much alike for both sexes, but they believed that they were starting from different points with different “material” to work with.
A recent review of the literature on differential socialization of girls and boys found surprisingly few differences in the ways that parents treat their children, in spite of widely held assumption to the contrary (Maccoby and Jacklin, 1974). However, there are some areas where differential effects are found. Parents provide sex-typed clothes and toys for children, and they discourage them, especially sons, from engaging in activities which they believe to be appropriate only for the other sex. Parental anxiety is elicited much more readily by a boy who wants to wear makeup and dresses than by a girl who wants to wear pants and play baseball.
Some surprises appear in the research. It is generally believed that one reason for boys’ greater aggressiveness is that they are encouraged or rewarded for it while girls are not. The fact is that parents do not value aggression in either sex, and a major thrust of their socialization efforts is directed toward teaching children to inhibit aggressive responses. There is no evidence in the research that parents reinforce boys and not girls for aggressive behavior, or that they are more permissive of it in boys. Another area of childrearing, the encouragement of independence and autonomy, is also usually thought to distinguish parents of boys from parents of girls. But in the preschool years parents behave similarly in their reactions to independence seeking (or its opposite, dependency behavior) in girls and boys, with mothers showing some tendency to be more restrictive toward boys. However, as girls begin school, parents become more protective of them, and are more likely, for example, to walk home with them. Beginning around age seven, daughters begin to receive what is called “chaperonage,” with adults checking on their whereabouts and accompanying them more than they tended to do with boys (Newson and Newson, 1968). But they are allowed to make their own decisions about where they want to go and what they want to do as often as boys are. The chaperoning seems to be less a fostering of dependency than an expression of concern about the danger that the child will be sexually molested, a risk to which very few parents of daughters are indifferent.
One area where parental behavior was different for the two sexes was in the administration of discipline. Boys were clearly found to receive more physical punishment than girls (Maccoby and Jacklin, 1974). One study provided an interesting explanation. The sequence of maternal acts leading up to punishment of the child was analyzed, and it was found that mothers tend to escalate their pressure on the child if their first request for compliance with a request is not obeyed. The mother then raises her voice, or removes the child if it is a dangerous situation, or spanks. Girls were more likely than boys to obey the first request, thus avoiding more spankings (Minton et al., 1971). Also, it is likely that boys simply do more things that draw parental wrath. If boys are more aggressive, and parents are working to teach the child other ways to settle problems, then boys would come in for a greater share of parental punitiveness. In addition, parents do see boys as tougher and girls as more fragile, and thus might be less likely to restrain themselves when they feel the child needs to be punished.
Few studies bear on the ways that fathers treat children, or on differences in fathers’ and mothers’ treatment of boys and girls. But those that do so reveal some interesting cross-sex effects. In general, parents seem to be more permissive with children of the other sex, and more strict with children of their own sex. In the area of aggression, mothers tend to be more tolerant of angry behavior directed toward them by sons than by daughters; fathers react in the reverse (Rothbart and Maccoby, 1966). Fathers were much more repressive toward expression of anger by sons (Block, 1973). Fathers were also more likely to take their daughter’s part in an argument with a guest, but if a son argued with a guest, fathers would take the guest’s side (Lambert et al., 1971).
Why should parents be more strict with children of their own sex and more lenient with children of the other sex? The father-son interaction may be a recapitulation of male dominance struggles. That is, the father is reacting to the son as a male who is challenging him, whereas a daughter is no such threat. The daughter, in fact, would benefit in this case from the probability that her father was socialized to be gentle with girls. As for mothers’ greater tolerance for their sons, women are accustomed to use moderation in their reactions to male threat, and perhaps this conditioning comes into play when they are confronted with boys’ flouting of their authority. A challenge from another female could be more openly dealt with (Maccoby and Jacklin, 1974).
Interestingly, the patterns of childhood socialization into gender roles observed in Western societies are not peculiar to us in either type or intensity. A study of the extent of sex-typing in the childtraining process of twenty-nine African and seventy-nine non-African societies revealed that highly differentiated patterns are common in Africa, and that these patterns are similar to those from other cultural regions. Specifically, they found that societal pressures for achievement, independence, and self-reliance behaviors are higher for male children, while female children experience more pressure for nurturance and obedience. Significantly, however, girls received less socialization pressure than boys do for sex-related behavior. These pressures are reflected in actual behavior, too, with boys showing more achievement, .independence, and self-reliance behaviors, and girls being more nurturant, obedient, and responsible. Boys had significantly higher scores than girls did for anxiety around socialization pressures in sex-related areas. The authors conclude that the stratification of child-training processes by sex is a universal phenomenon that takes similar form across a variety of societies (Welch and Page, 1981).
In general, where parents are concerned, it seems that boys receive more socialization pressure than girls do. Their behavior is subject to more and stricter sanctions. While there may be fewer differences in our society in the ways that parents treat sons and daughters than was once thought, where differences do occur, with boys they are in the direction of greater coerciveness and less tolerance for violations of gender-roie prescriptions. Apparently, it is more important for a boy to be all boy than for a girl to be all girl.
Other influences
As children grow, other sources of influence beyond home and family converge to strengthen sex-typing of the socialization process. Television, books, and school provide models for them, instructing them in how they ought to be and behave, informing them in countless ways, often indirectly, of the values of the society and of its expectations of them as females and males.
Children spend many hours each week looking at television, mostly for entertainment. At the same time, however, they are absorbing messages about the nature of people and of their world. Children in homes as far apart as Florida and Alaska watch the same shows, resulting in a level of uniformity in the informal learning that is part of the television experience. How does television depict gender roles? A few shows feature women as police officers or business executives. Many perpetuate stereotypes. An analysis of commercials in the morning, afternoon, and evening found that 60 percent showed women in three roles: maternal, housekeeping, and aesthetic (beautification or hygiene). Housekeeping commercials in particular made use of the male voice-over, in which an unseen male tells the woman about the product or how to use it. Men also appear in person as technological experts on the product. The housekeeper is pictured as being alone and needing male instruction if she is to use the product. One commercial had a woman saying, “I don’t know why it works, it just does” (Mamay and Simpson, 1981).
Children appeared in the commercials primarily to be fed or doctored, get their clothes muddy, or mess up the house. Mothers gave them things to consume and expected nothing in return, a oneway obligation. Thus woman’s status in the commercials is lowered in two ways: (1) Housekeeping is a complex technological process in which men are the experts, and (2) mothering consists of serving children who are self-centered consumers who do not work. The family is not a social unit, but a loose-knit collection of people living in the same house, cared for by the mother. The authors point out that gender-role differentiation is greater in the commercials than it is in the real world—but what do children learn?
A study of prize-winning children’s picture books concluded that the females were dull and stereotyped, neat and passive, their status determined primarily by their relationship to males—wife of a king, admirer of an explorer, helper of a worker. Working women and divorced women did not exist. “The world of picture books never tells little girls that as women they might find fulfillment outside of their homes or through intellectual pursuits. Women in the books are excluded from the world of sports, politics, and science. Their future occupational world is presented as consisting primarily of glamour and service” (Weitzman et al., 1972, p. 1146).[20]
A popular line of children’s books sold by the millions in supermarkets and drug stores includes a story of a small boy and girl fantasizing about the future (Vogel, 1968):
-
He will be a baker, an icing expert. She will be the baker’s wife.
-
He will be a mailman, delivering surprise packages. She looks, listens, says nothing.
-
He will be an explorer in the jungle, and will bring back a lion. She will curl the lion’s mane in her beauty shop for animals.
-
He will be a policeman. She will wear a disguise and be his helper.
-
He will be a doctor. She will be a nurse.
-
He will be a fireman. She will be rescued by him.
-
He will be a deep-sea diver. She will be a mermaid and serve him tea and ice cream.
-
He will be an artist. She will be a singer. As he paints, three of the four people watching him are females. As she sings, all her admirers are birds.
-
He will be an astronaut and go to the moon. She will be there, prepared to serve him moonburgers.
All nine of his fantasies have the potential to be realized. They are real occupations for which people are trained and paid. Of hers, only three seem to have even the slightest vocational potential: nurse, singer, and animal groomer. In the others, she marries him, helps him, and serves his food. And she is a victim if the house catches on fire.
When boys and girls start school, they do not need to make any adjustments in their previously acquired perceptions of sex roles. A ten-year study of 554 stories in readers for elementary school revealed that men and boys continued to outnumber females in the new editions, and role stereotypes were if anything stronger. While more occupations for women appeared in the newer editions, they were still far from reflecting reality, especially where women were concerned (Graebner, 1972). An extensive study of nearly three thousand stories in over one hundred readers for grades one through six found the following sex ratios:
| Boy-centered stories to girl-centered stories | 5:2 |
| Adult male main characters to adult female main characters | 3:1 |
| Male biographies to female biographies | 6:1 |
| Male animal to female animal stories | 2:1 |
| Male folk or fantasy stories to female folk or fantasy stories | 4:1 |
These readers do much more than teach reading. Those traits valued as positive and desirable in our society are displayed by the protagonists most of whom are male. Boys are clever, brave, creative, and resourceful; girls are docile, kind, dependent, and selfabnegating. Fathers solve problems, and take the children (boys) hunting and fishing. Mothers are the perfect servants, disgruntled sometimes but always on call. “The reader mother is a limited, colorless, mindless creature. She wants nothing for herself you have to assume, since her needs are mentioned only once in this entire study when she treats herself to some earrings on a shopping trip” (Women on Words and Images, 1972, p. 26).
One report of major fields by sex at a large state university in the Southeast provided some interesting data on the later effects of gender-typing of roles and of socialization practices relevant to career choice. Majors with high female enrollment included foreign languages, education, fine arts, rehabilitation, communicology, gerontology, and nursing. Majors with high female enrollment included foreign languages, education, fine arts, rehabilitation, communicology, gerontology, and nursing. Majors with low female enrollment were in the colleges of engineering and medicine.{3}
Thus the majors with the highest female enrollment are those that imply roles of expressiveness, verbal skills, and nurturance of the young and the sick. However, the high proportion of females in these areas reflects not only their appeal for women but also their lack of appeal for men. Such observations of young adults of both sexes show clearly the results of differential treatment and expectations applied earlier in the life span.
Computer education is a good example of differential coursetaking by male and female students. In 1984, fifty high schools in Florida sent student teams to a statewide computer programming contest. Of the two hundred competitors, five were girls. According to a report on the “gender gap” in computer education, girls and boys in elementary school are similar in their interest in computers. The change begins in middle school. In one Florida middle school, twelve boys and nine girls took the first year of a two-year programming course. Seven boys and no girls completed the second year.
In high school, the gap widens. One girl, a computer student, said that the girls lack confidence in their ability to do things with the computer. “If a boy and a girl both learn how to load a floppy disk, the girl will say ‘All I can do is load a disk,’ while the boy will say, ‘Hey, I can load a disk.’ ”
In one high school, boys outnumbered girls two to one in computer programming classes. But girls outnumbered boys more than seven to one in word processing classes, learning to use computers as sophisticated typewriters.
There are few role models for women computer students at the university level. One large state university in Florida had no women on its computer science faculty of fifty-four professors (Gibson, 1985).
While it is easy to document institutional pressures for sextyping of activities, interests, and roles, and the stereotypes that arise therefrom, their persistence and implications need to be considered also. Schools as institutions of society tend to support the status quo, and despite the idealism of their goals, they do not necessarily initiate innovations that will lead to social change. Schools in general are conservatories of the past, and they change in the wake of social change—they do not initiate it.
The authority structure of the school itself is a model for the larger society. The large majority of elementary teachers are female, but most principals are male. When children misbehave they are sent to the principal, the ultimate authority figure.
Children spend a very large amount of their time in the classroom interacting with each other and with their teachers. The teacher is the representative of the adult society. Does she behave differently toward boys and girls, and if so, what does this mean for the subsequent development of the child? A review of the few studies in this area supports an affirmative response to the first question. Boys were the recipients of more blame for disobedience than girls, but they also received more positive attention. Girls exceeded boys on disapproval for lack of knowledge. When teachers were asked to describe incidents in which they had rewarded creative behavior, of those mentioning sex, 74 percent involved boys, and 26 percent girls (Sears and Feldman, 1974).
Different experiences should have different effects. Boys have more difficulty adjusting to the requirements of the school situation for disciplined, conforming behavior, thus making greater demands on the teacher’s attention. But attention, both positive and negative, can have reinforcing effects, can confirm feelings of importance, and encourage a certain resistiveness to authority that goes with motives for autonomy and independence. For girls, criticism for lack of knowledge (even though they make better grades) could have a negative effect upon self-esteem and undermine confidence in their ability and worth. Further, the “feminine” behaviors rewarded by teachers and schools seem to be just what girls do not need for future achievement. In addition, studies show that nonconformity with that role is associated with higher IQ, and that the girl whose IQ increases from ages six to ten is likely to be competitive, independent, and dominant (Baumrind, 1972).
It is unfortunate that personality qualities such as autonomy, assertiveness, competitiveness, and initiative have been consistently called masculine in the literature, while others such as conforming, dependent, passive, nurturant, and sensitive have been labeled feminine. It may be that more males are described by the former, and more females by the latter, so that it became expedient to use such terms, subsuming a whole array of characteristics under the words masculine and feminine. But such usage is not only sexist,[21] reinforcing the relationship between socially valued characteristics and males, it also encourages the notion that if girls are going to fulfill their potential, they must become more masculine. The emotional and value loading of the word masculine when applied to females may itself mediate resistance to permitting or encouraging the display of these traits in girls. Since sex itself is not a personality characteristic, should we not recast our formulations to consider what traits in what strengths combine in individuals to effect a wide range of healthy personalities distinguished by many diversities not necessarily linked to sex?
The Menarche: Socialization Effects
“... beginning to menstruate makes you think about things.”
—Marjorie Shostak, Nisa, 1981
In Chapter 4 we looked at the physiology of the menstrual cycle, including its onset, the menarche. Here, we want to examine the menarche as a socializing event, to consider its meaning in the lives of adolescent girls.
In societies with strong menstrual taboos, the menarche is a rite de passage, celebrated by a variety of rituals and special treatment of the young girl (for a complete account of these see Weideger, 1977). In our society, the taboos on menstruation are more subtle, consisting of special names for the flow, prohibition of certain activities, and the need for secrecy, and there are no formal menarcheal rituals to mark the passage of the young woman from childhood to womanhood.
Early psychoanalysts generally attached highly negative meanings and interpretations to the menarche, defining it in terms of physical violation, damage, and psychic trauma. The menarcheal girl experienced shame, believing that “divine punishment has fallen upon her as retribution for former misdeeds” (Chadwick, 1932, p. 33). The bleeding “wound” evoked from the shadows of the unconscious the old Oedipal afflictions of penis envy and castration anxiety, and her female masochistic potential was confirmed forever. That menstruation was a curse upon womankind was taken for granted; psychoanalyst Otto Fenichel (1945) called the menarche “the first pollution” (p. 11).
Helene Deutsch (1944) in an often insightful essay on menstruation emphasized its problematic features, including the traumatic effects of the menarche, brought out in her analytic work with her patients. She dwelt on the shame experienced by the young girl, whose greatest horror was the fear of detection, that someone would “know” of her unclean state:
This view of menstruation as unclean is a direct descendant of the cloaca theory, according to which everything coming from the lower apertures of the body is dirty and distasteful. The idea of dirtiness can in fantasy be extended to the entire body and the girl feels unclean and depreciated as a whole. Her relation to herself now corresponds to ... those taboos and superstitions in which a girl who is menstruating for the Erst time is treated as unclean in the highest degree (p. 162).
Clara Thompson too, whose work was reviewed in Chapter 3, was critical of the way society defined menarche. She wrote of the resentment of one of her young patients who, after she started menstruating, was no longer allowed to go camping or hiking with her brother. “She was filled with bitterness and envy of her brother and for several reasons centered her whole resentment on the fact of menstruation. This seemed to be the sign of her disgrace, the sign that she had no right to be a person” (1964, pp. 234—35).
What is the experience of girls today? Certainly information is more generally available, some mothers and teachers are better informed, and the weight of the old sanctions against “talking about it” is less. Still, elements of the taboo continue, and it is a rare girl who approaches menarche completely informed and experiences it with equanimity (Breit and Ferrandino, 1979).
Though girls who have absolutely no preparation for menstruation are in the minority, even those who know what is happening often experience fear at the first occurrence (Konopka, 1976). Mothers are usually the ones who impart the information, perhaps minimally, or in an embarrassed and awkward way. Many mothers themselves know little about it and were raised to consider it shameful and dirty. Too, the menarche is highly significant in mothers’ minds as a symbol of their daughters’ developing sexuality and the possibility of pregnancy. Sometimes information is accompanied with dire warnings to “stay away from boys,” with no explanation or with the suggestion that boys plus menstruation equal pregnancy. A seventeen-year-old girl remembering her menarche related:
My mother told me not to let a boy touch me or I would have a baby. And I always thought if a boy touched my hand I was pregnant.... One day a boy bumped against me. I was scared. I went home and laid in bed and I said, “Oh Lord, I’m pregnant” (Ladner, 1972, p. 179).
Another adolescent girl reported:
I just know when I went to the bathroom and I talked to a girlfriend. She told me that 1 was, you know, having a period, and I was so happy. 1 was waiting for it. My mother had already bought me all these things. I don’t know, just felt like I was growing up, you know (Konopka, 1976, p. 49).
A contrasting experience was related by a fourteen-year-old girl:
It was horrible. My twin sister had started about a month earlier and she told me about it, and I said, “Oh no, I’m just gonna die.” I had never heard about it before, and she had never heard about it before she started (Konopka, 1976, p. 47).
More positive attitudes toward menstruation were expressed in a later study of premenarcheal nine- to twelve-year-old girls. Most identified it with growing up and being normal. Even so, about a third thought it would be embarrassing, and others felt it would be disgusting or a nuisance. Many also believed some of the old taboos, such as that a girl should not go swimming or be active in sports while menstruating. Most drew the line at talking about menstruation with boys, and 40 percent did not approve of such discussion with their fathers (Williams, 1983).
So-called sex education classes and books and pamphlets intended to inform girls (and boys) about their bodies are often less than honest, perpetuating the taboo in their own way, as, for example, by using cartoon illustrations, or drawings of girls’ bodies in which there are no labia, cervix, clitoris, or hymen (Delaney et al., 1976).
A few exceptions, however, suggest a change in the direction of greater openness and more explicit dealing with the subject. One is Judy Blume’s book for young girls, Are You There God? It’s Me, Margaret (1970). The story of Margaret and her friends, all of whom are awaiting their periods presents a positive view of puberty and its physical changes. The girls are eager for their breasts to grow, and they are in friendly competition for their periods to start. Mothers are friendly and understanding. With an all-female cast, the book is a little vignette for girls, one which echoes a female culture heretofore absent in juvenile literature (Delaney et al., 1976). A second is The New Our Bodies, Our Selves, written by the Boston Women’s Health Collective (1984). For an older audience, the book is clear and explicit, and deals in very direct language with the menstrual process and the many questions that even experienced women may have.
Other changes
The significance of menarche as a critical event is manifested in important areas of a girl’s life, such as relationships with parents and her own body image.
One study compared pre- and post-menarcheal girls in the sixth and seventh grades. Though the average ages of the two groups were the same, the postmenarcheal girls were more likely to shave their legs, wear makeup, and go out on dates. They also were less comfortable discussing emotionally charged subjects such as sex and drugs with their parents and had more conflict with their parents than the premenarcheal girls did (Danza, 1983).
After menarche, girls experience personal changes in the ways they perceive their own bodies as well as the bodies of others. In one interesting study, seventh grade girls drew male and female figures on two occasions about six months apart. Of the eighty-seven girls in the study, thirty-four were premenarcheal on both occasions, twenty-three were postmenarcheal on both occasions, and the menarcheal status of thirty changed between the two occasions of testing. As a group, the postmenarcheal girls produced drawings that were more sexually differentiated, and they were more likely to draw their own sex first. Among those girls whose menarcheal status changed from the first to the second testing, there was likewise a change in the direction of greater sexual differentiation in the second drawings. Such changes were not apparent in the drawings of girls whose status remained unchanged in the course of the study.
(Reprinted by permission of the publisher, from Menarche, edited by Sharon Golub, Lexington, Mass.: Lexington Books, D.C. Heath and Company, Copyright 1983, D.C. Heath and Company.)
Dramatic evidence of the effect of menarche on body image can be seen in some examples. The drawings in figures 6.1a and 6.1b were made by a premenarcheal girl whose status did not change during the study. Those in figure 6.2a and 6.2b were by a girl who was postmenarcheal at the onset of the study; and those in figures 6.3a and 6.3b were done by a girl whose menarcheal status changed between the two testings. One can see rather striking changes among the postmenarcheal girls in the direction of greater sexual differentiation of the drawings, including more mature body contours, breast development, and more feminine hairstyles, dress, and adornment, as if the menarche itself had effected a transformation from girl to woman (Koff, 1983).
Achievement: Conflict and Resolution
The finding that women do not attain to the level of their intellectual and creative potential echoes with a dreary sameness through the literature on achievement. In 1913, Castle undertook a statistical study of the thousand most eminent women of history but found that in all of recorded time there were not many women who could be called eminent by any reasonable criteria (Castle, 1913). A classic longitudinal study of gifted children begun in 1921 showed that the girls were more gifted artistically, and the seven most talented writers were girls. But when these gifted children grew up, all the eminent artists and writers among them were men (Terman et al., 1947; 1959). As adults, almost half the men were professionals in high-level occupations. Only 11 percent of the women were in professions, mostly teaching. Many of the women had made their most notable achievement in their selection of a mate. Their husbands were the achievers.[22]
Many reasons have been advanced for this ubiquitous phenomenon. During the nineteenth century, spurred by the discoveries of Charles Darwin, many writers promoted the hypothesis of greater male variability in such attributes as intelligence and creativity (Shields, 1975). That is, more males are found at both the high and the low end of the ability spectrum. This doctrine explained both the finding that more men were in institutions for the mentally retarded and also the common observation that many more men were among the achievers, the eminent, and the creative. The hypothesis of greater male variability has not been seriously challenged as yet, though alternative explanations have gained more credence. The preponderance of males at the low end of the mental ability spectrum is well documented and is explicable on the basis of the greater male vulnerability to congenital defects and early brain trauma discussed in the last chapter. The difference at the upper end of the spectrum can be explained as a reflection of the differences between women’s and men’s lives—as a social artifact. Evidence of innate differences in variability in intelligence or creativity is lacking. The literature on sex differences in variability reveals that boys were more variable, that is, more scored very high and very low, on tests of spatial and numerical ability, but they were not more variable on measures of creativity (Maccoby and Jacklin, 1974). If as many girls as boys are creative in their youth, then the greater creativity of males in later life would have to be explained on grounds other than innate characteristics which would determine that men are more talented than women, or that more men than women are talented.
Genius is rare in any population. For its quality to become manifest, motivation, opportunity, training, and tools must be available. It seems reasonable to believe that such a combination has been more probable for males than for females in the history of civilization. For example, Anne, a seventeenth-century queen of England for whom life must have been more propitious than for the average woman at that time, had ten miscarriages and gave birth to five infants, only one of whom survived his first year, and he died at age eleven. One of her biographers tells us that “she took no interest in the art, the drama, or the literature of her day” (Yorke and Thomson, 1958). The twentieth-century British novelist Virginia Woolf, in A Room Of One’s Own, imagined that Shakespeare had an equally talented sister named Judith. What would her fate have been? She was “not sent to school. She had no chance of learning grammar and logic, let alone of reading Virgil and Horace. She picked up a book now and then, one of her brother’s perhaps, and read a few pages. But then her parents came in and told her to mend the stockings or mind the stew and not moon about with books and papers” (quoted in Rossi, 1973, p. 639). To escape an arranged marriage, Woolf thought, she would
have run away to London as did her brother; but there, she would have been laughed at for her ambitions, and denied training in her craft. “No girl could have walked to London and stood at a stage door and forced her way into the presence of actor-managers without doing herself a violence and suffering an anguish .. (p. 641).
Achievement and Socialization
Observations of differences in high-level achievement reveal effects not causes, and cannot really answer the questions posed by woman’s lesser productivity away from the home. “Very few women have ever had the opportunity to enter this world and fewer still have been admitted fully to it. For most of human history most women have spent most of their adult lives gestating, nursing, and caring for small children, these functions preempting their entire lives. They were ignored for all high-level purposes, shut out from the world that supplied the conditions of productivity. They are only now beginning to enter it and even yet there are many barriers” (Bernard, 1973).
This scenario of the fate of the capable woman has been documented in countless lives. During the 1970s, researchers became attentive not only to discrimination and lack of opportunity as deterrents to female achievement, but also to elements in the socialization process which give rise to a number of interlocking hypotheses. While boys identify with a culturally defined masculine role, which includes an achievement yardstick by which they will be evaluated, girls identify with their mothers, most of whom have not achieved independently outside the home. Girls are more dependent upon the reward value of interpersonal relationships, thus they work for love and approval rather than for the intrinsic value of the achievement itself. Girls and women are assigned the social roles of providing nurture and compassion to other members of society, and the domestic setting is a natural stage for the display of these qualities. The prevalent mores are such that males do not like to compete with females. This provides negative consequences for girls who dare, such as loss of popularity and denial to them of social perquisites reserved for conforming women. Great difficulties lie in the path of the young woman with potential who decides to use it to the fullest. Not only will she encounter the remnants of sex discrimination, but the combination of the demands of a family and the demands of a career on time and energy are impossible for many, entailing at best the loss of a few years in her career development while babies are young. Confined to home for those years, her confidence in her ability diminishes. If she decides later to make a commitment away from home, she may be plagued by guilt and anxiety, and so settle for a role which is less demanding.
It has been suggested that contrasts between the experiences of females and males are rapidly diminishing along with a depolarization of gender roles (Winick, 1969). But if work roles are becoming disengaged from sex, little effect was noted in a study in which the responses of fifth-graders revealed their views of career and employment patterns, and of home and family responsibilities to be highly traditional. When given a list of jobs and asked whether men, women, or both should perform them, a majority of both sexes thought that bosses, taxi drivers, mayors, factory workers, and lawyers should be men, and that nurses and house cleaners should be women. Asked to indicate who does what around the house, they held that women wash dishes, cook, dust, scrub floors, and get up at night with a sick child. The men’s list was shorter—they pay bills, fix things, and work in the yard. Career aspirations of the children also reflected traditional sex typing. The boys wanted to be engineers, professionals or sportsmen; the girls, teachers, nurses, and stewardesses. Only 6 percent said they would be a mother or housewife only. But when asked to describe how they would spend a typical day when they were grown up, most of the girls emphasized marriage and family life in their descriptions, while the boys overwhelmingly ignored it, focusing instead on details of job and career (Iglitzin, 1972). While it would be difficult to find evidence for a blurring of gender roles in these data, we may note that, while girls no more than boys took an innovative posture, more of them were willing to see jobs open to both sexes, could see both parents performing household tasks, and assigned similar personality traits to both sexes.
The task of answering the question What do I want to be? is probably less conflict-ridden for ten-year-old girls than for their older sisters who are closer to the time of choosing. The younger girl is still free to imagine the future in any way she likes. And if her statement of what she wants to be does not mesh with her vision of a typical day in her future as an adult, it is of no consequence. The contingencies and the payoffs of the choices she will make are still far from clear to her, and she can comfortably tolerate the ambiguities and contradictions in her fantasies.
Let us consider two revealing and touching examples. A ten-year-old girl in the above study said that she wanted to be an artist, or maybe a beautician. When asked to look into the future, and describe a typical day of her adult life, she wrote:
I would start the morning after getting out of bed by eating breakfast. Then I would clean house. If I was done before lunch I would probably visit a friend. Then eat lunch. After lunch I would go shopping. Then I would come home and rest for a while. When my husband came home (if I was married) he would probably tell me how his day went and I would tell him how mine went. If he was in a real good mood he would take me out to dinner. When we were done with dinner we would go to a movie. Then we would go home and go to bed (Iglitzin, 1972).
Where in this regimen is the painting of pictures or the dressing of hair? I suspect that the discontinuity lies in the available responses evoked by the questions. The question to a ten-year-old, What do you want to be, opens to her the whole spectrum of occupations observed by her thus far, and invites her to choose one. By this time she has a global idea from the media and from the various commentaries available to her of the activities associated with certain jobs, and she chooses on the basis of that knowledge. But when asked to visualize a typical day in her future, she falls back on her observations of what real women really do. What other data has she? We should not read into this a doom-saying prescience of little girls saying: I want to be Leonardo, but I will settle to be La Gioconda.
A contemporary story of Julanne, a young black girl who wanted to become a neurosurgeon, was related by Joyce Ladner in her study of black womanhood (1972). Julanne was the second of eight children who lived with their mother, a part-time cook. Ladner describes her as a brilliant girl who, at twelve, was selected for a summer enrichment program at a prominent private college. For her, this was the most outstanding event of her life; she lived in a dormitory and met students from all over the country. Precocious as she was, she had very firm ideas of what she wanted her life to be like. Yet at fourteen she became pregnant, dropped out of school, and had her child. When Ladner interviewed her she still had ambitions for returning to school, but confronted with the obstacles of poverty and motherhood at such an early age the probability that she would be able to achieve her goals seemed small.
The motif of ambivalence and conflict in the development of identity and personality in the young woman has attracted considerable theoretical interest (Bardwick, 1971; Douvan, 1970; Mednick et al., 1975). The culture prompts her very early to become sensitive to the responses of others, and to evaluate herself accordingly. She learns to be and to behave in ways that will maximize for her the powerful rewards of love, admiration, and approval. But to the extent that her self-esteem and sense of self become dependent upon such rewards, she is dependent upon the presence of significant others for their delivery, and she fails to develop internal criteria for an evaluation and definition of her self. Thus, she remains tentative in outline so that she may adapt more easily to the man she marries whose personality is as yet unknown. While such an adaptation to a future contingency does not necessarily lead to conflict, it does represent the deflection of considerable energy into the motivation to form affiliative relationships, within which her needs for positive response and affirmation of herself by others can be met.
At the same time however, middle-class girls as well as their brothers live in a society that values competence, mastery of skills, and achievement in the educational and vocational areas. To the extent that a girl is intellectually capable and has acquired these values, she can be expected to respond to early rewards for appropriate accomplishment by the development of a motive to achieve. Achievement by the young in our society is defined in terms of academic excellence, or mastery in a special interest area, such as music or sports. Since education is seen as crucial, and since all children go to school, successful achievement in that area is seen as highly desirable by parents and teachers and probably not less so for daughters than for sons. Now one can turn one’s capabilities to, let us say, academic achievement for two possible reasons. While they are not mutually exclusive, they may have differential strength as motivators. They are the pleasure of doing something well for its own sake, achieving an internalized standard of excellence—in Keats’s words, the fascination of what’s difficult; or the approval, recognition, and benevolent warmth which the achievement brings from others. Thus the bright girl conditioned already to seek out the latter can work hard and do well in school in the service of her affiliative needs without experiencing conflict between the two modes of behavior (Caplan, 1979).
But as she grows older, social pressure becomes very great to conform to a feminine image and to set for herself the eternal feminine goals of finding a mate and making a home. Now she is faced with a paradox because the feminine image does not include the display of intelligence, competence, and skill mastery, nor is it compatible with the high-level academic or vocational achievement. If she persists in manifesting these characteristics in the pursuit of such goals she may perceive herself and be perceived by others as unfeminine, and she may be unable to reconcile her achievement orientation with her interpersonal needs. Because successful achievement threatens to interfere with or to preclude successful affiliation leading to identity and performance as wife and mother, any serious contemplation of it as a major part of one’s life style is productive of anxiety and avoidance. The threat consists of two major obstacles, the evidence for which is all around her. First, if her successful achievement is unfeminine, then men will not find her desirable, and second, high achievement calls for difficult preparation and sustained effort, which may require deferral of affiliative goals.
Achievement tends to be redefined for girls as they grow older with the most drastic change occurring during puberty. During their school years, the ways that girls can achieve are not drastically different from those for boys. A girl who makes good grades, takes a leadership role in school activities, and is acceptable to her peers is praised for achievement just as the boy is for doing the same things. During and after puberty, however, new patterns of behavior take on achievement meaning for girls. Social skills, physical attractiveness, and popularity all become goals to which most girls clearly aspire, and which, while they are still in school, are not inconsistent with academic or leadership goals. These goals, highly salient during the pubertal years, comprise in themselves an area of achievement concern with its own standard of excellence (Stein and Bailey, 1973). This development, combining with pressure to conform to feminine role definitions and low expectations for adult female achievement in male terms, effects for many developing women a redefinition of achievement with its own standards and goals, very different from those of men and of her own childhood. While noticeable striving may simply drop out of some females’ repertoire, it may often be manifested in activities that are at least partially congruent with the feminine role. Such achievement behavior, while compatible with affiliative needs, is not simply a corollary to them but is itself a visible result of an internalized standard of excellence. While achievement is usually defined by what men do, many women may be just as strongly motivated to achieve different goals: interpersonal competence, an attractive, effective self, and, later, a harmonious, well-run household and healthy children, to mention just a few.
In the meantime, evidence is appearing that some highly competent college women are reevaluating old issues of conflict between career and family. When the doors of opportunity for women began to open in the 1970s, there appeared the model of the superwoman, she who combined a high-level career with the successful management of home and children, “having it all,” as it was called. The problems and stresses attendant upon that model have caused some to question its values, which include the determined pursuit of career goals while children of necessity are postponed or cared for by others.
Interviewed in the New York area, the women were college students aged eighteen to twenty-two, almost all of whom expected to attend graduate school or work after graduation. Most wanted to marry and have children, and they were concerned that it might not be possible to “have it all.” They were threatened by the high divorce rate and their perception that many successful women are unmarried. They saw the biggest problem as having children, and many planned to take time out to raise them even if it meant sacrificing their career advancement. “I’ve had enough of the superwomen with their top executive jobs and their seven children,” said a senior at Barnard. “I see no way someone with a fulltime job can take care of a kid.” Another, a prelaw student at Princeton, said, “I’m looking for solutions. It’s scary to me. I want both things and wonder whether having this great career is going to mean sacrificing the rest.”
Many of the women wanted to offer their children what their mothers had given them—the security of a mother to come home to. But most recognized that their twenties and thirties, the age of their mothers when they were born, were also the peak years of career advancement. Postponing having children until after graduate school and career security was an option considered by many. Interestingly, many of these young women did not identify with the women’s movement. In fact, they resented what they saw as feminist pressure to do everything they were capable of without providing answers as to how this could be done. They took for granted that jobs and opportunities would be there for them. But the sense is of a growing realization of the importance of family, too, and an unwillingness to sacrifice any of that experience in the furtherance of their own ambitions (Kleiman, 1981).
Fear of success
Thus the intellectually capable woman may perceive that she must make a choice or at best a compromise. Since her own affiliative needs are important, her sensing of the consequences of competitive achievement may give rise to the motive to avoid success (Horner, 1970; 1974).
The motive to avoid success is a stable personality characteristic that develops early in life as part of the learning of standards of gender-role identity. The explanation for the motive is given by expectancy/value theory, which proposes that the strength and direction of one’s behavior are determined by the belief or expectation one has about the probability and consequences of one’s behavior and by the value that one places on these consequences. According to the theory anxiety is aroused when one expects negative consequences to ensue from certain actions. The anxiety then functions to inhibit the behavior expected to have negative consequences. Thus for women, if success is seen to have negative consequences, actions or behavior that are pertinent to it arouse anxiety that in turn inhibits them. The motive to avoid success, then, is a disposition of women to avoid behavior that will have negative consequences such as rejection or threat to one’s feminine image.
Now it should be clear that the motive to avoid success is of variable potency in individuals, and may be absent altogether. It tended to be most important in bright women who had incorporated achievement as a value. If a woman does not desire to achieve and is incapable of doing so, then the behaviors leading to the inhibitory anxiety would not occur (Horner, 1974). A recent review of fear-of-success studies, however, reported that direct tests of the relationship between ability and fear of success do not support the theory (Mednick & Weissman, 1975). That is, one cannot conclude that the brighter the woman the more fearful she is of success.
Some other studies have examined the effects of mixed-sex competition on performance of women who are high or low in the motive to avoid success. Performance on achievement tasks was measured in a competitive mixed-sex situation, and compared to subsequent performance in a noncompetitive situation where achievement was relevant only to the task and to the subjects’ internalized standards of accomplishment. Female subjects who were high in the motive to avoid success did significantly less well in the competitive than in the noncompetitive situation, while those who were low, and most of the men, did better in the competitive condition (Horner, 1974).
While females do show a fear of success under certain conditions, it is not clear that they have a higher level of anxiety about successful achievement than males do. It may be that males and females equally experience fear of success as a motivational state, but that it affects the actual behavior of females more than it does males. The crucial test of the importance of fear of success as a personality characteristic is the extent to which it is correlated with behavior. Since both males and females experience fear of success, and gender differences have not been demonstrated, it appears that the underrepresentation of women among the high achievers has other determinants (Tresemer, 1977).
We may not know, then, the extent to which women more than men are motivated to avoid success. But it does appear that bright young women are less ambitious and less sanguine of achievement in conventional arenas than are their male counterparts. A recent study of one thousand Canadian university students yielded a syndrome called “the unambitious female.” Some of the correlates of the relative lack of ambition among these university women were perceptions of society’s prejudice against women, greater female anxiety and feelings that a “nervous breakdown” was imminent, lack of involvement of women in political activity in the university and the community, and greater involvement of women in social assistance kinds of activities, such as working for United Fund.
When the students were asked if men and women were equally able to make important decisions in business, politics, and the professions, 40 percent of the men and 26 percent of the women thought that women were less able. Most egalitarian in their views were men over thirty and women working for degrees in traditionally female fields. It appeared that women who associated in their studies with large numbers of other women had more respect for their own sex than did women in male academic and professional areas. Only 7.1 percent of the women were aiming at a profession, compared with 37.9 percent of the men.
The women students had higher scores on measures of anxiety, and reported more somatic distress than the men did. When asked for their reasons for feeling in a state of crisis, the most frequent cause given by men was worry over course work and exam pressure, whereas women most often cited trouble in personal relationships with men and with their families. Again, affiliative concerns were of more importance than were achievement concerns.
The male students were involved in more political activities, both in and out of the university, than were the female students. But when it came to “social acts”—working in organizations whose goals involved service to others—women were more active. Also, women were more in favor of a democratized university, progressive social action, and the abolition of inequity, but were less likely than the men to express personal willingness to take action and risk (Sutherland, 1978). These findings do not necessarily support a specific motive to avoid success, but for many young women their effect is failure to achieve to their potential.
Thus, success-avoidant behavior, especially in competition with males, may be important in the personality dynamics of many bright young women. And for them it means that sights will be set shorter, potential will be unfulfilled, talents will be wasted, and society will be poorer. At the same time some capable women do not show a fear of success and proceed to display achievement and to compete on an equal basis with males. What could account for the difference in fear-of-success motivational strength in women? What developmental events might promote a high dependence on love and approval and a fear that noncomformity with gender-role standards will lead to their withdrawal?
One theory holds that the female child is not adequately encouraged for early independence striving and for the development of an identity separate from her mother (Hoffman, 1972). This theory and the data supporting it are highly relevant to findings both on achievement motivation and success-avoidance motivation in women. Freedom from crippling emotional dependence on the approval and good will of others and a sense of oneself as an autonomous person clearly underlie the kind of commitment and willingness to extend oneself to take risks that characterize the high achiever.
Independence and competence are personality characteristics laid down in childhood as a function of the child’s experience with her caretakers and with her environment. Her optimum development occurs when the child has a secure emotional base in a warm, nurturant parent who permits exploration, encourages independent action, and is not too protective. Dependent orientation can result from parental behavior which threatens the child’s security, such as neglect or rejection, and also from overprotectiveness and failure or delay in providing experiences that encourage independent striving. The development of a sense of self occurs as the child increasingly becomes able to perform independent acts, to do things for herself, and to experience herself as a competent person.
Some studies show that parents are more protective of girls and grant them independence at a later age than they do boys (Hoffman, 1972). Since children pick up attitudes of their caretakers, it is not unreasonable to infer from such findings that girls begin under these conditions to sense themselves as less able and as more fragile and thus more in need of support and reassurance from others. Such rewards then become necessary for security, and any threat of their loss is anxiety provoking.
Related to the development of autonomy and sense of self are studies showing that strong mother-feminine identification is maladaptive both for psychological well-being and for achievement. Thus the daughter who is able to separate early from her mother and to develop confidence in her own coping abilities may later be more willing to test herself and to risk negative consequences in the pursuit of a valued goal. Indeed, the Feis longitudinal study found that “maternal hostility” was positively related to later achievement behavior in girls, while maternal protection and warmth related positively to boys’ achievement (Kagan and Moss, 1962). This does not mean that cold, rejecting mothers are good for girls. Rather, it is likely that a mother-son interaction which is seen as perfectly normal may be perceived as hostile when the child is female. This explanation reflects again the problem of comparing the sexes on some dimension in which the norms for males and females are different. It is highly probable that there is some optimum combination of parental support, encouragement of independence, and gentle disengagement that results in a self-confident, competent, non-anxious person whose sex is incidental.
Other Influences on Achievement
Achievement motivation and behavior are complex and can be influenced by many-variables. For example, women who are achieving in male-dominated occupations have common themes in their backgrounds. In their childhood and youth they had the opportunity to explore and to develop independently, and to witness a wide range of female and male models. They received encouragement and support for achievement, education, and the exploration of both “masculine” and “feminine” endeavors within a stable family structure. They tended to enjoy special status in the family, being a favored child or being the only or eldest child (Lemkau, 1979).
The relationship of birth order to achievement is especially interesting. Numerous studies have pointed to the over-representation of firstborns among high achievers. For example, a study of women doctorates in the United States found that 47 percent were firstborns (Astin, 1969). Most remarkable, a sample of 25 percent of the one hundred women presidents and vice-presidents of major business corporations revealed that all were firstborn and none had any brothers (Hennig, 1973).
An example of the influence of family environment on daughters appeared in a report on the family of Jerome Karie, co-winner of the 1985 Nobel Prize in chemistry. He and his wife Isabella, who participated in his scientific investigations, have three daughters, two with Ph.D.’s in chemistry and one in geology. They described the level of encouragement and expectation that was part of their childhood. “My parents took a great interest in what we were doing academically,” said one. “They set high standards, we should do well.” Another described how her parents encouraged an interest in science, taking their daughters on nature walks and hikes. “Our family vacations and our family outings maybe centered around science. Our toys were kind of geared that way.”{4}
If a girl is a first born or only child, or if she has only sisters and no brothers, her childhood experiences will be freer from competitive striving with boys. Such an environment appears to be salubrious for the development of achievement behavior in girls. The effect on females of absence of male peers, however, does not end in childhood. Women’s colleges, for example, have an outstanding record of graduating women who become distinguished for leadership qualities and for achievement. The absence of male competition in these settings brings out leadership abilities in women and motivates them to strive for academic excellence. Perhaps these qualities are less likely to be seen as unfeminine if there are no men around to set up complementary role standards. Women’s colleges have a ratio of women faculty to students which is twice as large as that found in coeducational institutions. A study of women achievers coming from women’s colleges found that a major influence in their development was the large number of women faculty. The greater the number of women faculty in the institution, the greater the number of women graduates who achieved distinction as measured by earning Ph.D.s and inclusion-in Who’s Who of American Women. In
The Development of Competence in Girls
A study of socialization strategies and patterns of childrearing which facilitate the development of competence and mature independence revealed four patterns of parental authority (Baumrind, 1972):
-
The authoritative parent who exercises firm control and sets limits, but values autonomous self-will and recognizes the child’s individuality. This parent encourages verbal give and take, solicits the child’s opinions, and gives reasons for policy decisions.
-
The authoritarian parent who values obedience, restricts autonomy, uses punitive control, and believes that the child should accept the parent’s word as final authority.
-
The permissive parent, affirmative and accepting, presenting her or himself to the child as a resource to be used as the child wishes. The belief of this parent is that the child should be free of all restraints except those required for physical safety.
-
The harmonious parent, who has control but does not exercise it. The child seems to know intuitively what the parent would want; thus the parent does not need to direct or command.
The difference between the authoritative and the harmonious parent may be more of degree than of kind. That is, the former may represent a higher level of interaction between members of the family or simply more explicit presentation by the parent of what her or his expectations are. It seems reasonable to believe that the harmonious style can be an evolution from the authoritative. That is, a parent who was authoritative with a very young child can gradually abandon explicit controls when the child has learned what the parent’s expectations are. In any case, neither the permissive nor the authoritarian model of parental authority promotes instrumental competence in girls because both shield and overprotect her, the one by placing no demands on her, the other by so structuring her life that she never learns to make her own decisions. With neither type of parent can she experience the anxiety of nonconformity because in the permissive situation nothing is defined as nonconforming and in the authoritarian setting nonconformity is not allowed. Thus, she has no opportunity to learn to handle such anxiety or to become desensitized to it. By contrast, in the harmonious and the authoritative families the child’s personhood is valued and respected, and competent, autonomous behavior is not only sanctioned but expected. In the course of testing limits and trying out autonomous behavior the child inevitably experiences the anxiety that comes from violation of norms—but she also learns the nature of real consequences and can make rational choices from the range of alternatives.
What are specific ways in which instrumental competence can be developed in girls? To ask the question should not imply that girls need a different kind of preparation than boys need, but it does point up the possibility that more conscious attention may be required for such a result in girls, who are less likely than boys to be assisted in the acquisition of such skills by prevailing social pressures. Girls should be taught to compete in sports and other contests and to win and lose gracefully (Baumrind, 1972). Also, girls can learn to be assertive in defense of their persons and their rights as individuals. This does not mean an obnoxious insistence upon having one’s own way all the time or a selfish disregard for others, but it does mean having a clarity of vision into the merits of a situation, so that one can rationally insist upon justice, and not need to fall back upon a plea for mercy. Finally, girls should be socialized to assert their individuality and to be independent of pressures either to conform or to rebel. The independent person does not display a mindless obedience to illegal authority or a conformity to irrelevant social norms, nor does she resist or violate them purely as a response to peer and other pressures to do so.
Instrumental competence is a drab phrase to describe the development of skills and powers that can enormously expand experience and enrich life for all humans. John Stuart Mill, speaking more than a century ago of the benefits of the extension of full equality to women, said that for them it would mean the difference “between a life of subjection to the will of others, and a life of rational freedom. After the primary necessities of food and raiment, freedom is the strongest want of human nature...” (1973, p. 238). At the same time the American poet Walt Whitman had a vision of women who are
... not one jot less than I am
They are tann’d in the face by shining sun and blowing winds, Their flesh has the old, divine suppleness and strength,
They know how to swim, row, ride, wrestle, shoot, run, strike, retreat, advance, resist, defend themselves,
They are ultimate in their own right. They are calm, clear, well possess’d of themselves (p. 117).
Surely, to be ultimate in one’s own right is what instrumental competence is all about.
Moral Development: In a Different Voice?
Theorists of human development, as we have seen earlier, have almost always held the male to be the prototype of the human being, such that their constructions of human development were really models of male development. As we noted in Chapter Two, both Freud and Erikson proposed developmental theories that explained male development, and it was only later, and with questionable goodness of fit, that explanations for female development were incorporated into the theoretical system.
Theories of moral development—that is, the growth of concepts of moral principles as guides for behavior—have likewise been built upon male models. A classic in the Held is Jean Piaget’s The Moral Judgment of the Child (1932). Throughout, “child” is assumed to be “boy,” whose moral development procedes from the learning and elaboration of rules of the complex games of boyhood and the invention of procedures for settling disagreements and conflicts. This process results in the development of a sense of fairness, of an understanding that rules and codes of conduct are necessary to maintain the social order. Such rules and codes, based on justice, provide a base for the making of moral judgments. Girls receive scant attention in Piaget’s work and are treated as an anomaly to the theory. Girls play simpler, less ridebound games and treat rules more casually. Thus the sense of lawful conduct “is far less developed in little girls than in boys.” (p. 77).
The most extensive research on moral development is that of Lawrence Kohlberg (1963, 1981). Based on a twenty-year study of a sample of males who were aged ten to sixteen when the study began, Kohlberg developed a model for moral development that consists of six stages, presented as a fixed sequence of universal principles that should apply everywhere, independent of specific situations. These stages are levels of perspective on social and moral events. The method Kohlberg used involved the presentation to subjects of a series of stories and dilemmas that embodied moral issues. The best known of these is his “Heinz dilemma,” in which the husband of a woman who is dying of cancer, unable to raise enough money to buy a drug that may help her, breaks into a drugstore and steals the drug. Should he have done that? is the question. From subjects’ responses, their level of moral development could be determined on the six-stage scale. The content of the stages is as follows:
-
Stage 1: deference to power. Goodness or badness is determined by the dictates of authority.
-
Stage 2: doing good to serve one’s own ends. A person helps someone because he himself may need a favor later; or he hurts someone to get even.
-
Stage 3: care for the other. Moral behavior is in the context of interpersonal relations. Generosity, helpfulness, and concern for the needs of others are of primary importance.
-
Stage 4: the primacy of the social order. Morality is seen in terms of maintaining the orderly structure of society, by being a good citizen, working hard, and following the rules.
-
Stage 5: creation of the social order. The individual tries to improve on society, to insure the values of equality and liberty, rather than accept and obey, as in Stage 4.
-
Stage 6: primacy of moral principles. Certain principles are absolute, such as the value of human life as an end in itself. While the social order is valued, it is not an end in itself, and one is morally obligated to defend human rights and social justice if they are threatened by the social order.
According to Kohlberg, stages 1 and 2 are most frequently found in ten-year-olds, while Stage 3 predominates among thirteen-to sixteen-year-olds. Stages 3 and 4 may characterize most adults. Stage 5 is rare, and Stage 6 exists only as a theoretical end point of the system, being almost never found in anyone, except in such rare persons as Gandhi and Thoreau (Kohlberg, 1978).
Kohlberg’s system of moral development has stimulated a great deal of research and some criticism as well. His claim of the universality of the sequential stages has been challenged, on the grounds that the higher stages reflect the values of Western, democratic societies, thus embodying the ethnocentric assumption that other political and social systems are less morally advanced (Simpson, 1974).
The theory has been challenged on other grounds as well. The system was developed from studies of adolescent males; thus it is vulnerable to the critical question of its validity for females. This question has been raised, most notably by Carol Gilligan in her book In a Different Voice (1982). Women’s responses to Kohlberg material, Gilligan noted, are most often scored at Stage 3, the stage at which morality is defined in terms of care for others, not hurting others, having a responsibility for the welfare of others with whom one is connected. This has the effect of generally lowering women’s scores compared to men’s, who often score at 4 or even 5. Does this mean that women are less morally advanced than men are, as Freud and others have believed? Gilligan’s work sets forth her theory that women, in no way less moral than men, are different from men in their moral development and in their basic principles of morality. Thus, she argues, women score lower on Kohlberg’s scale because it is sexually biased toward a masculine model of moral development that is less relevant to women’s values and experiences.
The origins of this difference are in women’s childhood experiences as the daughters of mothers. While both boys and girls are nurtured by the mother and have their earliest identification with her, boys must detach themselves, separate themselves from their early oneness with their mother, and pursue a separate path toward masculine identity. Having severed this first and most important connection, in the psychic sense, they then develop and value ways of resolving interpersonal issues and conflicts through systems of rules and laws that not only regulate conduct but provide standards and codes for moral behavior. Girls, by contrast, nurtured by one of their own sex, can continue their identification and their connectedness with her. This connectedness, and its meaning in the mother-daughter relationship, gives rise to an ethic of care and the avoidance of causing hurt to others. Thus women’s moral judgments are more likely to be made in terms of their meanings in the contexts of relationships and the people involved, rather than in terms of societal rules:
The psychology of women that has consistently been described as distinctive in its greater orientation toward relationships and interdependence implies a more contextual mode of judgment and a different moral understanding. Given the differences in women’s conceptions of self and morality, women bring to the life cycle a different point of view and order human experience in terms of different priorities (Gilligan, 1982, p. 22).
Gilligan’s theoretical work grew out of her research on moral development in children, college students, and women making the decision to have or not to have an abortion. While her results so far are supportive of her theory that women’s developmental course leads to different outcomes where morality is concerned, some have questioned the initial findings that women in fact score lower than men do on Kohlberg’s scale (e.g., Walker, 1983) when relevant variables, such as education and occupational level, are controlled. But if women base their moral judgments on different grounds than men do, then that in itself would call for the construction of a model for women’s moral development, which could then be tested and evaluated as Kohlberg’s has been for men.
Values and Interests
The values and interests of females collectively are different in important, measurable ways from those of males in this society. Several decades ago a scale to measure the strength of certain values in the individual’s personality was developed (Allport and Vernon, 1931). Adopted from the earlier work of Spranger, a German philosopher, the values are defined as follows:
-
theoretical: interest in the discovery of truth; a critical, rational, “intellectual” approach;
-
economic: emphasis on useful, practical things; a “hardheaded” approach;
-
esthetic: valuing form and harmony; enjoyment of grace, symmetry, and fitness;
-
social: interest in helping people, in philanthropy; altruistic; political-, valuing personal, power, influence, and renown;
-
religious: concern with the unity of experience; mystical; seeking to understand the universe as a whole.
Studies using this scale have consistently found large sex differences in all the values. Women are much higher in esthetic, social, and religious interests, while men show more strength in theoretical, economic, and political areas (see Fig. 6.4). It is not difficult to see the relationship between these values that women hold and the kinds of work and activities that they usually do. But even when males and females of similar ability are engaged in the same kind and level of activity, their values and interests are different as are the personality characteristics they bring to the situation.
One study investigated the abilities, interests, and values in seven hundred girls and thirteen hundred boys taking a high-school physics course in an attempt to shed some light on the matter of the paucity of women in science and their relative lack of eminent accomplishment. Since physics is seen as a masculine subject and relatively few girls take it, one might expect that those who do would be more similar to males in their values and interests. But a comparison of Figure 6.4 with Figure 6.5 shows that the large sex differences in values observed in a general population were just as prominent for physics students almost four decades later (Walberg, 1969).[23] The girls scored higher than the boys on Esthetic, Social, and Religious, results implying, respectively, greater valuing of form and harmony, greater interest in people, and more concern with the unity of experience and with mysticism. 4 he largest differences between the sexes were on Economic and Social values. The author thought that this difference might reflect the students’ preoccupations during the last year of high school: boys’ thought of making a living and girls’ concern for homemaking and family life.
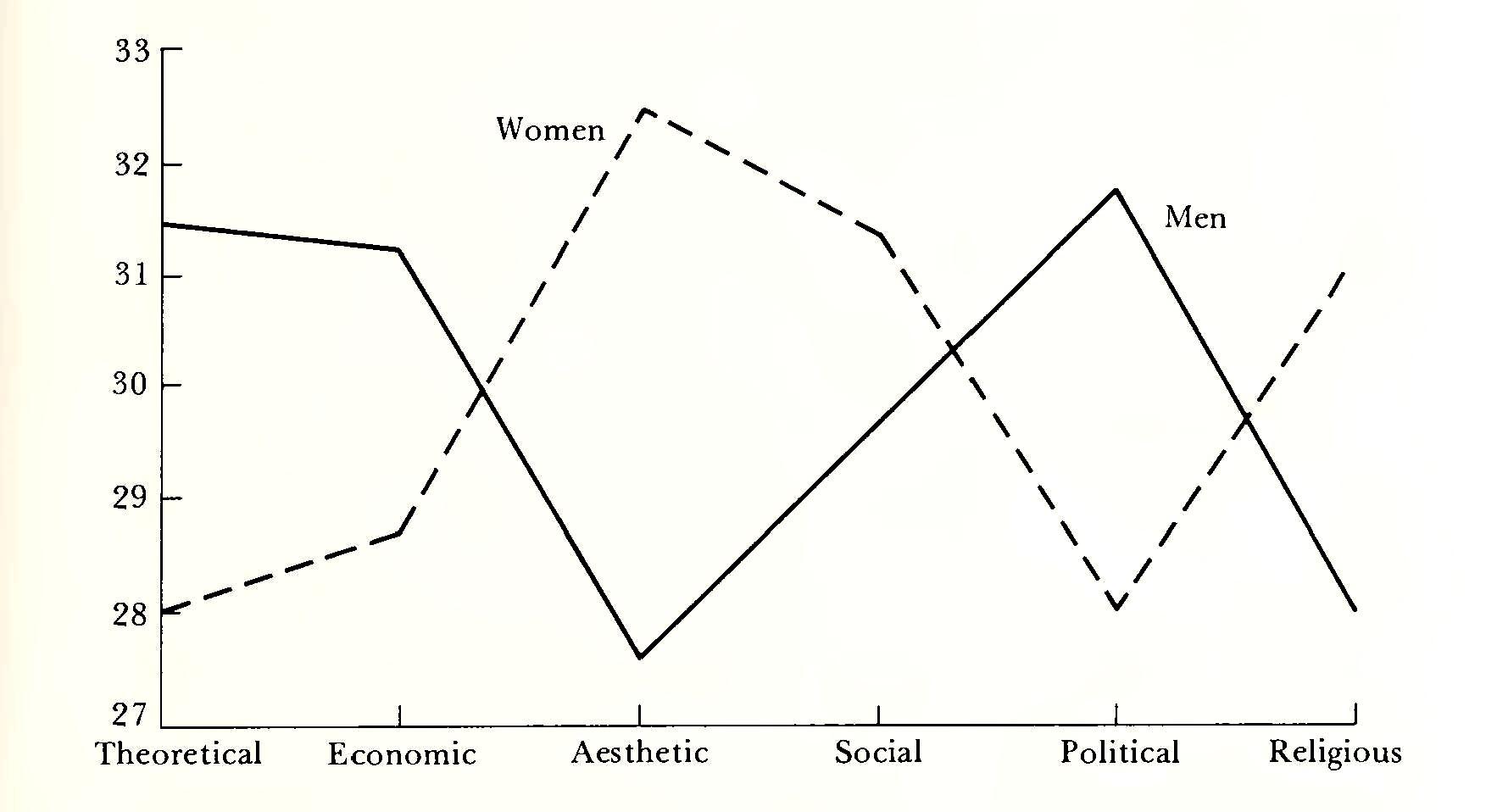
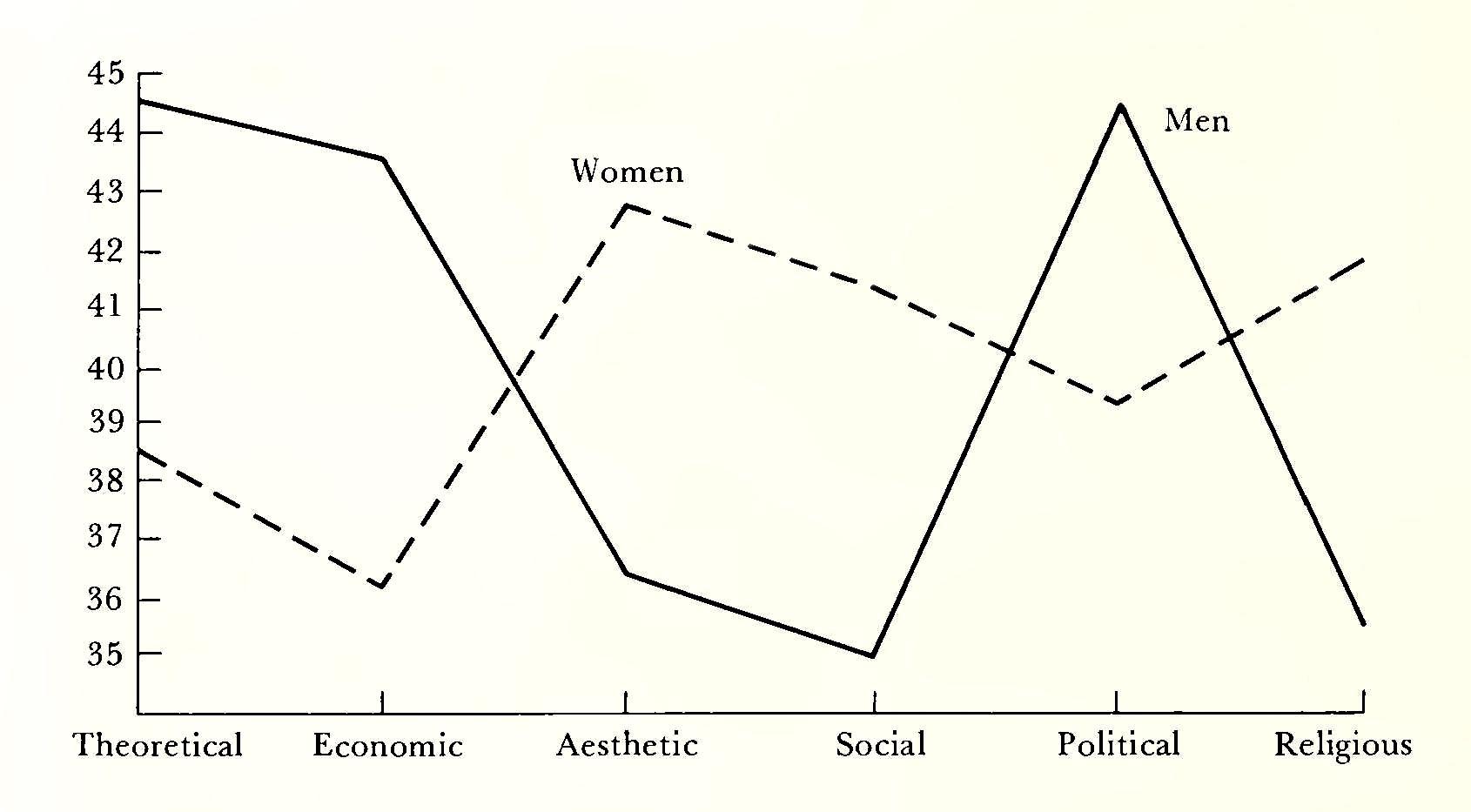
Furthermore, this highly selected sample of girls (their mean IQ was 118, significantly higher than the boys’ 113) differed from the boys in their self-initiated scientific activities. They liked to participate in activities involving nature study and the applications of science to everyday life, like collecting insects or bird nests and learning about nutrition and how the body uses food. The boys were more likely to show interest in cosmic questions of time, space, gravity and to spend some time in scientific tinkering with machines and electronic equipment. Girls were more interested in the life sciences and their application, boys in abstract ideation and the physical manipulation of objects.
Medicine, another field which is atypical for women, might also be expected to attract persons with common values and interests, regardless of sex. But a study of seven consecutive classes of entering medical students found that the women differed from the men in ways similar to those observed in other studies of more typical samples (Cartwright, 1972). They saw themselves as more willing to express feelings, and to admit weaknesses, and less likely to endorse the extremes of dominant and aggressive behavior. On personality tests they were more responsible, more highly socialized, and more tolerant. They were more sensitive to relationship values, and more alert to moral and ethical issues. While the direction of all these variables seems typically linked to their sex, two were the opposite of a prediction based on sex: the women valued independence and individuality more highly than did their male colleagues. But the independence and nonconformity that probably facilitated their choice of an atypical career coexisted in their value system with concerns that have traditionally been more characteristic of women.
Thus the values and interests of women, even of those in atypical fields, distinguish them from men. These characteristics, as well as social prejudices and lack of opportunity, may have worked against their emergence in any numbers among the eminent creators of civilization. In a study of creative scientists, thirteen distinguishing traits were found (Taylor and Barron, 1963). Another study of sex differences of physics students revealed that seven of those thirteen traits distinguished the males from the females in the samples (Walberg, 1969): 1. a high degree of autonomy and self-sufficiency; 2. a preference for manipulations involving things rather than people, a detached attitude in interpersonal relations; 3. a high degree of personal dominance, but a dislike for personally toned controversy; 4. a high degree of impulse control, with relatively little inclination to talkativeness, gregariousness, or impulsivity; 5. a liking for abstract thinking; 6. rejection of group pressures toward conformity; and 7. interest in trying oneself in uncertain circumstances in which one’s own effort can be the deciding factor. To the extent that these traits distinguish not only creative scientists but also males, from females in scientific fields, there is a discontinuity, at least in science, between women’s characteristic traits and values, and those distinguishing persons who become noted for creative achievement.
Though interests and values sometimes change drastically during adolescence, they become fairly stable attributes of the person in adulthood. Learned under the conditions of experience and socialization, they influence behavior and contribute to its direction. Attempts to understand and to explain the differential roles and outcomes for females and males can be enriched by considering the differences in what is important to them, what they care about.
Most studies of values that have included females have emphasized gender differences and have been concerned with abstract and generalized concepts, as in the Allport scale, or in interests relevant to occupational achievement. But what are the personal values of adolescent girls in our society, most of whom are not going to pursue careers in science, medicine, or academia? A nationwide study of adolescent girls provided some insight into this question (Konopka, 1976).
There was a strong emphasis on autonomy, on the right to be recognized as an individual whose rights were equal to those of all other individuals. They valued family life based on mutual respect and trust between men and women. Family life included having children, though they wanted the freedom and responsibility of having choices about that. Material goods were important to them too, especially to those from poverty backgrounds. Some upper-income girls, however, totally rejected what they saw as the materialistic life styles of their parents, even though they took the comfort and luxury of their own lives for granted. Most saw education as a means of fulfilling life goals, especially if it included participation and actual involvement. They did not want to be forced to be exclusively listeners and receivers of information. Honesty and trust were seen as the cornerstone of human relations; most wanted desperately to be trusted and were willing to return that trust to others.
The girls valued justice and equal treatment for all people regardless of race, sex, or national origin. They were much more concerned with cooperation than with competition, and related to this in their value systems was open and gentle intimacy among people. They were turned off by superficial and cold relationships. Though they wanted sex to be discussed openly and did not consider premarital sex a sin, they wanted it to be part of a genuine and responsible relationship. Finally the girls wanted to find meaning in life, at a time in their own lives when doubts were especially strong as they sought to find their identities as individuals. They wondered what they should believe in and what they should reject. The common motif among them seems to be idealism, with the expectation that the working out of these values in their own lives is possible. Resilience and hope characterized girls from all kinds of backgrounds and ways oi life, even those whose own life experiences were the antithesis of the values they cherished.
Familial and social processes shape the experience of a girl in ways that result in special outcomes for her. Identification with her own sex and with its characteristic role is learned early by most girls. Her socialization gives her perceptions and learnings that show her clearly where her “place” will be. As she matures, she may find that she has to make choices that boys do not need to, and that something of herself gets lost in the process. By adulthood the values and interests of women are very different from those of men, and while these interests are functional for the role women are socialized for, of themselves they may be inadequate for other kinds of achievement in the larger world.
It is surely not accidental that women occupy few positions of leadership and power in the society. Two major explanations have been advanced to account for this. One rests on the greater aggressiveness of the male that serves practically to insure that more men than women will seek those positions that carry with them some degree of power over others.
On close scrutiny, however, such a causal link between aggression and leadership or the exercise of influence in the society seems rather weak. Our society does not value overt aggression and tries to socialize it out of children of both sexes. The emerging ethos in political and business leadership seems to favor less reliance on the flagrant use of power or show of strength and more emphasis on leading others by defining mutual goals and by cooperative effort, a style of leadership that women might find more to their liking.
In a modern society most roles do not require either high levels of aggression or the ability to forcefully dominate others. Perhaps those that do will continue to be sought after by men more than women. In any case, an explanation based on the idea that men are naturally more aggressive fails to substantially account for the great differences in outcome for girls and boys.
The other major explanation lies in the different sets of experiences of the two sexes as they are socialized to be members of the society. These experiences, by which girls learn to be attractive and pleasing so that they can attract a husband and enter into a domestic and nurturing role, and by which boys learn that they must prepare themselves for positions commensurate with their abilities reflect old and stable needs and values of the society that do not give way easily to pressures for change.
However, as the needs of the society change, so do its values, and the exceptional and the unacceptable become commonplace and acceptable. Society no longer needs to prepare girls for a lifetime of domesticity, and other qualities in addition to those related to expressiveness can now be encouraged and valued. Girls can be socialized to be competent, and when they are both competent and expressive, instead of expressive only, they are psychologically healthier. While little is known about the effect of a comparable balance in males, it is conceivable that both competence and expressiveness, instead of competence only, would result in healthier personalities for them too. As girls and women acquire skills and competencies relevant to the many social roles heretofore held by males, their display of these will become commonplace and accepted, and many will acquire the confidence which, more than aggression, is necessary for leadership. When all conditions for the acquisition of competence and confidence become equal for girls and boys, then we shall see what the contribution of nature to woman’s “place” really is.
7. Sexuality
Sex is intimate physical contact jor pleasure, to share pleasure with another person (or just alone). You can have sex to orgasm or not to orgasm, genital sex, or just physical intimacy—whatever seems right to you. There is never any reason to think the “goal” must be intercourse, and to try to make what you jeel fit into that context. There is no standard of sexual performance “out there,” against which you must, measure yourself; you aren’t ruled by “hormones” or “biology.” You are free to explore and discover your own sexuality, to learn or unlearn anything you want, and to make physical relations with other people, of either sex, anything you like.
—Shere Hite, The Hite Report, 1976
During the past two decades, the surge of interest in women—their lives, their histories, their rights—has been accompanied by a growth of recognition of the significance to women of their bodies and of the expression of their sexuality. From the “sexual liberation” motif of the 1970s to the “new celibacy” advocated by some for the present decade, the trend has been in the direction of giving women more knowledge about their bodies and their sexuality, as well as more autonomy and control over their bodies, and more options from which to choose. The new climate of appreciation for women’s sexuality as equal in importance to that of men is reflected in both popular and scholarly literature, but, even so, when women themselves describe their actual experiences, it often appears that the chasm between the contemporary ideal and real life is still wide (Ross, 1980).
The sexual nature and experience of women is rich and complex. It is often misunderstood and misinterpreted. Women themselves, young and older, frequently display a lack of knowledge of their own bodies and capacities for sexual experience which one is tempted to characterize as a kind of developmental lag. On the other hand, some women of all ages and of all times have without doubt enjoyed the discovery and exploration of their own sexuality to the fullest. In this area of human behavior, females have displayed greater variability than males. That is, the range of such variables as frequency of orgasmic response and reported interest in sexual activity is greater for females than for males. For example, it is not uncommon to find that an adult woman has never had an orgasm. At the other extreme, some women have been known to have had as many as fifty orgasms in an hour (Masters and Johnson, 1966). It is probably safe to say that no physically intact adult male has not had some form of orgasmic experience; nor, on the other hand, has any male had fifty orgasms in an hour. While there may be in the annals of human lore reports of exceptions to the above, the research supports the generalization of greater female variability.
Attitudes toward and beliefs about sexuality, as well as sexual behavior itself, vary widely from culture to culture and from era to era. Manners of manifesting the sexual drive and the forms and meanings of its acting out are carefully prescribed and codified in human societies. These prescriptions and codes are part of the social learning of the members of a society, though much of the learning of these is of an informal nature. In Western society, as in most others, the behavior of women has been more carefully and rigidly defined and regulated than has the behavior of men. In the past, this has had the effect of obscuring the “true nature” of female sexuality. It is only within recent years that a relaxation of sexual codes and the undertaking of serious research into the matter have begun to inform us about the nature and potential of female sexuality.
At the present time we are witnessing an increasing acceptance of the idea of sexual equality and of the individual’s right to seek her own personal modes of sexual expression and fulfillment. While these ideas are not new in human history, they are new as an emerging ethos of this generation. They have the potential for providing new insight into old problems of sex and sexual relationships, such as the role of biology in sexual activity, sexual response patterns, sexual behavior as a function of social norms, effects of psychological factors on sexual functions and dysfunctions, and variations from the conventional model of the heterosexual dyad.
While sex and sexuality have always been of interest and concern to humans,[24] the intense search for objective knowledge about them is a feature of contemporary science. Scientific disregard for the subject of sexual behavior reflected prevailing attitudes and mores during the last century especially, for that era generally held that discussion of the subject was taboo, except within a highly moralistic framework whose intention was to describe what was proper and acceptable. In such a climate, scientists and nonscientists alike were constrained by the code of silence and by a belief which rigorously defined both the style and the limits of sexual behavior.
Women and Sexuality: Historical Perspective
In order to understand the role and significance of sexuality in women’s lives today, we need to look at some historical trends in attitudes about women and sexuality. How did these attitudes arise and how have they affected the relations between women and men?
We have seen in other contexts that women, until recent times, were regarded basically as property. That is, a woman, her body and her goods, literally belonged to a man, first her father, then her husband. According to contemporary theorists, the institution of marriage arose through the reciprocal exchange of women by tribal groups. The value of this was the formation of alliances between groups through the elaboration of kinship systems, thus strengthening the original family. The giving away of sisters and daughters became an insurance against extinction (Levi-Strauss, 1969).
The value of women as items of exchange lay in their identity as sex objects and reproducers. From this practice and this identity, there arose the ideology of virginity, the belief that a girl or woman had value as a bride only if she had never “belonged” to another man. This ideal is an aspect of male property rights that has always been supported, up to the present time, by men and women alike— men, because it gives them control over women as a class; women, because in societies where they are economically powerless, it is a prized resource by which they can obtain security through marriage (Berger and Wenger, 1973). Since male virginity has never been similarly valued, a powerful double standard for the expression of sexuality has typically pervaded attitudes and beliefs about women and sex since earliest times.
The concept of woman as property merged during the early Christian era with beliefs and attitudes about sexuality. Chastity and asceticism became synonymous with holiness; marriage was a sorry state, to be contracted only in direst need or for procreation, and the status of women declined accordingly. At best, the woman was a silent, submissive wife; at worst, she was the instrument of damnation, exciting lust and enticing man away from more important pursuits. The man was not made for the woman, but the woman for the man. “Wives, submit yourselves unto your own husbands ... as unto the Lord. For the husband is the head of the wife, even as Christ is the head of the church” (Ephesians 5: 22–23).
Attitudes toward sex became somewhat more positive during the sixteenth-century Protestant Reformation, even though women, their bodies, minds, and functions, continued to be denigrated. Martin Luther in his Table Talk said that women had narrow chests and broad hips because they were destined to “remain at home, sit still, keep house, and bear and bring up children” (Luther, 1890, p. 299). Even though he held women in low esteem, he advocated marriage, knowing that celibacy was an elusive goal for most, including the clergy. One of his contemporaries, John Calvin, also favored marriage over its alternatives, though he recommended restraint and modesty in marriage as in all else. The renunciation of pleasure and worldliness was a strong theme of his, and their equation with sin and the evocation of guilt continued to permeate Western ideas about sex and morality until recent times (Rugoff, 1971).
During the eighteenth and nineteenth centuries, the Romantic movement began, with its emphasis on nature, freedom, deRance of traditional mores, and the ascendancy of the individual. Sexual love was imbued with divinity, and emotions, rather than cool reason, were the guides to truth and happiness. Romanticism was the antithesis of conventional bourgeois marriage, arranged for practical reasons of family and patrimony. The Romantic might marry, but only for love and its passion. The Romantic tradition waned with the influence of the Victorian era, but its thematic ideas of the relationships among love, sex, and marriage continue to be important, and its rejection of traditional values echoed through the Victorian counterculture, the bohemian ethos, and the emergence of the widespread acceptance of sexual freedom in modern times.
Only Yesterday: The Victorian Context
It has been suggested that “our culture is gradually convalescing from a sexually debilitating disease: Victorianism” (Brecher, 1979, p. 324). It is no novelty to observe that the Victorian era was highly repressive of all aspects of sexuality, but the truly morbid flavor of the middle-class teachings of the times can best be savored by examination of the original sources. The prudery and propriety of the time were exemplified in books and articles on health and hygiene, and in pamphlets on religion and ethics (Haller and Haller, 1974). The prevailing message was chastity, continence, even in marriage, and self-control, which meant denial of sexual desires and avoidance of all .temptation, especially for women.
Since sexual intercourse was approved only for the purpose of procreation in the marriage relationship, young girls were admonished to avoid all sources of possible stimulation which might lead to the misstep that would ruin them for life. The worst of these was masturbation, the “solitary vice,” which brought the threat of disease, mental derangement, and future childbirth complications. Romantic novels, dancing, and “unnatural” affection for other girls carried the seeds of disaster. They contributed to premature sexual development and introduced girls to impure thoughts and actions for which they would pay dearly later.
The young girl was advised to be passive in relations with males. She was to be courted and pursued, and perhaps caught in marriage, but without any contrivance on her part. Boldness and immodesty were equally deplored mainly because of their effect on the young male, who might lose control and make an improper advance. Male writers warned of the untrustworthiness of males where females were concerned. The tenor of these warnings suggested that male lust was barely held in check, and that it was up to the female to make sure that no provocative act of hers unleashed it.
Many women entered marriage quite ignorant of sex. In fact, one writer said that there were some women into whose minds the thought of sexual intercourse had never entered (Haller and Haller, 1974). The manuals, however, did not dispel such ignorance of the facts. Rather, the emphasis was on avoidance and restraint. Since men were considered naturally aggressive, it was up to the wife to maintain decorum in the marriage bed by her passivity and lack of passion. It was her duty to submit to her husband’s embraces, but she must not react with desire or pleasure. Orgasm must be avoided because it interfered with conception, inducing a relaxation and weakness that could lead to barrenness.
Since intercourse was approved only for the purpose of procreation, separate bedrooms were advised to avoid temptation and to cut down on excessive stimulation of the male. The moral dictum which confined sex to reproduction was reinforced by the teaching that excessive ejaculations would have a debilitating effect on the male. On the other hand, reserves of seminal fluid in the conservative male would have a beneficent effect upon his mental activity and productivity.
The derogation of sex as an activity which should be engaged in as seldom as possible and enjoyed not at all by women was a residual of the ascetic doctrine of early Christianity. During the Victorian era, however, it became part of the value system of manners and morals which was supposed to set the middle class apart from such earthier citizens as immigrants and slum dwellers. The effect of such views, widely promulgated by physicians, preachers, and self-appointed moralists, was to generate a climate of attitudes about sexuality whose effects still characterize our “convalescence.” We saw in chapters 2 and 3 how this climate affected psychoanalytic views, especially of female sexuality, and the recognition of its derogatory consequences for women by such observers as Clara Thompson. As early as the turn of the century, however, others began to speak out in dramatic opposition to the approved wisdom, and in the course of time a few works appeared which attempted to introduce objectivity into the discussion and to place sexuality in perspective as an aspect of human behavior worthy of investigation. Sex research gradually became respectable, and information based upon systematic study of sexual phenomena became widely available.
The Study of Human Sexuality
Although the scientific study of sexual behavior began as a midtwentieth century phenomenon, it has its origins in the turn of the century with the work of Havelock Ellis, an English physician whose Studies in the Psychology of Sex were published in six volumes between 1897 and 1910. Ellis’s contributions went far beyond clinical study of patients, drawing upon anthropological and medical material, case studies and life histories. His vast collection of data from cultural groups all over the world showed the variability of sexual norms, and it introduced a new idea to the Western world: “Not everyone is like you”. Although Ellis endured considerable vilification for his views, he argued for sex education, trial marriage, legal immunity for sexual acts of consenting adults, and removal of sanctions against sexual experimentation.
Emphasizing normal human sexuality, Ellis’s findings startlingly presage many findings of contemporary research. Masturbation and other sexual responses appeared early in life and were common for both girls and boys. Women’s sexuality reached its peak later than men’s and continued strong late into life. The prevalent notion that women had little or no sex drive was a myth. The orgasm was similar for both men and women, but the multiple orgasm was common for women, whose pleasure was enhanced by prolongation of the sex act. Frigidity in women, a common phenomenon at that time, was the result of repression of sexuality in girlhood and male ignorance of female sexuality, particularly the importance of the clitoris.
Ellis was an advocate of sexual equality for women, and he worked for the reform of divorce laws and for the abolition of laws banning the promotion and sale of contraceptive devices. Shortly before his death in 1939—also the year of Freud’s death—he expressed his delight that the Victorian attitudes against which he had battled for so long were beginning to change. “I cannot see now a girl walking along the street with her free air, her unswathed limbs, her gay and scanty raiment, without being conscious of a thrill of joy ... that I am among people that are growing to be gracious and human.”[25]
In 1926, a Dutch gynecologist, Theodoor van de Velde, published Ideal Marriage, which became one of the best-selling sex manuals of all time. In spite of its quaintly Victorian title, the book was concerned with showing this first post-Victorian generation how to develop and maintain enjoyable sexual relationships. Van de Velde had learned from his patients that love and affection were not enough to insure a good sexual adjustment in marriage. He therefore addressed what he saw as the two most common problems: Erst, the introduction of the virginal bride to the joys of sexual responsiveness by her loving and desirous (and presumably more experienced) husband; and second, the maintenance of enthusiasm, excitement, and novelty in sex over many long years of marriage. Van de Velde did not concentrate on one sex or the other, but rather was concerned about mutuality in the sex act. He emphasized the importance of the adequate arousal of the woman, and of her need for longer stimulation to achieve orgasm. Many women were capable of and wanted to have several orgasms; the sensitive male would be sure she was satisfied before he reached his climax. Both clitoral and oral-genital stimulation were described in detail. However, van de Velde saw these as acceptable and desirable in foreplay, in preparation for intercourse, but not as substitutes for penile-vaginal orgasm. Even so, he lifted them out of the catalog of perversions. Van de Velde was one of the Erst to give equal importance to the sexual satisfaction of the woman. If the husband climaxed first, and his wife was not yet satisfied, he should stimulate her genitals manually until she had an orgasm. If this did not work, it was perfectly acceptable for her to masturbate herself to her satisfaction. Van de Velde even quoted a Catholic treatise by a French cleric which sanctioned this radical advice.
Another student of female sexual response was Robert Dickinson, an American gynecologist, who with Lura Beam documented the continuing effects of Victorianism in A Thousand Marriages (1932), and The Single Woman (1934). Based on hundreds of detailed sexual histories of his patients, these books painted a dismal picture of women’s sex life in marriage. Dickinson described the characteristic coitus as brief and oriented toward male satisfaction. Without preliminaries, it occurred once or twice a week, lasted about five minutes, and ended when the male achieved orgasm. The woman submitted without excitement, expecting exactly what she got— nothing.
Dickinson did more than report histories. His classic Atlas of Human Sexual Anatomy (1933) contained detailed drawings of the vagina in various stages of sexual stimulation. He obtained the information by inserting a glass tube resembling a phallus into the vaginas of dozens of his patients. He observed the changes which occurred in both the vagina and the cervix as they stimulated themselves. By this process he was able to lay to rest at least one myth, that at the moment of orgasm the cervix opened and sucked up the deposit of semen. Such opening was very rare, and was not accompanied by any sucking action. Dickinson also pioneered the use of the electrical vibrator to help women learn to reach orgasm. Applied to the pubic area above the clitoris, this device gives erotic stimulation which leads to orgasm in many women who have previously been unable to experience it. Dickinson demonstrated the use of the vibrator to patients, who subsequently found themselves able to reach orgasm by masturbation or coitus.
Social changes following World War II eroded many traditional attitudes toward sex and sexuality, and research on the psychology and physiology of sexual response appeared in the arena of modern science. The most important studies for female sexuality were those of Alfred Kinsey et al. (1953) and William Masters and Virginia Johnson (1966; 1970).
Kinsey was an entomologist at Indiana University in the midthirties when he was selected to teach a course on sexual behavior. Discovering the paucity of scientific research in the field, Kinsey embarked upon the most extensive study of the sexual habits of white,[26] mostly middle-class Americans. Through personal interviews, he collected the sexual histories of more than five thousand males and more than five thousand females. The data from these samples are the basis for Kinsey’s first book, Sexual Behavior in the Human Male, and his second, Sexual Behavior in the Human Female. These studies deal primarily with the frequency and variety of sexual outlets. Although questions have been raised about their validity and the degree to which they are representative of the sexual habits of the entire population, they continue to be the most complete and reliable sampling available (Brecher, 1979; Katchadourian and Lunde, 1975). Their publication created a furor because of some of the findings, especially on the incidence of premarital sex and homosexuality. They also challenged some cherished myths about the sexual behavior of females.
The studies of Masters and Johnson differed in important ways from those of Kinsey. They were interested in the physiology of the sexual response from arousal through orgasm and back to the quiescent state. To learn what happens in the human body through the sexual response cycle, they used the method of direct observation of subjects in a laboratory setting. Their sample consisted of 694 males and females, white and black, ranging in age from eighteen to eighty-nine. As a result of this research, the book Human Sexual Response appeared in 1966.
Sexual Anatomy
The female sexual anatomy serves both sexual and reproductive functions. It consists of the external genitalia and the internal reproductive structures. Although all these structures belong to a single body system, the external genitalia are more closely associated with sexual activity, and the internal organs with procreation. The origin and sexual differentiation of this system was described in Chapter 4.
External genitalia
The external female genitalia include the mons pubis; the major and minor lips, called labia; the clitoris; and the vaginal opening, or introitus, which is flanked on each side by erectile tissue called the vestibular bulbs (Fig. 7.1).
The mons pubis or mons veneris, “mount of love,” is the most visible of the external genitalia. It is a rounded area of fatty tissue which becomes covered with hair in the course of puberty.
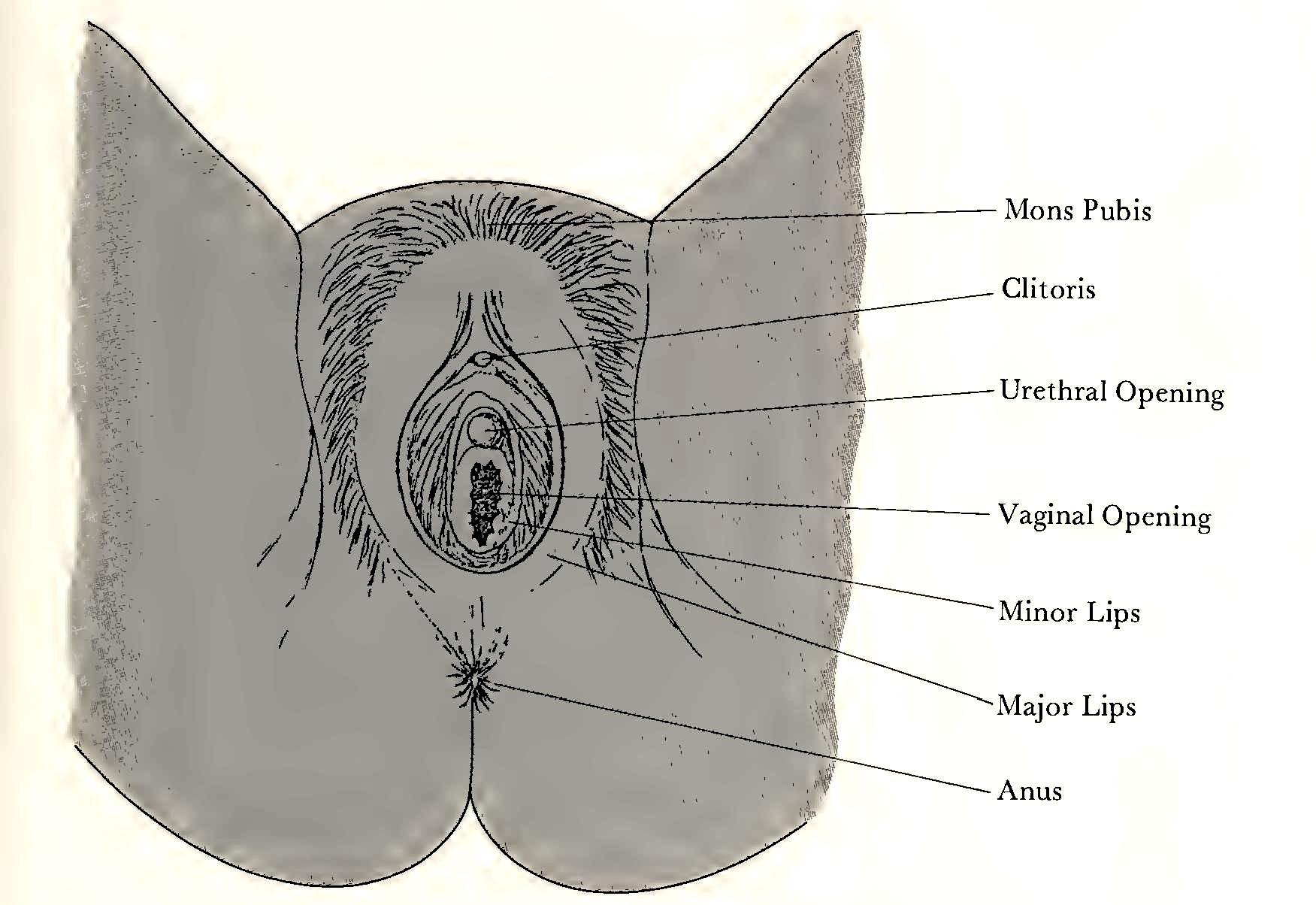
Running back from the tnons pubis and blending into the tissues in front of the anus are the major lips, two loose folds of skin whose outer surfaces also grow hair during puberty. The inner surfaces are smooth and hairless. The size and color of these labia vary with individuals and with age and parity. The minor lips are thinner and hairless and lie within the major lips, where they enclose the clitoris, the urethral opening, and the vaginal opening, as well as the duct endings of Bartholin’s glands. They come together in a single fold over the clitoris, forming the prepuce, or hood, of the clitoris.
The clitoris is unique in the human body in that its sole function is sexual. It is homologous to the penis, although the penis also contains the urethra through which pass urine and semen. In women, the urethra is a separate duct entirely. The clitoris consists of the glans, or tip, the shaft, and the crura, “legs”, which attach it internally to the pelvic bone. The glans is the only part of the clitoris which is visible. It projects slightly from under the prepuce or hood, and it may be viewed with a mirror by parting the minor lips. Richly endowed with nerves, the clitoris is the most sexually sensitive part of the female body. Masturbation is more likely to involve areas over or around the clitoris than in the vagina. It was not an uncommon practice in Victorian times to excise the clitoris of young girls to prevent masturbation (Sherfey, 1972). This operation, a clitoridectomy, is rare today except as a radical procedure for cancer.
The urethral opening is the end of the urethra, the tube which carries urine from the urinary bladder. It is unrelated to the sexual reproductive system.
The vaginal opening or introitus is much larger than the urethral orifice, and is easily seen by parting the minor lips. This opening may be partially covered, or bridged, in young girls by the hymen,[27] a thin membrane which has no particular function but around which has accrued considerable mythical and psychological significance. Though the size and shape of the hymen varies, it has an opening which permits the passage of menstrual blood and even the use of a tampon. An erect penis is usually too large to be admitted past the hymen without tearing it, a point which has given the hymen its particular niche in sexual folklore. As a consequence, many young women experience slight pain and bleeding when the hymen is torn during their first intercourse. This “evidence” of virginity has been highly prized in many socieites. However, the intact hymen is not a definitive sign of virginity, as hymenal ruptures can occur during normal childhood activities.
Bartholin’s glands open between the edge of the hymen and the minor lips. While they secrete a scanty amount of fluid during sexual stimulation, the major source of vaginal lubrication is the wall of the vagina.
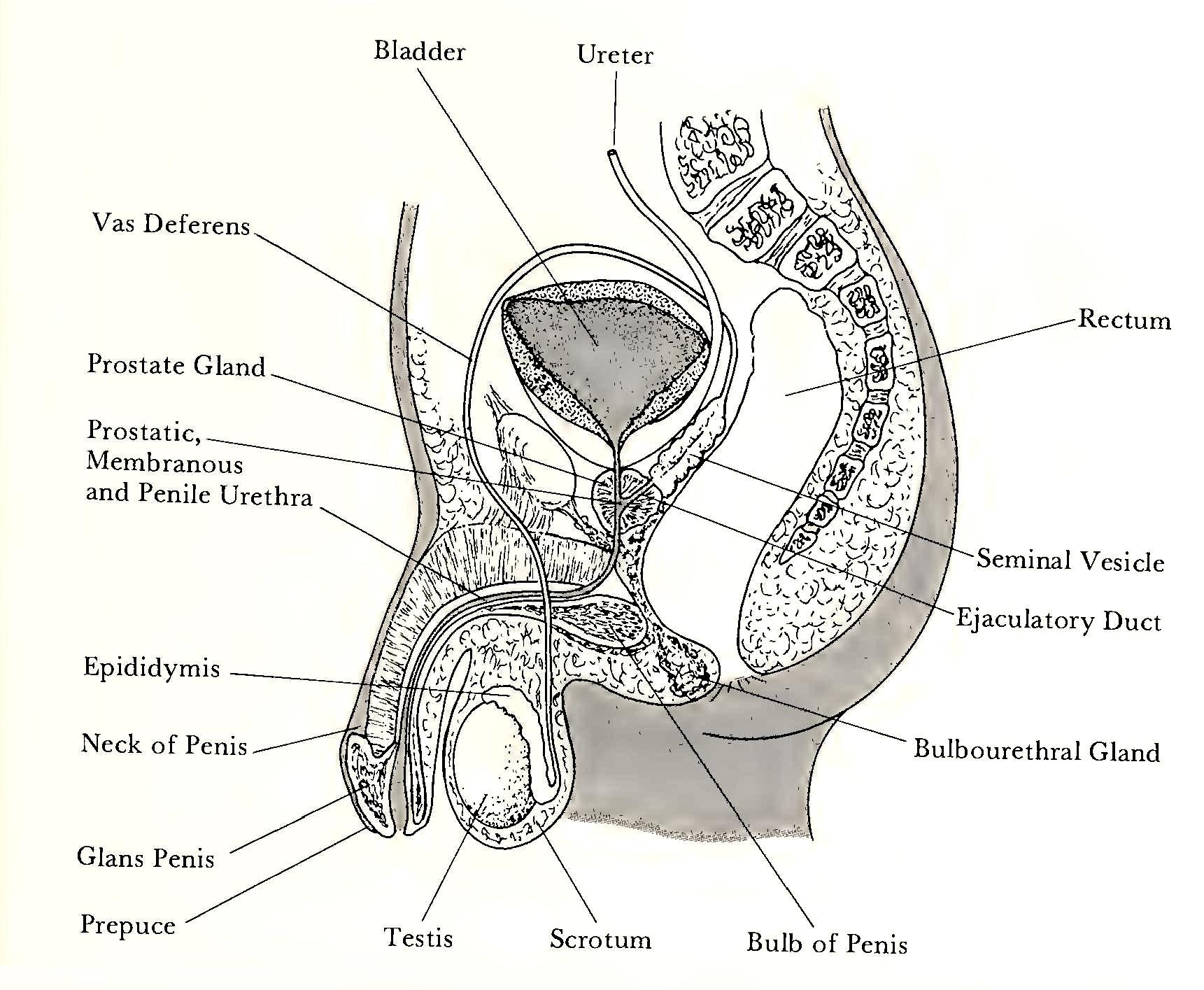
A detailed description of the male sexual reproductive system is beyond our scope. However, a diagram of the organs and structures is presented in Figure 7.2 for reference.
Internal reproductive system
The internal reproductive organs include the ovaries, the two Fallopian tubes or oviducts, the uterus, and the vagina (Fig. 7.3).
The ovaries lie on either side of the uterus to which they are attached by ligaments. They have two major functions: the production of ova, and the manufacture of estrogen and progesterone, the female sex hormones.
The female child at birth has about four hundred thousand immature ova in her ovaries. During puberty, when the ovarian cycle begins, some of the ova begin to mature, and subsequently each month one ovum ruptures the thin wall of its follicle and leaves the ovary. The ovum is captured by the ovarian end of the Fallopian tube. The tubes are not connected to the ovaries but have projections which appear to close about the ovary during ovulation.
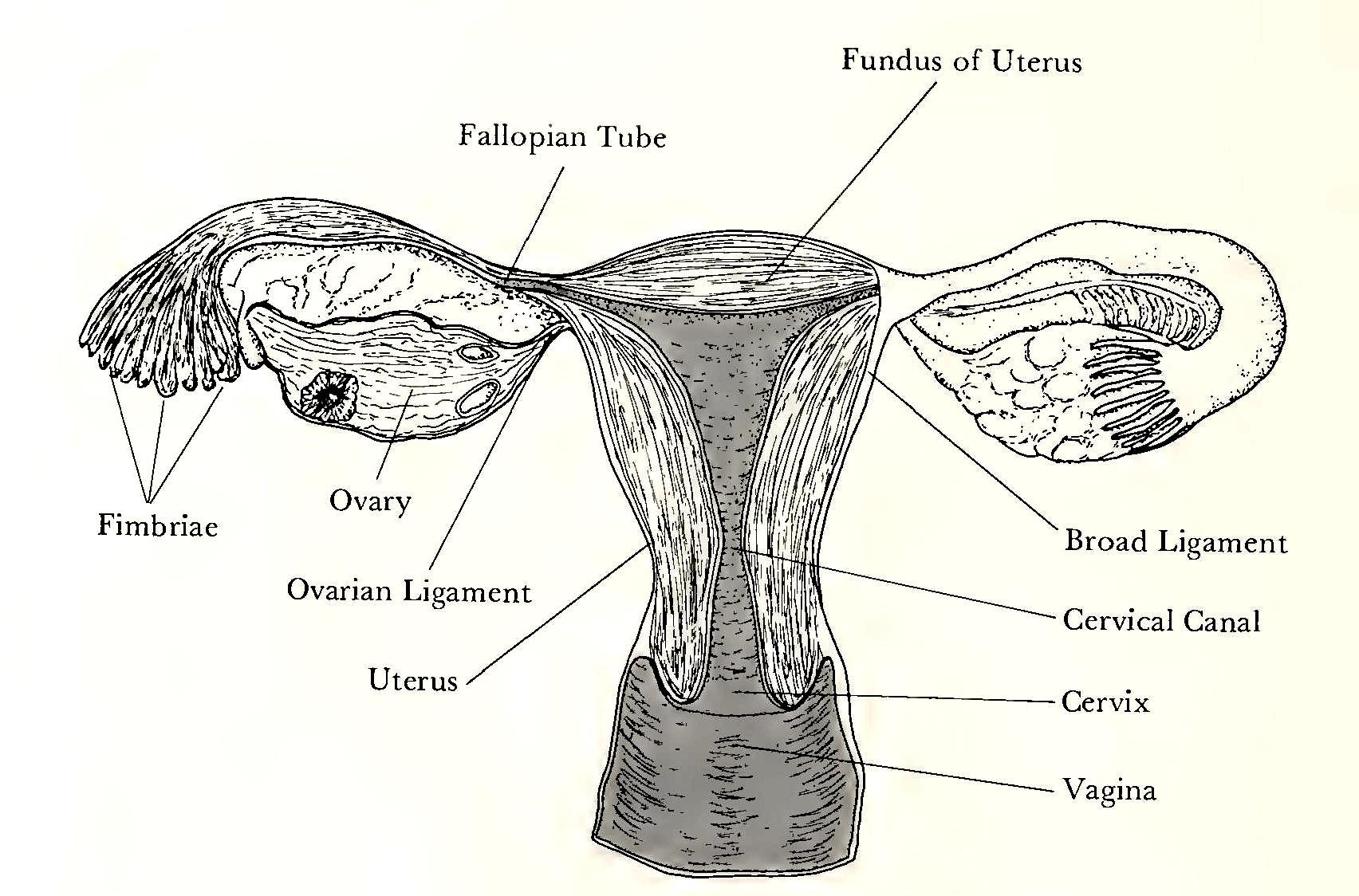
The ovum is moved through the tube by hairlike cilia. If it meets spermatozoa, it may become fertilized, subsequently moving on through the tube and into the uterus, where it either implants if fertile, or is flushed out during menstruation.
The uterus is about three inches long, and is normally held in place by ligaments and tipped forward, its cervix or neck protruding into the vagina. It is very muscular and elastic, expanding greatly during pregnancy. Its function is to shelter and to nourish the developing fetus.
Of all the internal structures, the vagina is the most involved in sexuality. It receives the penis and its deposit of semen. It serves also as the tract through which pass the menstrual blood and the baby at birth. Slanting downward and forward, it is about four inches long and is usually a collapsed tube. Its walls are muscular and are lined with a mucous skin similar to the inside of the mouth. The vagina itself is rather poorly equipped with nerve endings, and thus is relatively insensitive, especially its upper two-thirds. The area surrounding the introitus is, however, very sensitive.
The size and condition of the vagina have been the subject of evaluative appraisal and commentary in the popular culture. Since the vagina of the adult female can expand to permit the passage of a baby, it can accommodate the largest penis; thus no mature vagina is too small for sexual intercourse. It is possible that a muscular spasm, vaginismus, will prevent penetration in a tense and anxious woman. Such an event is psychogenic in nature and unrelated to the size of the penis or the vagina. In the premenopausal woman, the vagina develops its own lubrication when she is sexually excited. After menopause, the walls of the vagina become more delicate and thin, and lose their lubrication efficiency. This condition results from the gradual cessation of estrogen production by the ovaries and can be treated by exogenous lubrication or by medically prescribed creams containing estrogen. The vaginal opening may become larger and looser after childbirth. However, the contraction of the opening is to some extent under the voluntary control of the woman. That is, she can tighten or relax it at will, much as one shuts off the flow of urine. Further, the muscles controlling this phenomenon can be developed by exercises, and such exercise has been shown to be related to the development of orgasmic potency (Masters and Johnson, 1970).
Physiology of Sexual Response
We now move to a consideration of the physiological processes of the woman’s body during sexual experience. For much of what follows we are indebted to the nonpareil studies of Masters and Johnson (1966).
Sexual response may be elicited by a wide variety of stimuli, and stimuli which may be arousing to some individuals may be neutral or aversive to others. As the individual matures, her responses become selective and are likely to be elicited by direct stimulation of parts of the body and by erotic situations. Though arousal can involve all the sensory modalities, touch is probably the most important in women, followed by vision and fantasy.
Certain areas of the body thought to be especially sensitive to sexual arousal are called erogenous zones. In women these include the clitoris, the minor lips, the breasts, the mouth, and the inner thighs. However, almost any area of the body can have erotic potential since individual preferences differ. Probably most important is a sensitivity for the other’s wishes and preferences.
The observations of Masters and Johnson led to a description of the sexual response cycle in both sexes which include four phases: excitation, plateau, orgasm, and resolution. Reactions of the sex organs and other body reactions during each of these are summarized in tables 7.1 and 7.2. Two points should be emphasized regarding these data. First, the sequences and timing of reactions are generalizations based upon observations of a large sample; individual variations from these data are to be expected. For example, many sexual experiences do not culminate in orgasm, or an individual may return from near-orgasm to plateau several times in one cycle. A cycle may be as brief as a few minutes or last for hours. Second, the phases are not discrete, except perhaps for the orgasm; plateau, for example, is an extension of excitement during which the maintenance of sexual tension leads to orgasm.
Several characteristic features develop during the female cycle. The first sign of excitement is the appearance of vaginal fluid, which becomes more copious as the cycle progresses. This exudate actually comes through the vaginal walls owing to the vasocongestion which develops in the pelvic area. The congestion, which is an accumulation of blood and fluids, pushes fluids into the tissues, and results in the “wetness” which lubricates the vagina. This pelvic vasocongestion is the single most important factor underlying the female sexual response cycle.
In the excitement phase, the upper two-thirds of the vagina begin to balloon out, and as the phase is prolonged the cervix and uterus lift away from their usual position. Further, the lower vagina and labia begin to thicken as the tissues become engorged, and, in the plateau stage, this part of the vagina develops the orgasmic platform, the congested walls in which the rhythmic contractions of orgasm are most manifest.
Table 7.1 Reactions of sex organs during sexual response cycle{5}
| Male | Female | |
| Excitement phase | ||
|
Penile erection Elevation of scrotum Testicular size increase |
Vaginal lubrication Thickening of vaginal wall Ballooning of top % of vagina Clitoral tumescence |
|
| Plateau phase | ||
|
Cowper’s gland secretes Testicular tumescence Full testicular elevation |
Orgasmic platform develops Uterine and cervical elevation “Sex-skin” coloration Bartholin’s gland secretes |
|
| Orgasmic phase | ||
|
Contraction of vas deferens, seminal vesicles, ejaculatory duct, and prostate Contractions of penile urethra, 5–8 times at 0.8-second intervals |
Uterus contracts from fundus down Contractions of orgasmic platform 8–18 times at 0.8-second intervals Rectal and urethral sphincter contracts for some subjects |
|
| Resolution phase | ||
|
Loss of pelvic vasocongestion Loss of erection (may be entire or partial; some subjects capable of continued intercourse) |
May return to orgasm Slow loss of pelvic vaso-congestion and orgasmic platform Return of clitoris to normal position |
Table 7.2 Body responses during the sexual cycle{6}
| Male | Female | |
| Excitement phase | ||
| Nipple erection |
Nipple erection Sex flush Plateau phase |
|
|
Sex hush Skeletal muscle tension Hyperventilation Rapid heartbeat |
Skeletal muscle tension Hyperventilation Rapid heartbeat Orgasmic phase |
|
|
Specific muscle contractions Hyperventilation Rapid heartbeat |
Specific muscle contraction Hyperventilation Rapid heartbeat Resolution phase |
|
| Perspiration Hyperventilation Decreasing heartbeat | Perspiration Hyperventilation Decreasing heartbeat |
The glans and shaft of the clitoris also become engorged under stimulation. During the plateau stage shortly before orgasm the shaft of the clitoris increases in diameter and decreases in length, to such an extent that the clitoris retracts under the hood, and its glans is no longer visible or in direct contact with any stimulating agent. Penile thrusting, however, exercises a “pulling” effect on the hood, moving it in such a way that the stimulation of the clitoris continues indirectly. Most women find direct stimulation of the clitoris undesirable owing to its extreme sensitivity.
In general, women reach the orgasmic stage of arousal more slowly than men do because greater pelvic congestion is necessary prior to orgasm. Ina heterosexual situation the male must be willing and able to continue to stimulate her until she reaches orgasm.
The orgasm is a neuromuscular discharge which occurs with appropriate stimulation and massive buildup of pelvic vasocongestion. It is characterized in women by a sequence of rhythmic contractions of the orgasmic platform, of the uterus, and in some women, of the rectal and urethral sphincters. These contractions, timed at about 0.8-second intervals, may vary in number and in intensity for different women and for different experiences.
The difference between the male and female resolution phases accounts for some women’s ability to experience several orgasms during the course of one experience. The male normally has only one.[28] Following orgasm, the clitoris emerges from its retracted position, and begins to lose its tumescence, or erection. The orgasmic platform also begins to subside. Decongestion of the female pelvic structures proceeds at a much slower rate than does detumescence of the penis which rapidly loses its erection after ejaculation. Vasocongestion underlies the capacity for orgasm, so as long as this condition exists, the female may continue to experience multiple orgasms. If the woman does not have an orgasm after prolonged stimulation, the congestion may be a source of discomfort for several hours.
Factors relating to orgasm
Several physiological factors affect the experience of orgasm. The most important is stimulation. Prolonged physical stimulation of the labial and clitoral area is necessary for many women to reach orgasm. Following orgasm, further stimulation may result in prolonging the pelvic vasocongestion, making more orgasms possible.[29]
Masters and Johnson found that most women in their study who were multiorgasmic would be satisfied with three to five orgasms. Women who had much greater numbers of orgasms in succession usually did so by masturbation or by the use of an electric vibrator. The latter was most productive since the fatigue factor was less important. In general, the number of orgasms and the intensity of the orgasmic experience was highly related to the duration and the efficiency of stimulation regardless of the source.
A second finding was that age and childbearing history are related to orgasmic potency for women. In general, women reach their peak of sexual activity later than most men do. The physiological consequences of pregnancy enhance the orgasmic potential of the woman. In the course of pregnancy an elaboration of the system of blood vessels supplying the pelvic area occurs, and this system continues to be available after the woman has given birth. Consequently, the capability for vasocongestion increases, thus increasing the potential for orgasm.
Although the findings are sometimes contradictory, the weight of evidence indicates that the sex drive in women is greater during the luteal or premenstrual phase of the cycle. This finding persists in spite of evidence that most experience heightened feelings of wellbeing during the ovulatory phase when the estrogen level is highest, and that a majority report some symptomatology characteristic of the premenstrual period during the luteal phase (Golub, 1973). The increased interest in sex during this period is a function of the vasocongestion and edema of the lower abdomen and pelvic area prior to the onset of menses (Sherfey, 1972). There is, however, considerable individual variation among women as to when they are most interested in sex, and it is likely that situational factors contribute more to this variability than phases of the menstrual cycle do.
Theories of orgasm
Freud proposed two types of female orgasm, the clitoral and the vaginal. The clitoral orgasm, resulting from stimulation of the clitoral area as commonly practiced in childhood masturbation, would give way, Freud thought, to the vaginal orgasm, which characterized the sexually mature woman. If this shift did not occur, the woman was sexually immature and technically frigid. The notion that women experience two kinds of orgasm has persisted until quite recently. For example, a recent study of twenty-seven gynecology textbooks revealed that of the four that indexed orgasm, three said that the vaginal orgasm was characteristic of the mature woman (Scully and Bart, 1973). An essay on “The Clitorid Woman” referred to her as the perfect sexual partner, passionate and conforming, but said that these traits “do not necessarily give her the vaginal orgasm which is the ultimate, and she may even be frigid” (Meyer, 1966).
The studies of Masters and Johnson led them to conclude that physiologically there is only one type of orgasm. The physiology of the orgasm triggered by a neuromuscular discharge and including rhythmic contractions of the orgasmic platform and related pelvic structures is always the same regardless of which parts of the body are being stimulated or who the partner is. Orgasmic experiences can vary greatly, depending upon a host of factors. But these differences are psychological. The physiological basis remains the same.
An extensive investigation of the anatomical and physiological bases of erotic responses in the female corroborated the single-type theory of orgasm. Because of the extreme sensitivity of the clitoral glans and the relative insensitivity of the vagina, penile or other intravaginal stimulation affects the clitoris, the minor lips, and the lower vagina as an inseparable functional unit with the clitoral glans being the indispensable initiator of the orgasmic reaction. It is a physical impossibility to separate the clitoral from the vaginal orgasms as demanded by psychoanalytic theory (Sherfey, 1972).
The issue continues to be debated, however. Another theory suggests that the vaginal contractions, an essential component of orgasm according to Masters and Johnson, are not necessarily present in all orgasms. A triple model of orgasmic experience has been presented. The first is the “vulval” orgasm, the kind observed by Masters and Johnson. The second is the “uterine” orgasm, characterized by a gasping type of breathing followed by a forceful exhalation. The result, as in the first type, is sexual gratification. This kind of orgasm is brought about by repetitive displacement of the uterus owing to the physical impact of the penis causing it to stimulate the peritoneum, the tissue covering the abdominal organs. The third type is a blend of the first two (Singer and Singer, 1972).
Another theory of the female orgasm suggested that some women are vaginally oriented and some are clitorally oriented. While the clitoral orgasm resembles the kind described by Masters and Johnson, the vaginal orgasm, on the other hand, seems to be more like Helene Deutsch’s description of the ideal orgasm of the mature woman: subjectively, a happy, warm, contented feeling, without the convulsive quality of the clitoral orgasm (Fisher, 1973).
The fact that agreement has not been reached on the question of what constitutes an orgasm exemplifies a certain elusive quality surrounding many aspects of female sexuality. Regarding orgasm, the problem lies primarily in the differing subjective reports of women as they describe the experience. Since women have no ejaculation, which signals orgasm in the male, it is not possible to know on a descriptive level whether two women are describing the same physiological event when they describe their orgasms. Some women describe very satisfying orgasms which do not include vaginal contractions. Exactly what these are at a physiological level is not known.
The view which has the strongest empirical base of support is that of Masters and Johnson, whose single-type theory of female orgasm is based upon direct observation of the physiological responses of sexually stimulated females. Furthermore, the subjective reports of the women in their study taken in interviews immediately following the orgasmic experience are consistent with Masters and Johnson’s objective description of the physiological events. From reports of 487 women, they were able to describe three stages of the orgasmic process.
The first stage, the onset of orgasm, is identified with a sensation of suspension or stoppage. At the same time or immediately after, there is an intense sensual awareness in the clitoral area which radiates into the pelvis. Paralleling this is a loss in sensory acuity; the compelling quality of the imminent event diminishes awareness of everything else.
The second stage, a sensation of suffusing warmth beginning in the pelvic area and spreading throughout the body, was experienced by almost all the women.
By the third stage, the women consistently described a feeling of involuntary contraction in the vagina followed by a throbbing sensation in the pelvis, sometimes spreading to the whole body and becoming combined with a sense of the pulse or heartbeat. This stage of the orgasm as reported by the women was correlated with the contractions of the orgasmic platform as objectively observed by the researchers.
Proponents of theories which propose two or more kinds of orgasm might argue that Masters and Johnson defined orgasms as only those events characterized by contractions of the vaginal barrel. In that case, the subjective reports of the women who experienced that type of orgasm would of course tally with the recorded physiological data. Other culminations of the response cycle which might be quite satisfying and conclusive as a sexual event to some women would not fit the “contraction” definition, and thus would not be called orgasm. If the orgasm is qualitatively different from the earlier stages of the cycle, however, one would expect physiological changes to underlie the difference. So far, the other kinds of orgasms described in the literature have not been shown to have physiological correlates.
Sexual Behavior
The term “sexual behavior” is deceptively simple. As many psychologists understand it, behavior is what one does, those acts that are observable, in contrast to processes that are not observable, such as mood states, thoughts, and feelings. Sexual behavior is behavior that is related to the arousal and gratification of sexual feelings. Narrowly defined, it means the activity done by people to achieve orgasm. This simple definition has problems because an almost infinite variety of behavior can be potentially sexually stimulating, and a great deal of behavior that is clearly sexual does not culminate in orgasm. Most of the research on human sexual behavior has restricted the focus of investigation to a few selected behaviors that account for most of the ways the humans reach orgasm. For example, Kinsey collected data in six categories of behavior; heterosexual intercourse, heterosexual petting, homosexual relations, masturbation, nocturnal sex dreams, and sexual contact with animals. A later study by the Playboy Foundation included those areas plus oral-genital sex, anal intercourse, sadism, and masochism (Hunt, 1974). These last four can be subsumed, of course, under either hetero- or homosexual behavior. The discussion here will be much more limited.
Development of sexuality
The earliest phase of sexual development begins soon after birth in the context of the close physical contact between mother and infant. The sensory experiences the baby has of being held, cuddled, rocked, and nursed begin the gradual evolution toward feelings of affection, attachment, and desire for intimacy with others. Soon this repertoire is expanded to include contact with soft blankets and toys to which the baby may become attached. Comfort-seeking, selfsoothing behaviors, such as thumb-sucking and rhythmic rocking, are employed by many babies, especially if they are feeling stressed or sleepy. All these behaviors, involving sensory stimulation by self or others, are rudimentary rehearsals for the eroticism of adult sexuality (Higham, 1980).
The biological capability to experience sexual arousal and to reach orgasm is present in infants, and it is widely recognized that at least some infants under one or two years do exhibit behavior that is clearly sexual in nature. Kinsey described what appeared to be sexual activity culminating in orgasm for both sexes very early in life (1948; 1953). While we cannot know what the subjective experience of such activity is in the preverbal child, the physical signs are the same as those exhibited by adults, including bringing the genitals in contact with an object, such as a doll or pillow, rhythmic thrusting movements of the pelvis, rapid breathing, increase in body tension, loss of sensory acuity, and sudden release of tension followed by relaxation. While the emergence of such sexual behavior occurs at variable times, with infant orgasm being infrequently reported by parents who may overlook evidence of sexuality, there is no reason to doubt its pervasiveness in the very young.
Whether sex differences exist in infant sexuality or even in observable behavior that appears to be sexual is not known. Clearly reliable data would be difficult to obtain. Male infants have erections frequently beginning soon after birth, but whether these have any erotic significance is questionable. Although erections are the most visible sign of sexual arousal in older males, their appearance in very young males is probably reflexive, that is, occurring independently of higher brain centers that mediate thought and feelings. Kinsey believed, however, that a majority of boys were capable of orgasm by age four. No comparable estimate was made for girls, though Kinsey included in his study of sexual behavior in females a graphic account, provided by a mother, of her three-year-old daughter’s masturbation to orgasm (1953, pp. 104–5).
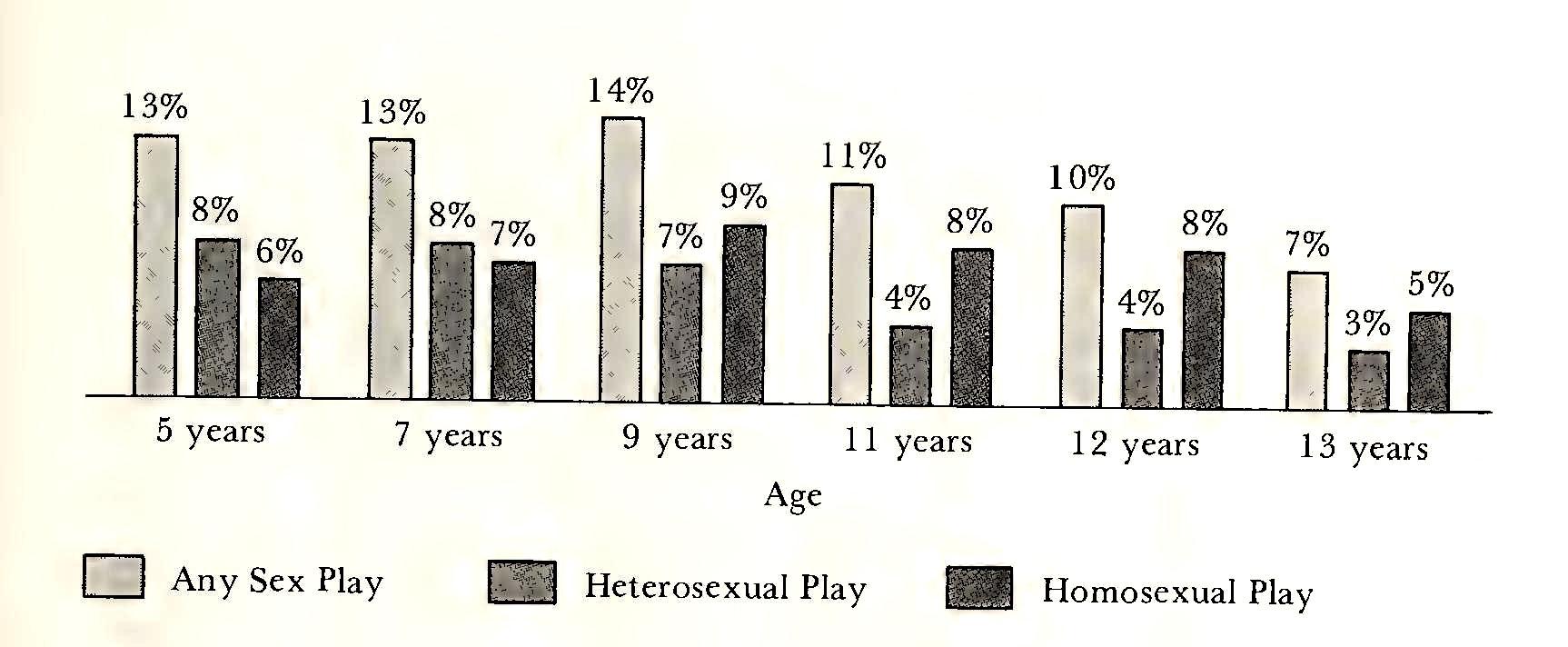
Sex play and genital exploration are very common in children after the age of two or three. Kinsey found an interesting sex difference in the incidence of sociosexual play as contrasted to self-masturbation in children aged five to thirteen. As figures 7.4 and 7.5 show, girls were more likely to be engaging in sex play with others at age five, and maintained a fairly constant level of such activity until age nine, when the percentage begins to decline. The percentage of boys engaging in sociosexual play increased fourfold from age five to age twelve, when it peaked at 39 percent compared to 10 percent for girls of the same age. Obviously, these data should be viewed with some caution, as they are primarily based on the recollections of adult subjects. Further, both the memory of the behavior and the behavior itself are subject to cultural pressures, affecting adults’ perceptions of themselves as children, as well as their childhood perceptions of their own behavior in a social milieu.
The most common sociosexual activity for both sexes in childhood is the exhibiting and handling of genitals. Most of this in prepubertal years is homosexual in context, although 30 percent of the women in Kinsey’s sample and 40 percent of the men recalled heterosexual play before puberty. Homosexual play was unlikely to persist after puberty, though Kinsey found that the adult homosexuals in his sample had discovered their sex preference in the course of childhood homosexual play.
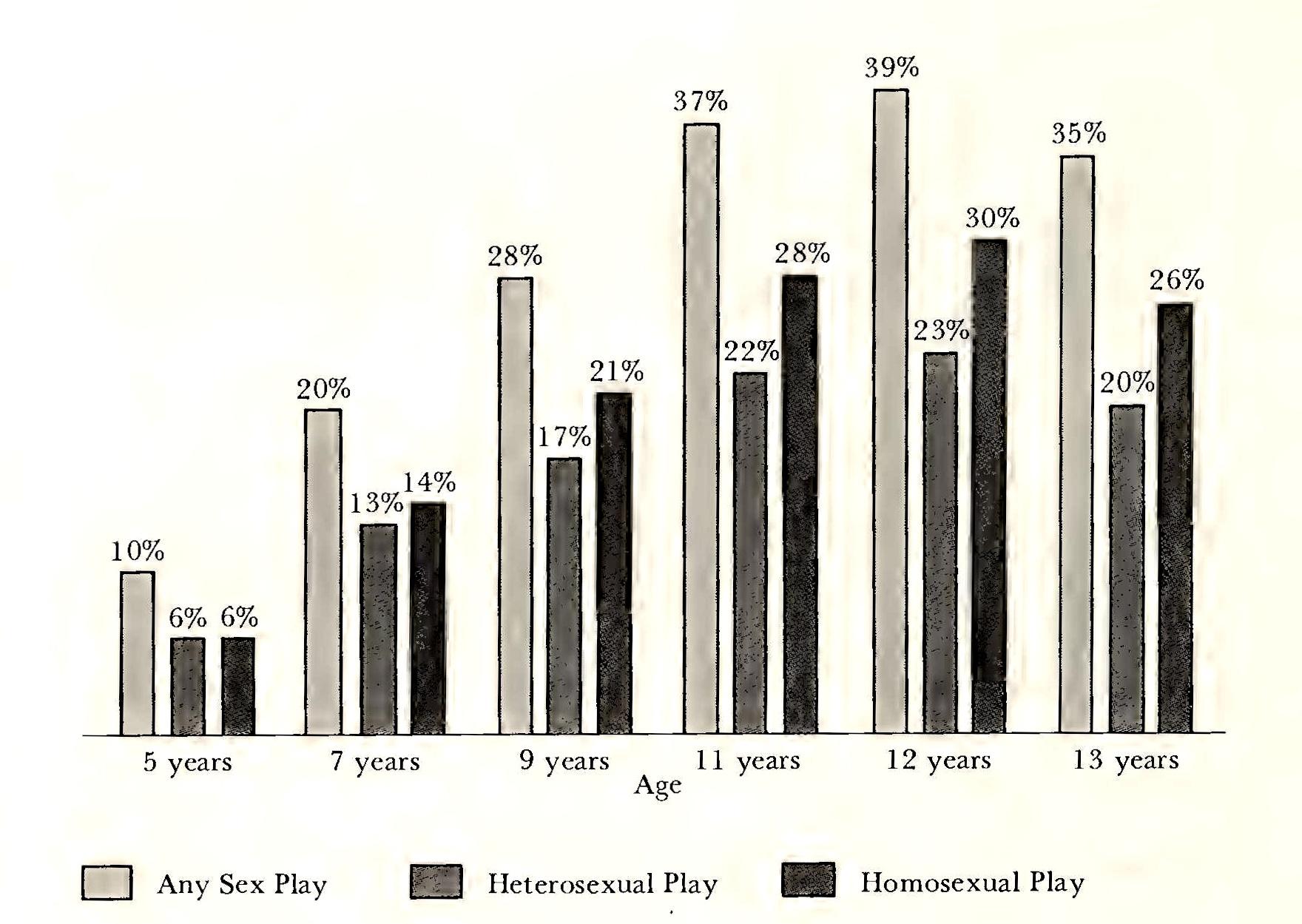
Although infants and young children often discover the pleasures of genital stimulation and engage in masturbatory activity on a sporadic, nonsystematic basis, deliberate masturbation becomes prevalent in prepuberty or the early pubertal years. Kinsey’s data indicated that a higher percent of girls than boys between the ages of five to ten had masturbated to orgasm. After that age there was a slow but steady increase in the percent of females who had ever masturbated, reaching a peak of 62 percent by age forty-five. Women continued to discover and to practice masturbation well into middle age. By contrast, the percent of males who had masturbated increased rapidly after age ten or twelve, reaching a peak at age twenty when 92 percent of males had masturbated to orgasm. The salience of masturbation for females in the Kinsey sample was indicated by the fact that 85 percent had reached their first orgasm through masturbation, compared to 70 percent of the males.
The Playboy survey provides some interesting comparisons with Kinsey’s data on masturbation. For the total samples of males and females over eighteen, 93 and 63 percent respectively reported that they had ever masturbated to orgasm, an increase of only 1 percent over the Kinsey samples. However, the incidence of masturbation to orgasm by the age of thirteen was much higher for both sexes than Kinsey found, as shown in Figure 7.6.
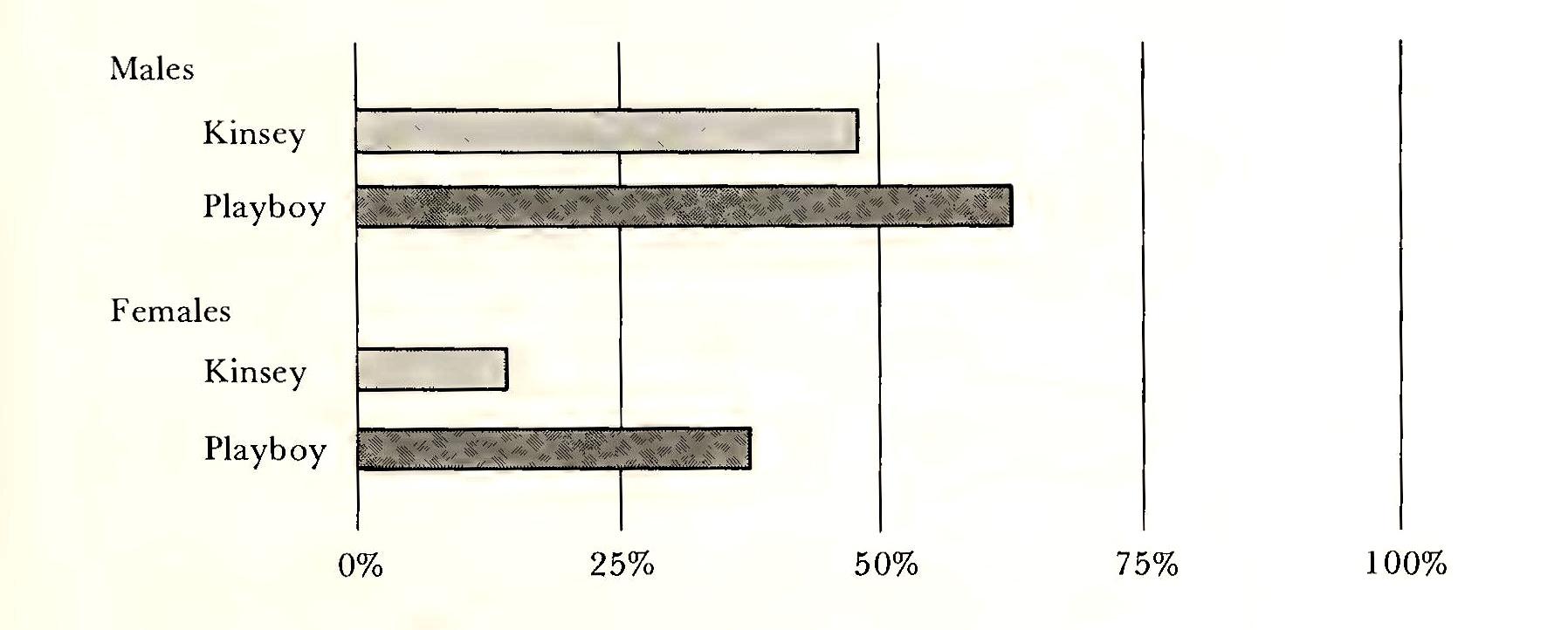
How real this increase in masturbation to orgasm is for children under thirteen is problematic. Again, the figures are based on adults’ memories of their early behavior, and while they may represent a genuine shift toward an earlier breaking through of parental and social barriers of disapproval, they may also reflect in part a relaxation of the taboos against admitting such behavior, or even an enhancement of the self-image through such admission (Hunt, 1974).
Puberty greatly increases the salience for both girls and boys of sociosexual activity. The emergence of the secondary sex characteristics makes the physical differentiation of the sexes more visible. The maturation of the sexual potential of the body, as well as sociocultural pressures and expectations, brings about increased libidinal interest in the other sex. At the same time, however, sanctions, especially for girls, are imposed on sexual activity. Romantic attachments, falling in love, dating, going steady, all become features of the adolescent’s life. Today that syndrome is likely to include the experience of sexual intercourse as well. Data from two national surveys reveal an increase of 30 percent in the prevalence of intercourse among unmarried fifteen- to nineteen-year old women between 1971 and 1976. Sexual activity increased among both black and white women, with a greater increase for whites. By age nineteen, 84 percent of black and 49 percent of white unmarried women had experienced intercourse in 1976, compared to 79 percent of blacks and 41 percent of whites in 1971 (Shah and Zelnik, 1980).
The sexual revolution?
The Playboy Foundation survey of adult sexual behavior in the United States population makes it possible to compare later data with the Kinsey data and to examine changes in premarital, marital, and extra- or post-marital sexual behavior which have occurred in the last two decades. While the general shift is toward a higher incidence of all kinds of heterosexual activity and more permissive attitudes toward homosexuality and variety in the sexual act, the change has been more dramatic among women than men.
Table 7.3 Percent of respondents who ever had premarital coitus, by age{7} (Total Married Sample)
| Percent | Under 25 | 25–34 | 35–44 | 45–54 | 55 and up |
| Males | 95 | 92 | 86 | 89 | 84 |
| Females | 81 | 65 | 41 | 36 | 31 |
Probably the most significant change is in the reported incidence of premarital coitus. The increase, especially among females, from the older to the younger age groups, had accelerated within the last fifteen years (see Table 7.3).
By contrast, in the Kinsey sample, only a third of the women had had premarital coitus by age twenty-five, consistent with the Playboy Endings for the forty-five-fifty-four age groups. The increase was striking enough to lead to the conclusion that in another five or ten years, premarital coitus will be an all but universal experience for the young in our society (Hunt, 1974).
While sex before marriage seems to have become the norm, it has not become more casual for those under twenty-five, nor are the young more promiscuous, according to the more recent survey. Of those females who had had premarital coitus, both the Kinsey and Playboy surveys found that approximately half had had only one partner—the man they expected to marry. Both older and younger males in the Playboy sample had had an average of six premarital partners. Kinsey did not give data on premarital partners of males.
Sexual liberation has affected the marital relations of people of all ages in the United States. At every age group, the frequency of coitus has increased from the Kinsey to the Playboy survey. (Table 7.4).
Nine-tenths of the wives in the Playboy survey said that their coital experiences in the past year had been generally or very pleasurable. Among women who had been married fifteen years, the number who always or nearly always had orgasm increased from 45 percent (Kinsey) to 53 percent (Playboy), while the number who seldom or never did so dropped from 28 percent (Kinsey) to 15 percent (Playboy).
One of the most striking findings in the Playboy survey was the increase in duration of coitus among married couples. Kinsey had estimated that about three-quarters of married males reached orgasm in two minutes or less after intromission. Today, according to the Playboy data, the median duration is about ten minutes for all couples, ranging from thirteen minutes for the youngest age group to ten for those fifty-five and over.
Table 7.4 Comparison of Kinsey and Playboy respondents on frequency of marital intercourse: median weekly frequency of marital intercourse{8}
|
1938–49 (adaptedfrom Kinsey) |
1972 (Playboy survey) | ||
| Age | Frequency | Age | Frequency |
| 16–25 | 2.5 | 18–24 | 3.0 |
| 26–35 | 2.0 | 25–34 | 2.5 |
| 36–45 | 1.5 | 35–44 | 2.0 |
| 46–55 | .9 | 45–54 | 1.0 |
| 56–60 | .5 | 55 and | up 1.0 |
The Playboy survey also found a strong correlation between marital success and sexual pleasure. The large majority who rated their marriages very close also found coitus very pleasurable, whereas three out of five women and two out of five men who rated their marriages not close found marital coitus not pleasant.
The Playboy study also noted that the increase in frequency and satisfaction among married couples was caused by freer attitudes, better birth-control methods, and the influx of information relevant to obtaining sexual satisfaction. The women’s liberation movement is credited, also, with getting rid of the image of women as passive and uninterested in sex.
Sexual liberation seems to have had the least impact on the incidence of extramarital relations. The only groups in which more subjects had had at least one extramarital experience were the under-twenty-five married and divorced, both males and females. Males in this category increased from 27 to 32 percent, and females from 8 to 24 percent. Paralleling the premarital statistics, the rate of increase is much greater for females than for males, suggesting that liberated attitudes and better contraception have made more of a difference for women than for men. The figures on mate-swapping and group sex, which Kinsey did not collect, indicate that only about 2 percent had ever engaged in mate swapping, and 2 percent of men and less than one percent of women had ever had sex with other partners in the presence of the spouse.
Divorced women in the Playboy sample were much more active than those in Kinsey’s sample. The median frequency for the sexually active was almost twice a week, almost as high as for divorced men and four times higher than the divorcees in the Kinsey sample. Also, only a tenth of the divorced women in the Playboy sample were sexually inactive, compared to a third of Kinsey’s younger postmarital group and the majority of those older than the mid-forties.
Although the Playboy study remains the most recent attempt to replicate Kinsey’s work, a few large-scale questionnaire-type studies on the sexual behavior of American women have appeared in the past few years (Hite, 1976; Tavris and Sadd, 1977; Wolfe, 1980). Though none of these is representative of the general population, tending rather to be biased toward younger, better educated, more affluent groups, they do provide interesting data on that part of the population. An example is a survey of the sex lives of its readers conducted by Cosmopolitan magazine (Wolfe, 1980). Based on over 100,000 responses, the study revealed sexual practices and attitudes of young, employed, urban women all over the United States.
About 20 percent of this group had their first sexual experience before the age of fifteen, compared to 3 percent of Kinsey’s sample. Most reported that the first experience, regardless of age, ranged from disappointing to awful: “... the first few days after my boyfriend and I made love, I thought, Maybe I’ll never do it again. But I did—twice more—and I feel a little better about it, but in a way I’m still asking myself, Is this what all the fuss is about?” (p. 255). Only 10 percent had an orgasm that first time. Two-thirds of the women had had from five to twenty-five lovers, and half the married sample had had at least one affair since marriage. Almost all had masturbated and had sexual fantasies.
In experiencing sex, most of the women wanted foreplay to last up to a half-hour, though few drew the traditional lines between foreplay and intercourse: “... we don’t think of the things we do beforehand as getting ready for intercourse but as pleasures in and of themselves” (p. 257). Though the majority reported the need for some clitoral stimulation in order to reach orgasm, most still preferred the “missionary” position—man on top—to any other. Eighty-five percent participated in oral sex, both fellatio and cunnilingus, though only a few had tried anal sex. Only 2 percent participated in sadomasochistic activities.
As for orgasm, only 1 percent had never experienced it, and half “usually” had an orgasm during intercourse. Among those two-thirds who had multiple orgasms, the majority had two to five in a session.
In general, the women in this study were sexually experienced, uninhibited, and enjoyed their sexual lives. They reported, however, that the new freedom that accompanied the “sexual revolution” had its own problems. Many thought that it had trivialized sex and diminished intimacy, in addition to placing pressure on women to have sex whether they wanted to or not: “The sexual revolution has given men an excuse for avoiding any sort of commitment. They never wanted commitment, and now we’ve let them think we don’t want it either.” “The old rules have been thrown out but the new ones aren’t clear.... The confusion is causing me and all my friends a great deal of unhappiness” (p. 265).
Based on the available data, it does seem that a major shift in sexual mores and behavior has occurred in our society. Whether it is accurate to call this a revolution is dubious. People are experimenting with sex at earlier ages, compared with Kinsey’s data from the 1950s, and the incidence of sexual activity in the premarital period, within the marriage relationship, and among the divorced, has increased substantially. Inhibitions have relaxed, more information is available, and because of advances in birth control methods, the fear of pregnancy is reduced somewhat.
In the meantime, though it may be too early to predict a significant modification in sexual behavior, some commentators have remarked that the sexual revolution is over. Several college campus surveys have reported a renewed interest in virginity as a value, with increased numbers of women identifying themselves as virgins. A longitudinal study over a ten-year period indicated a return to sexual conservatism among undergraduate women at the University of Texas. In 1974, 35 percent reported having sexual intercourse at least once a month. Five years later, the number had increased to 50 percent. But in 1984, the most recent survey showed a drop to 38 percent. It was speculated that the retreat could result from a fear of sexually transmitted diseases, a more conservative campus mood, or an increase in women’s assertiveness in saying no (McLeod, 1984).
Experiencing sex
How do women feel about sex? At the beginning of this chapter we commented on the great variability among women in sexual experience and satisfaction. Later we noted an elusive quality to the available information on the female orgasm. Both these observations are pertinent to the question in that they show why there is no definitive answer. To paraphrase Samuel Johnson, “Which woman? What kind of sex?”
The sexual behavior of women is changing so rapidly that all generalizations about it must be suspect. Earlier writers were quite sure that women had a lower sex drive than men, that their capacity for arousal was lower, that they engaged in sex mostly to satisfy men, and that they could adjust quite comfortably to a life without any sex at all. In view of the recent investigations into the physiology of sex and into sexual behavior showing women’s biological potential and behavioral response in an environmental context, it is evident that any conclusive statements about female sexuality would be premature.
We can, however, consider the variability of sexual experience and some of the factors affecting it. Masturbation, for example, is begun early and practiced regularly by some girls and women. Others never even think of it. Many women enjoy sex greatly and are orgasmic from their first experience. Others grow old without ever having experienced an orgasm. Many nonorgasmic women nonetheless take great pleasure in their sexual relations. Others resent it as one more chore or see it as an exploitation of their bodies.
If we assume that women do not differ greatly in their biological capacity for sexual arousal and orgasm, then we must conclude that the variability in women’s sexual experience is primarily caused by extraneous factors: experience and opportunity, and sociocultural attitudes toward sex.
Several writers agree that an important factor in female eroticism, particularly orgasm, is experience (Bardwick, 1971; Kaplan, 1975; Kinsey, 1953). Simply stated, women can learn to have orgasms. The ability to do so is latent in all females and responds to cultivation. Once a woman achieves arousal to orgasm by any means, masturbation, petting, or intercourse, it should be easier for her to do so again under similar circumstances. As she learns more about the responsiveness of her body, she becomes more adept at stimulating and facilitating it. With practice she becomes less inhibited and less fearful, and more willing to “let go,” to give herself over to the experience. The role of experience is supported by Kinsey’s finding that sexual activity reached its peak in women at about age thirty and continued over the next decade.[30] The Playboy sample showed that, compared to single women, the number of married women who reported that all their sexual intercourse resulted in orgasm was about 20 percent greater. Likewise, the number reporting that none of their sexual intercourse resulted in orgasm was about 10 percent. Since it is reasonable to assume that married women in general have more experience with coitus than single women do, these findings are consistent with the notion that experience is a good teacher.
Sociocultural attitudes toward sex and the body and the extent to which the individual woman has incorporated them into her own attitudes and value system clearly have an effect upon her sexual responsiveness. Leah Schaefer studied the sexual experiences of thirty married, college-educated women in New York City. The recollections of their childhood sexual explorations uniformly included reactions of shame and guilt and need for secrecy. The repressiveness characteristic of the Victorian attitudes discussed earlier pervaded the teachings and admonitions they received about masturbation, petting, and intercourse. Enjoyable sexual experiences before marriage were exceptional, owing to the fear and guilt surrounding them. Even so, twenty-three of the thirty had premarital intercourse. They engaged in their Erst act of coitus not because of sexual desire but because of a wish to lose their virginity, to “get it over with,” or out of curiosity. Only three of this group had orgasm in their Erst coitus. Of the seven who remained virgins until marriage, none had orgasms in their first coitus. While this is evidence for the experience factor discussed above, most of these women also felt a need to “hold back,” a fear of the loss of control which orgasm meant to them, and a continuing feeling of shame and guilt, that something was wrong with what they were doing (Brecher, 1979).
This awareness of the partner and what he thinks of her, and anxiety about his attitudes toward her sexuality also affect the sexual experience. For example, a female student of mine wrote, “The first time I had an orgasm I didn’t know what was happening to me. It was like a series of spasms that 1 couldn’t control ... it just happened. I was very embarrassed. My boyfriend looked at me like I was some kind of a whore. From then on I felt I had to control it.”
Certain attitudes are more typical of unmarried college women who are coitally orgasmic than of those who are not. The orgasmic women had less conflict with parents, especially fathers, and believed that they themselves would be no more restrictive with their daughters than with their sons. They also rated themselves freer of sexual inhibitions, became more aroused from petting, and were more satisfied with their capacity for sexual arousal. They felt that their sex drives were about equal with their partners’, and they were more likely to initiate sexual activity (Shope, 1975).
While the orgasmic women reported more total coital contacts, the numbers in both groups who reported forty-one or more were not very different from each other. Although there may have been an experiential effect, greater weight was given to the attitudinal differences which distinguished the two groups. As one would expect, high levels of arousal and enjoyment characterized the orgasmic group. But three out of four of the nonorgasmic group enjoyed coitus much or very much. Plainly, the coital experience had dimensions of pleasure even in the absence of orgasm.
Willing involvement in the sexual act was much more characteristic of the orgasmic group. Giving in to male pressure was rare for them, in contrast to the nonorgasmic group. This mutuality of interest, along with the previously noted belief in the equality of their sex drive with their partner’s, suggests a certain freedom of action, of autonomous consent in the relationship.
The desire for sexual activity to continue after coitus was typical of the orgasmic group, while only about a fourth of the nonorgasmic group expressed such a wish. Probably different motivations affected the two groups in their responses to this question. Many sexually experienced women can have multiple orgasms. For this reason, the orgasmic women might have wanted to continue their highly pleasurable experience, while the nonorgasmic women who expressed a desire to continue might have felt frustration at the termination of the encounter before their own orgasmic relief has occurred. Those in the orgasmic group who did not express a wish to continue said they were “too tired” after the experience, while those in the nonorgasmic group were more likely to see coitus as an activity to be “gotten over with.”
Focusing on the sexual experience was much more characteristic for the orgasmic group. Most of them were not disturbed by outside noises whereas over half the nonorgasmic group were. Again, the extent to which one can abandon the self, and shut out interference from other sources including the conscience is a correlate of responsiveness in the sexual experience.
Most of the orgasmic women rated themselves as uninhibited in their sexual expression. This probably reflects a global evaluation by the women of their general interest and willingness to participate in sexual activities. That they judged themselves to be uninhibited, however, does not necessarily mean that their freedom from inhibition was a cause of their orgasmic ability. The fact that they were orgasmic could have caused them to see themselves as less inhibited.
Orgasmic women were only half as likely to prefer the man-over-woman position in coitus, compared to the nonorgasmic group. Their general satisfaction with their sexual experience led many of them to report that all coital positions were equally preferable. This suggests a willingness to experiment, and an openness to the possibilities of the experience.
Clinical evidence strongly suggests that women who are typically orgasmic in coitus have certain attitudes that mediate their sexual responsiveness. Such women value their sexuality for its own sake. They are interested and seek actively to satisfy themselves. Sexual interaction in and of itself is positively valued. Many nonorgasmic women who enjoy sexual interaction focus less on the purely sexual aspects of coitus, and are less likely to engage in sex for the sake of sex. I heir reaction is global, to the totality of the situation, to its setting, its timing, its romantic overtones, and to the closeness, warmth, and sharing experienced with the partner. While orgasmic women are likely to appreciate these too, they may be less dependent upon them for their own sexual gratification.
Orgasmic or not, it appears that most women value and enjoy their sexuality and their sexual lives. In The Hite Report, a nationwide study of the sex lives of three thousand women, one of the questions asked was, “Is having sex important to you? What part does it play in your life, and what does it mean to you?” The overwhelming majority of women responded that sex meant a great deal to them. The reason most frequently given was that it was a time of intimacy and closeness with another human being (Hite, 1976). “Sex is beautiful because such a complete contact with another person makes me feel my being is not solely confined to my own body” (p. 283).
Such a finding was reinforced in the results of an informal survey of her readers by popular columnist Ann Landers. Having discerned that sexual activity might have somewhat different meanings for females and males, Ms. Landers posed the question, “Would you be content to be held close and treated tenderly, and forget about ‘the act’?” More than two-thirds of the ninety thousand women who responded said yes, leading one sociologist to comment that some fundamental differences between males and females in the realm of sexuality have been ignored. While the survey was not scientific, the magnitude of the response strengthens the hypothesis that women are more interested in the interpersonal nuances of sexuality, such as emotional closeness, romance, and feelings of belonging, than they are in the physical release of intercourse. Of course, it should be pointed out that the two are not mutually exclusive. Still, it is interesting to note that romance novels, which are not usually sexually explicit, are written for women, while pornography, which is always sexually explicit, is produced for men (Squires, 1985).
Feminism and sexuality
It is important in a chapter on female sexuality to take account of recent trends and issues in feminist discussions of sexuality. As the feminist movement emerged and grew in the late 1960s, the sexual issues within the movement were twofold. The first of these was the support and promotion of women’s claim to be sexual beings in their own right, instead of subordinating their desires and sexual behavior to those of men. This meant that the experience of orgasm was women’s right, and the focus was on empowering women to insist upon that right, thus elevating women’s sexuality to the same status, giving it the same importance, that men’s sexuality had always had.
The second issue was the right to abortion. Abortion was seen not only as women’s right in exercising control over their fertility, but also as legal protection from the consequences of heterosexual intercourse.
As women’s right to pleasure became credible, and abortion became legally available in 1973, the major feminist sexual issue that emerged was an emphasis on women’s rights to sexual pleasure with other women. Radical and lesbian feminists in particular thought that heterosexuality with its socially sanctioned dominance by males for male pleasure, and its historic identity with patriarchy, was closely allied with the oppression of all women. Only by bonding with women in a women-oriented culture that included sexuality could women hope to free themselves from male dominance (for extended discussion of lesbianism, see Chapter 11).
As these earlier goals began to be legitimated, and cultural inhibitions became somewhat less rigid, feminist attention turned to sociosexual practices that are embedded in the heterosexual society, such as pornography, sadomasochism, and the sexual use of children. These practices, they said, glorified the flagrant abuse of power to sanction violence, exploitation, and degradation of women and children.
This critique of patriarchal sexuality was met with strong opposition by other feminists, who saw it as a new kind of moral purism that reflected the antisexual attitudes of earlier times, against which feminism had fought so hard. This group was opposed to what they saw as censorship, implied in the antipornography stance, and favored f reedom to participate in any kind of sexual activities between consenting persons.
This debate, which has included confrontations both in print and in public,[31] has been painful and divisive for the women’s movement. “It is especially unsettling for a movement that has flourished on an ideal of female unity and a dream of a common sexual politics” (Freedman and Thorne, 1984, p. 103).
In an effort to heal the breach, Ann Ferguson (1984) suggested the adoption of a feminist sexual morality that distinguishes between basic, risky, and forbidden sexual practices. Basic feminist practices include both casual and committed sexual love, relationships that are distinguished by negotiation and equalization of the partners in terms of their differences in power in such areas as age, gender, and economics. A practice is risky it if may lead to dominant-subordinate relationships, such as sadomasochism, pornography, prostitution, and nuclear family relations between a male breadwinner and a female housewife. Forbidden sexual practices are those in which dominance and submission are so explicit that they should be illegal. These include rape, incest, domestic violence, and sexual relations between young children and adults.
Feminists have the right to engage in risky practices, said Ferguson, since they would not be proscribed. Presumably, however, one would need to be aware of the potential in these practices for paradigms of dominance and submission to emerge. But inherent in her proposal is the freedom to choose among basic and risky practices without fear of condemnation from other feminists.
Sexuality has become a much-discussed and researched topic in recent years, and a gratifying sex life has become the norm sought after by everyone. Failure to reach this goal is now defined by many as a problem. In this climate, a new discipline has emerged, the study of sexual dysfunctions, and a new therapy has been developed to help people overcome them.
Sexual Dysfunction
Sexual dysfunction is the inability of the individual to function adequately in terms of sexual arousal, orgasm, or specifically coital situations. Until recently the sexual problems of women were subsumed under the general label of “frigidity.” Hardly understood, they were thought to be symptomatic of neurosis or other psychopathology and to require lengthy treatment such as psychoanalysis for the identification and resolution of the underlying problem. Such a traditional approach persisted in spite of the absence of a demonstrated relationship between the treatment and the alleviation of the sexual problem. Rarely were sexual dysfunctions of women treated as problems in and of themselves. Rather, they were seen within the context of the woman’s intrapsychic conflicts or as part of a complex of problems within the marriage relationship. The relative lack of attention to problems of sexual adequacy is attributable to several sources, all applicable to women and some to men as well. First, until recently, the prevailing mores were incompatible with sex research. The level of knowledge about sexual response and behavior was simply inadequate to support effective treatment. Second, cultural taboos prevented open discussion of sexual problems even with physicians and other therapists. Third, women’s sexual needs were not considered to be of major importance to their adjustment and wellbeing, and women themselves were led to think that their submission to the male and identification with his satisfaction were the important components of their own sexuality.
Social changes in mores and values have substantially undermined the last two obstacles, and research has provided an empirical basis for eliminating the first. The major research in this area and development of treatment methods and procedures was done by Masters and Johnson following their earlier studies of human sexual response.
Two contributions by Helen Singer Kaplan are The New Sex Therapy (1974) and Disorders of Sexual Desire (1979). Her approach extends from the work of Masters and Johnson. Kaplan’s work is the primary source for this section.
The sexual dysfunctions of women are of four kinds: inhibited sexual desire, general sexual dysfunction, orgasmic dysfunction, and vaginismus. After describing each of these briefly, we shall consider the etiology, the psychological origins of sexual dysfunctions, and the principles of therapy which are being used to correct them.
Inhibited sexual desire
Inhibited sexual desire (1SD) seems to be the most common of the sexual dysfunctions. Persons suffering from ISD have a persistent and pervasive lack of interest in or desire for sex. While there are no reliable norms for level of libido, it is not difficult to identify pathological variations from the norm. As Kaplan points out, if a thirty-nine-year-old married woman never feels sexual desire, is not attracted to her husband or any other man, and never fantasizes or masturbates, she has an abnormally low appetite for sex. Sometimes ISD is situational, such that the woman may feel no desire at all for her attractive, loving husband, but is “turned on” only by casual sex with strangers.
General sexual dysfunction
General sexual dysfunction is what most people have in mind when they use the word “frigidity.” The woman who is generally nonresponsive describes herself as being devoid of sexual feelings. She experiences little or no erotic pleasure from sexually oriented stimulation. Genital vasocongestion and lubrication, the physiological accompaniment of arousal in the female, develop either minimally or not at all. Women with this type of dysfunction vary in their reaction to coitus. Some consider it a tedious ordeal; others find it frightening or disgusting. A third group can appreciate the positive experiences of physical contact with a loved one even though erotic arousal does not occur.
Primary and secondary types of general sexual dysfunction can be distinguished. The woman with a primary general dysfunction has never been sexually aroused with any partner. The woman with a secondary general dysfunction has been responsive at some time with someone, but is not with her present partner.
Orgasmic dysfunction
Orgasmic dysfunction refers specifically to the inability to experience the orgasmic component of the sexual response cycle. The dysfunction is primary if the woman has never experienced orgasm. It is secondary if she had been orgasmic in the past but no longer is. In addition to this distinction there is another which is dependent upon the circumstances. The dysfunction is absolute if the woman cannot achieve orgasm in coitus or with any other kind of stimulation. It is situational if she can reach orgasm under some circumstances but not others.
The women with orgasmic dysfunction may have a strong sex drive, become readily aroused, and develop vasocongestion and lubrication. It is the orgasm itself, the neuromuscular discharge, which is inhibited. Inability to reach orgasm is the most common and the most quixotic of the sexual dysfunctions. Some women seem to have a very high threshold for the triggering of the neural mechanisms involved in orgasms. That is, they require prolonged, continuous stimulation of the clitoral area before they are “ready.” Such women will clearly be nonorgasmic in a penile-vaginal intercourse situation of a few minutes’ duration. Others readily have orgasms by masturbation or with the use of a vibrator, but cannot in the presence of another person.
Achieving orgasm is not a criterion of sexual competence or normality in women. Nor is orgasmic dysfunction necessarily a symptom of pathology. Orgasm is basically a physical response which occurs under stimulating conditions which are variable for individual women. While almost all women[32] are physically able to have orgasms, many who do not are not unduly disturbed. Many women experience pleasure and gratification in the sex act even in the absence of orgasm (Shope, 1975).
Vaginismus
Vaginismus is a relatively rare condition in which the muscles surrounding the vaginal entrance close tightly whenever any attempt is made to introduce anything into the vagina. Attempts to achieve coitus are painful and frustrating failures, and even physical examinations involving vaginal penetration are impossible without anesthesia. Women with vaginismus are often extremely fearful of coital or other penetration, and develop high levels of anxiety under such circumstances.
Vaginismus is not always associated with sexual inhibition or orgasmic dysfunction. Some women with vaginismus are sexually responsive and orgasmic even though they cannot tolerate coital intercourse. The inability to have coitus still can be a serious problem and can have devastating psychological effects both on the woman and on her partner. The unpleasant consequences of attempting coitus can set up an avoidance reaction in the woman which results in a complete disruption of her sexual adjustment, especially if it is dependent upon a coital relationship.
Etiology of Sexual Dysfunction
A very large number of factors have been implicated as contributors to sexual dysfunctions in women. Physical factors, such as debilitating illness or neurological or endocrinological disorders, can interfere with sexual response, but these account for a very small percentage of female sexual dysfunctions. The great majority are caused by psychological factors (Masters and Johnson, 1970). Many of these causative factors are nonspecific in their effects. That is, they are general factors which can result in any of the sexual dysfunctions. Childhood and marital history, trauma, and attitudes about sex do not seem to differentiate unresponsive, nonorgasmic, and vaginismic women from each other. It is the way that women individually adapt to and react to these multiple determinants that produces the different symptoms.
These kinds of variables are contributors to the sexual dysfunctions in general: intrapsychic, dyadic, and situational. Traditional therapies such as psychoanalysis tended to lay most of the blame on the first; the new therapies, while not ignoring the intrapsychic, are more likely to focus on the other two.
Intrapsychic factors
Intrapsychic factors are those which arise from conflicts often on an unconscious level within the individual. Deep ambivalence about sex; shame, guilt, and fear can set up negative contingencies which produce avoidance of sexual encounters, defenses against sexual feelings or opening oneself to spontaneous participation. Such feelings are residuals of childhood experiences and conditioning. Repressive teaching about sexuality, harsh punishment for masturbation or exploratory activity, fearsome stories about the horrors of childbirth, or an incorporation of the evaluation of sex as bad or sinful can set up powerful inhibitions to the enjoyment of sexual activity.
Inhibition of responsiveness because of fear of loss of control affects some women. An anxious, insecure woman may be so concerned about monitoring her performance and so guarded in her participation that she cannot risk abandoning herself to her feelings. With its diminution of sensory acuity and of consciousness, orgasm is the triumph of the senses over mind and will. The implications of being out of control are quite threatening to some women.
Resentment, distrust, or fear of men can result in inhibition of sexual pleasure in coitus. Such feeling can emanate from many sources. Harsh treatment by the father, sexual brutality or other trauma related to males, experiences leading to expectation of exploitation or rejection, or to conflict over the dominance-submission dimension in the sexual act may promote a pervasive attitude toward men which is not conducive to enjoyment of coital sex.
Psychoanalysis attributed frigidity in women to unresolved penis envy. Some women do experience envy toward men, as well as fear and anger, because of cultural injunctions which force women into dependent, submissive roles. This can set up strong role conflict in some women who accept the cultural prescription on a conscious level and at the same time suppress the hostility it engenders which they cannot express because of fear of rejection.
Dyadic factors
Dyadic factors in the sexual dysfunctions are those which characterize the relationship between the two persons. It is widely believed that compared to men, women tie their sexuality more closely to the quality of the relationship and their feelings about it. The male’s arousal and ability to have orgasm seem to be less dependent upon relationship factors and to be more affected by the urgency of his sexual needs at the time. While the point is controversial, clinical experience supports the observation that women are much more likely to complain about the context in which sex occurs than men are. They are bothered more by negative qualities in the relationship, including transient ones such as a recent argument, hurt feelings, or the manner of approach. It is quite common to hear a wife say, “We had been fighting all afternoon, and I was really upset. Then when we went to bed he wanted to have sex, exactly as if nothing had happened!” This is not to say that men are insensitive to the quality of the relationship, but rather that women’s responsiveness may be more contingent upon it. The role of cultural conditioning is important, though the extent of its influence is unknown.
Women vary greatly in their preferences where lovers are concerned. Some are completely unable to respond to anyone but their husbands; others are orgasmic only with lovers. Some want to be pursued and captured by a dominant, strongly desirous man; others enjoy seducing and arousing a less-than-bold partner.
Under the best of circumstances a woman may be unable to respond if her partner is inept, too hasty, or unaware of her needs. Some men do not know enough about female sexuality to be good lovers. And some women are too reticent to communicate their needs and wishes to their partner.
Situational factors
Sexual dysfunction can be caused by factors in the immediate sexual situation. The most common of these is inadequate stimulation. Although some women are aroused very quickly and easily to orgasm, many women require extended stimulation before they are ready to have an orgasm. Most males, particularly younger ones, are readily aroused and able to ejaculate in a few minutes or less. If his ejaculation signals the end of the sexual experience, the woman may not even have been aroused. Often the sexual encounter is initiated by and is completely controlled by the male who may simply be guided by his own desires.
Women vary in the kind of stimulation they find most pleasureable. Rhythmic friction of the clitoral area, but not directly on the clitoris, caressing of the breasts, the labia, and other parts of the body are all erotically exciting for most women. The communication of her wishes and feelings helps the partner to meet her sexual needs.
It is probably more difficult for a man than for a woman to know how the other is progressing in the sexual act. Not only is the male arousal state manifest in the erection, but he is often less reticent about the active pursuit of his pleasure. If a woman is silent, or fails to assume responsibility for her own pleasure, he may simply take it for granted that she is having the same kind of experience that he is.
Having been socialized to be nurturing and solicitous of others, many women are more concerned about their partner’s pleasure than about their own. They refrain from making demands because they do not wish to alienate him, interfere with his enjoyment, or wear him out. The fear of displeasing him is basically a fear of rejection, and the insecure woman may choose compliance and passivity rather than take the risk that he will seek someone who is sexually more responsive than she is. While the underlying dynamic in this sort of situation is intrapsychic rather than situational, it mediates what transpires in the situation, particularly with regard to the woman’s willingness to be assertive in the service of her own sexual needs.
There are numerous situational factors which may cause a normal woman to be sexually unresponsive even if the relationship is generally satisfying. If she is worried or anxious about anything, the effect can be inhibitory. A sick child, a visiting mother-in-law in the next bedroom, noises in the hallway, fear of pregnancy, or if the relationship is illicit, fear of discovery and guilt feelings—all these can be inhibitory. Alcohol, tobacco, and body odors can be offensive.
In spite of everything, however, most women are responsive at least some of the time. For those who are not, new therapies are directed not only at the general causes of sexual dysfunctions, but at specific factors which are immediately related to the symptom: general lack of response, inability to reach orgasm, and vaginismus.
Treatment of Sexual Dysfunction
The new therapies for treatment of sexual dysfunction differ from conventional approaches in several important ways. First, the dysfunction itself is seen as the problem. By contrast, a psychoanalytic approach would see the dysfunction as a symptom whose cause must be discovered in the deeper layers of the psyche and dealt with. Only then would the symptom yield. The new therapies, while not neglectful of underlying problems or pathologies, are based on the recognition that many persons who have sexual problems are otherwise normal in every way. Second, the goals of sex therapy are limited to relief of the sexual dysfunction. The initial aim of the therapy is directed at the immediate causes of the problem. More distant possible causative agents, such as childhood events, are dealt with only if they are directly related to the impairment of the individual’s sexual functioning. Third, sex therapy employs prescribed tasks and exercises which the client and her partner carry out when they are alone. They are given specific instructions as to what to do in their lovemaking in order to achieve the desired results. Traditional treatment takes place in the therapist’s office and rarely includes direct intervention in the client’s life or the assignment of tasks.
These basic differences are not uniformly observed by all sex therapists. Many innovations in procedure and technique have been introduced since Masters and Johnson described their model in 1970. Helen Kaplan, whose approach we are describing here, considers sex therapy to be a form of psychotherapy. Although the goal is limited to removal of the sexual problem, the treatment also takes into account both the deeper and the immediate causes. Thus etiological factors such as those we have just discussed are not ignored even if they are nonspecific to the dysfunction and vary greatly among persons with the same symptom. Kaplan views sex therapy as “a task-centered form of crisis intervention” (p. 199) within which conflicts can rapidly be solved.
Persons with inhibited sexual desire experience anxiety around sexual activity, and also may have an underlying hostility toward their partner. When sex is anticipated, they tend to suppress or “turn off” the stirrings of desire by thinking negative thoughts about their partner or themselves. Sometimes they develop a phobic avoidance of sex-related items or situations. Persons with ISD are the most difficult to treat, with the least favorable prognosis. This is because they are usually lacking in insight as to the basic motivations of avoidance and hostility that underly the disorder. The treatment approach used by Kaplan and her associates attempts to modify the patient’s tendency to inhibit erotic feelings, to allow them to emerge naturally. The patient learns not to fight or suppress the natural tendency to become aroused in sexual situations. A combination of experiential tasks aimed at desensitizing anxiety along with more traditional psychotherapeutic sessions is the mode of therapy. The latter includes exploration of conflicts, whereby the patient gains insight into why she doesn’t want to have sex, and the mechanisms she is using to avoid it.
Treatment of general sexual dysfunction is directed primarily to the creation of a nondemanding, relaxed, and sensuous atmosphere in which sexual responsiveness develops. Communication with the partner about her sexual feelings and wishes is encouraged, and certain experiences are prescribed which reduce sexual anxiety and facilitate the unfolding-of sexual feeling. These are, in sequence, the sensate focus, genital stimulation, and nondemand coitus. Sensate focus requires that the couple refrain from intercourse for a while, limiting their erotic activity to touching and caressing each other’s bodies. Freed from the pressure of having to respond, the woman can relax and abandon herself to her own sensations as she focuses on the feelings evoked by her partner’s nondemanding attention to her body. This experience, repeated over a period of time if necessary, often is successful in producing erotic arousal in the woman. When this happens, genital stimulation, again nondemanding and noncoital, is begun. In response to the woman’s arousal, and without any pressure to produce an orgasm, intercourse is the next step. The woman is encouraged to focus her attention on her vaginal sensations with the aim of heightening sensory awareness. The experience is in her control, the goal being to bring out her responsiveness. Therefore, the partner must be willing to suspend his own drive to satisfy his needs in the interest of pleasuring the woman. The exercises have two advantages; they are designed for the erotic pleasure of the woman, and they relieve her of any pressure to respond. Because of this nondemand quality, they do not mobilize that anxiety previously associated with sexual activity (Kaplan, 1974).
This treatment is frequently successful in producing sexual arousal in the nonresponsive woman. Orgasm may or may not result from the process. If it does not, then the failure to have an orgasm is treated as orgasmic dysfunction, the inhibition of the orgasmic component of her sexual-response cycle.
Kaplan conceptualizes the inhibition of orgasm as an over-control of what is basically a reflex function by means of an involuntary ceasing of the response when the premonitory sensations appear. The treatment includes both psychotherapy which fosters awareness of the conflicts causing her to stop at a point just before orgasm, and exercises which show her how to eliminate the blocking of the response. The procedures are different for the woman who does not have orgasm at all and for the woman who has orgasm under some conditions but not others. For the first kind of problem, the exercises are a combination of eliminating tension, encouraging adequate stimulation by masturbation or use of a vibrator if necessary, and teaching the woman to use such aids as fantasy and muscular contractions. Some women are unable to have orgasm in coitus because they require more clitoral stimulation than penile-vaginal intercourse provides. Inability to have an orgasm through coitus alone is extremely common. However, such women were formerly seen as frigid or sick, because it was thought that only the vaginal orgasm was achieved by mature, healthy women, whereas the need for clitoral stimulation for orgasm to occur was an immature persistence of childhood sexuality. According to Kaplan, some women with high orgasmic thresholds cannot reach orgasm in coitus because coitus alone can never provide the stimulation they need. In such cases, anxiety about her failure is dispelled by counseling, and the woman and her partner are reassured that clitoral stimulation to orgasm is completely normal and in no way inferior to coital orgasm. They are shown ways to maximize clitoral stimulation during coitus by both manual and postural variations.
The treatment of vaginismus is less complicated than the treatment of the other sexual dysfunctions. Vaginismus is an involuntary conditioned response which originates in fear of penetration of the vagina. Its treatment has two elements: alleviating the fear and deconditioning the response. The woman is given reassurance and support in addition to an explanation of her vaginismus and its probable origins, and she is instructed in the procedure which she will use at home to gradually eliminate the muscular contraction which closes the vagina. Basically this involves dilating the vagina in gradual increments by inserting, for example, a finger or a tampon. When the woman can tolerate this without anxiety, further dilation is begun. In some cases, a graduate catheter is used, beginning with a very thin tube and progressing gradually to each next-larger size. It is most important that the desensitization proceed at a sufficiently slow and relaxed pace that anxiety is not aroused. At no time should the procedure be repellent or frightening to the woman.
Do the new sex therapies work? Compared to the use of traditional therapy, such as psychoanalysis, other kinds of psychotherapy, or psychiatrically based treatment, the results are impressive. Both Masters and Johnson and Kaplan report that almost all persons they have treated are either cured or improved. Masters and Johnson reported an overall cure rate of 80 percent with their two-week treatment regimen, and a five-year relapse rate of only 5 percent. While not reporting overall percentages, Kaplan agreed with Masters and Johnson that the treatment is close to 100 percent effective for vaginismus and that the great majority of nonresponsive or non-orgasmic women can be helped by these short-term methods developed specifically for the treatment of the sexual dysfunction. Sex therapy is not a panacea, however. The best results are obtained with psychologically healthy people whose relationship with their sex partner is basically sound and rewarding. Kaplan is careful to describe the conditions under which failure to improve or adverse reactions can occur.
Sexual dysfunctions of males can be of importance to women, just as the dysfunctions of women can be important to their male partners. The male sexual dysfunctions of impotence and premature ejaculation and their treatment are dealt with in detail in both Masters and Johnson (1970) and Kaplan (1974).
8. Birth control
Men and women have always longed both for fertility and sterility, each at its appointed time and in its chosen circumstances. This has been a universal aim, whether people have always been conscious of it or not.
—Norman Himes, The Medical History of Contraception, 1963
The shift from the late Victorian viewpoint that held sex to be a duty in the service of procreation to the evaluation of sex as an intrinsically rewarding activity quite independent of procreation was made possible by technological advances which separated sex from its biological consequences. Although the motivation to achieve and to maintain pregnancy has traditionally been reinforced by both social and persona] needs, compelling social trends and related value shifts have undermined the reproductive aim of sexual behavior and reduced the number of children that women will have, as well as the number of women who will have children. Coexisting in the past and in the present with the desire to realize fertility potential is the opposing desire to limit or control it, to make it contingent upon individual choice rather than biological chance. The development of methods and devices that prevent or terminate pregnancy have freed sexuality from reproduction. They can now be viewed as quite separate aspects of a woman’s life to a far greater extent than ever before.
Although the worship of fertility is the basis for most if not all of the oldest known religions, attempts to limit fertility, to control and space births, are as old as history itself and are documented for the last four thousand years. Women in any known society have never had as many children as they theoretically could. Under favorable conditions the greatest number of children that a woman could produce during her reproductive life is about twenty. But the total maternity ratio, the average number of live births per woman past forty-five, even in nonindustrial societies, rarely is greater than 5 or 6 (Wood and Suitters, 1970). In the United States the number of births per woman declined from 7.0 in 1800 to 1.8 in 1983. Thus it is appropriate to consider some of the values that are served by birth control, and the rewards to the individual and to society that accrue as a result of the limitation of fertility.
Social Values and Birth Control
Although explosive population growth has been only recently defined as a problem, it is not difficult to identify factors mediating attempts to control births by those living in earlier times on a less crowded planet. These could have included the availability of food, land, and other resources; the difficulty of migrating with a large family; and the desire to avoid illegitimate children. Also, uncontrolled fertility could mean that an individual woman would be either pregnant or lactating all the time, thus reducing her availability for sexual purposes. The Egyptians saw the avoidance of pregnancy as a way for women to retain their youth and beauty, and four millennia later, Jane Austen, the British novelist, approved of the late marriage of a niece, writing, “You will be quite young in constitution, spirits, figure, and countenance, since confinement and nursing make women grow old” (in Wood and Suitters, 1970, p. 104).
Contemporary values that support birth control reflect both individual needs and social pressures. The recognition of women as individuals and their increasing participation in nondomestic activities make large families and a lifelong dedication to serving them less likely. Children extract a very high price in time, effort, and money, and though most women still expect to experience the role of mother, few are interested in spending all of their adult life caring for young children. The emergence of such values as egalitarian male-female relationships, sexual adjustment, and the quality of life is compatible with the desire for few or no children. The women’s right to control her own body and to enjoy her sexuality without fear of pregnancy are dependent upon reliable methods of birth control. Sexual satisfaction in a relationship is easier to achieve in a situation uncomplicated by pregnancy or fear of it.
Social pressures favor limitation of family size and avoidance of unplanned pregnancies. Since the worldwide population crisis has given priority status to curbing the birth rate, large families have come into disfavor. Responsible fertility control is seen as the only way to solve the population problem, and in most societies this control must still be left up to individuals.
The prevention of pregnancy among the unmarried continues to be regarded as desirable in our society. While such pregnancies are more easily terminated today and are viewed with greater tolerance whether terminated or not, they still are rarely planned or wanted and often involve many problems and much personal distress.
Though the human fertility rate has not yet been brought under control, a developing technology is providing the scientific basis to make such control possible on a broad social basis. Birth control, however, is still very much an individual matter. Its management is not only an important social issue but a crucial determinant in the lives of women.
Birth Control and Health
Successive pregnancies close together are associated with health problems for both mother and child. The ability to space pregnancies permits consideration of the woman’s general condition, as well as health factors such as diabetes, heart disease, or psychiatric conditions, which could be aggravated by pregnancy. Also, studies in developing countries show that infant and child mortality rates increase sharply with the fifth- and later-born children in a family. Children born a year or less after a sibling are twice as likely to die in the first year of life as are those born after a four-year interval (Eckholm and Newland, 1977).
Another advantage of birth control is the reduction of risk of transmitting genetic disorders to children. Huntington’s chorea, cystic fibrosis, and certain anemias are examples of genetically transmitted disorders which married adults might not wish to chance in offspring.
Effective birth control could greatly lower the maternal and infant mortality toll for women who are younger than or older than the age range of maximum safety for giving birth. Fertility may begin from age ten onwards, before young bodies are fully mature, creating risks for both mother and baby. The safest age range for pregnancy is the decade of the twenties. After age thirty, risks begin to rise with each successive year. According to the Population Council, if women gave birth only in the age interval from twenty to thirty-four, maternal mortality in the United States would come down by 19 percent (Eckholm and Newland, 1977). The methods of birth control currently available and in use fall into four categories: abstinence, sterilization, and contraception, which aim at preventing pregnancy, and abortion, the termination of an unwanted pregnancy.
Abstinence
Abstinence for birth control means refraining from heterosexual genital intercourse in order to avoid the risk of pregnancy. Sexual abstinence has historically been advocated for a variety of reasons, most of them related to religion or character development. The notion that abstinence was correlated with sanctity seems to have been a Christian invention. St. Paul, for example, spoke very plainly in an Epistle to the Corinthians:
It is good for a man not to touch a woman ...
For I would that all men were even as I myself ...
... he that standeth steadfast in his heart, having no necessity, but hath power over his own will, and hath so decreed in his heart that he will keep his virgin, doeth well (I Corinthians 7: 1,7, 37).
Proof of victory of the spirit over the body was the major motive for abstention from sexual intercourse during most of the Christian era until the nineteenth century, when physical health of the male was added to its benefits. Conservation of semen meant conservation of energy, and life would thereby be lengthened and debilitating diseases warded off. Sexual abstinence in marriage continued to be widely advocated all during the nineteenth century, primarily in the service of moral and health beliefs. Its practice as a method of birth control was publicly advocated by Thomas Malthus (1766–1834), who proposed it as a solution to the crisis he foresaw of population outstripping the ability of earth to support it. Though his solution was never taken seriously, his concern with the problem of population was an important factor in changing attitudes about contraception. Today, abstinence in preference to other methods of birth control continues to be practiced for religious, moral, or health reasons, or when no other method is available.
In the narrow sense of our definition, it is clear that abstinence as a method of birth control does not necessarily mean total abstention from sexual activity. Nocturnal (involuntary) orgasm, petting to orgasm, self- or mutual masturbation, and oral-genital stimulation are all sexual outlets used by persons who are abstaining from genital intercourse.
The rhythm method
One of the more widely used methods of birth control which requires partial abstinence is called the rhythm method. The rhythm method relies upon abstaining from coitus during the woman’s fertile period. As a general rule an ovum is released from the ovary about fourteen days before the onset of the next menses, but this is highly variable. It is generally accepted that the ovum lives for about twenty-four hours after ovulation if it is not fertilized. Sperm can survive for approximately forty-eight hours once they reach the uterus. Theoretically, then, a woman can become pregnant only during about three days per cycle. Abstaining from intercourse during this period has long been a favorite method of birth control by individuals who felt they must eschew chemical or mechanical methods because of their religious beliefs. Unfortunately, it is difficult to determine accurately the fertile period since women vary in their menstrual schedules and an individual herself may vary considerably from month to month. Two-thirds of women are sufficiently irregular that the use of calendar rhythm alone offers too little protection from the risk of conception. This is especially true of adolescents who commonly experience irregularity for the first few years of their menstrual history, and of women who have just given birth and whose periods are not reestablished on a regular basis. Further, if a woman is lactating she may not menstruate at all.
A slight additional safeguard relies upon the maintenance of a temperature chart during the monthly cycle. At the time of ovulation there is a slight drop in body temperature followed by a rise of half a degree or more, which persists until just before the onset of the next menses (McCary, 1973). One problem is that the change in temperature is not remarkable in some women. Another is the necessity for preparing a chart and for taking and recording the temperature, all requiring planning and resources which are not available for many women. At any rate, the effectiveness of calendar and thermal rhythm for birth control is quite low (McCary, 1973).
The Billings method: “natural birth control”
A further refinement on the calendar and thermal methods requires observation of changes in the mucus secretions from the cervix, and changes in the cervix itself, just prior to the onset of ovulation. The yellowish mucus that is present during the pre- and postovulatory phases of the menstrual cycle becomes sticky and clear during ovulation. In addition, the external area of the cervix expands. It is during this time that intercourse is not advisable. This method of determining when ovulation occurs is known as “natural birth control,” or the Billings method. It requires careful education of the woman or couple for maximum effectiveness (Hatcher et al., 1978).
Studies of the effectiveness of these methods vary widely in their results. Failure rates as high as twenty-five to forty pregnancies per one hundred woman-years have been reported for the calendar and thermal methods,[33] while very low rates of only 2 or 3 percent have been reported for “natural birth control” (Hatcher et al., 1978).
The natural birth control method has been compared with a combination of the calendar, thermal, and natural methods in a yearlong study of 838 Los Angeles young couples (Wade et al., f979). Before the end of the year, three-quarters of those using the mucus method, and two-thirds of those using the combined methods, had dropped out of the study. Of the drop-outs, one-quarter of the natural group and one-tenth of the combined group left because of accidental pregnancy.
Coitus interruptus
Coitus interruptus is one of the oldest and most widely used methods of birth control, as well as one of the least effective. It is correct to consider it a form of abstinence only in that the male abstains from ejaculating into the vagina by withdrawing the penis just before ejaculation occurs. Many couples use this technique successfully over a long period of time. Members of the nineteenth-century Oneida colony, a commune in upstate New York, trained themselves in its use not only for birth control but for the prolongation of sexual pleasure for both sexes. Failure results if the man does not withdraw in time, if the secretion of the Cowper’s glands[34] contains sperm—which can be the case even if ejaculation does not occur—if he has an early partial ejaculation, or if he ejaculates near enough to the vulva that the motile sperm can find their way into the vagina.
Neither abstinence in the narrow sense that we have defined it nor coitus interruptus as methods of birth control need have deleterious effects upon the female since these do not preclude the female orgasm. If the male is practiced in the use of coitus interruptus and can delay his climax until the woman has had as many orgasms as she wishes to have, then his ejaculation outside instead of inside the vagina may not be of great consequence to her. The psychological effects of such methods are more likely to come from lack of confidence with the resulting fear and anxiety, thus spoiling her pleasure as well as interfering with her capacity to have orgasm.
Sterilization
Sterilization is a procedure, usually surgical, by which a person is made sterile, that is, unable to reproduce. Women have been sterilized by X-irradiation of the ovaries or by intrauterine application of radium, but because of the obvious hazards of such methods they are no longer used for sterilization. Today, sterilization may be effected by interruption of the Fallopian tubes or by removal of the ovaries or the uterus, the Erst being the most common when the goal is sterilization and not treatment of a gynecological disorder (see Fig. 7.3).
Tubal sterilization is accomplished by interrupting the uterine tubes to prevent the passage and union of sperm and ovum. While over one hundred variations of this method have been described, most of them may be subsumed under three types (Hatcher et al., 1978). Laparoscopic sterilization has been very popular in the United States. Two small incisions are made in the abdomen, one to admit the laparoscope (an instrument for visualizing the area), the other for the passage of an instrument that cuts the tubes and ties or cauterizes their ends. This procedure leaves no scars, and requires only a few hours of hospitalization. The mini-laparotomy is the most recent tubal method of sterilization to be introduced in this country. The physician makes a single small incision in the lower abdomen, draws the tubes to the incision, cuts them, and either sutures or cauterizes them. The procedure can be performed with local anesthesia in the doctor’s office in less than a half-hour. The classic vaginal tubal ligation has long been in use in this country and many others. The cul-de-sac at the top of the vagina is entered through a small incision, the tubes are sutured and cut, and the incision closed. The patient can go home on the same day.
Tubal sterilization has an analog in the male of vasectomy, a procedure in which two small incisions are made in the scrotum and the sperm-carrying ducts, the vas deferens, are cut, sectioned, and tied (see Fig. 7.2). Since no abdominal surgery is required, a vasectomy is simpler and safer than the tubal methods for the female are. Also, a recent study indicated that the risk of cancer of the cervix may be four times lower in women whose sexual partners have had vasectomies. One speculation for this Ending is that sperm may carry an infectious agent that causes cervical cancer in some women {Spokeswoman, August, 1979).
Oophorectomy and hysterectomy are two other surgical methods of sterilization. Oophorectomy, or the removal of the ovaries, brings ovulation as well as the ovarian cycle to a permanent halt, thus inducing premature menopause in the younger woman. Hysterectomy involves the removal of the uterus and sometimes the ovaries and uterine tubes as well. As a sterilization method, hysterectomy is most often performed at caesarian section. An advantage of hysterectomy is that it removes the risk of uterine cancer. It also means the cessation of the menses, but if the ovaries are left intact the supply of estrogen is unaffected and menopausal symptoms would not occur any sooner than they would have otherwise. Removal of the ovaries or the uterus or both is a major surgical procedure, usually involving an abdominal incision, and requiring several days’ hospitalization followed by two or three weeks of recuperation. While removal of either the ovaries or the uterus will bring the woman’s childbearing history to an end, these procedures are not used for the primary purpose of sterilization but rather for pathological processes in the organs themselves.
The incidence of sterilization. The incidence of sterilization for contraceptive purposes greatly increased in the United States during the decade of the 1970s (see Fig. 8.1.). An estimated 1,131,000 tubal sterilizations and vasectomies were performed in the United States in 1978, an increase of about 37,000 over the previous year, according to a report from the Association for Voluntary Sterilization. Six in ten of the sterilizations were obtained by women, reversing a trend noted in the early 1970s when about seven out of ten of the procedures were obtained by men (family Planning Perspectives, March/April, 1980).
In the 1980s sterilization emerged as the most popular method of birth control in the United States, used by 32 percent of sexually active women aged fifteen to forty-four. Poor women are more likely to rely on sterilization than are more affluent women, but whereas the latter group rely about equally on tubal sterilization and vasectomy, lower income women rely much more on tubal sterilization than on vasectomy. Age, too, is a factor. Only 6 percent of women aged twenty to twenty-four rely on sterilization of themselves or their partners, compared to 62 percent in the thirty-five to thirty-nine-year-old group (Forrest and Henshaw, 1983).
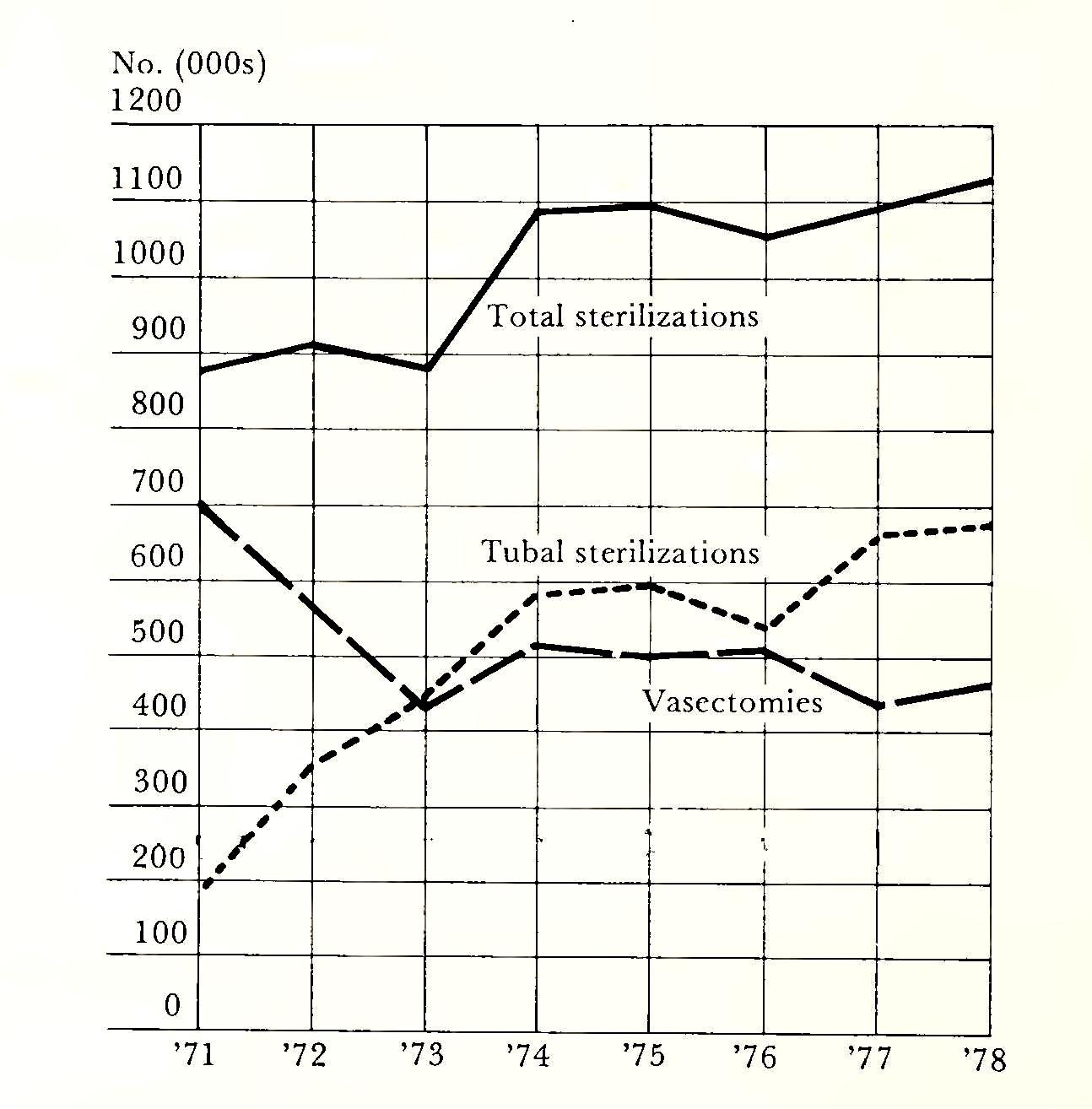
Psychological effects of sterilization. For many women the reproductive system with its manifestations of menstruation and pregnancy is inextricably related to their self-concept, their identity as women, and their concept of youthful femininity. To the extent that this is so, any violation of the system resulting in the visible cessation of its functions would have the potential for producing undesirable psychological side effects. For example, with the reappearance of uterine bleeding in postmenopausal women who were started on estrogen replacement therapy some women experienced an elevation of spirits at this sign of “rejuvenation,” though others found it a nuisance (Kaufman, 1967). Body systems and organs can be invested with a meaning that is far beyond their biological function, and for women the reproductive system is probably the best example, being that which defines them as women, making motherhood possible, a source of both pain and pleasure to themselves and others, and a potent variable in the transactions between the sexes.
One approaches the research on psychological effects of sterilization with caution for several reasons. It is not always possible to separate the noncontraception effects of the surgery itself from the psychological impact, if any, of sterility. When a woman develops symptoms of emotional disturbance following sterilization it is not always discernible whether her symptoms were caused by the surgery or by her knowledge of her sterilization, or whether they would have occurred anyway in the absence of either. Many of the studies are on small samples, and in addition there are the usual difficulties of definition of terms and lack of precision in psychiatric diagnosis. Also, differential effects would logically be expected between surgery performed at the woman’s request and involuntary sterilization for medical reasons, or between, for example, tubal sterilization and hysterectomy, since the former is less traumatic physically and includes the possibility of reversal. Also, hysterectomies are often performed because of cancerous or precancerous conditions, whereas tubal sterilization is most often an elective procedure. If the hysterectomy was related to the threat of cancer, the woman’s psychological reaction would be expected to reflect not only her sterilization but also the life-threatening reason for it.
A variety of symptoms following surgical contraceptions have been reported (Rodgers and Ziegler, 1973). Among them are depression, pregnancy fantasies, false pregnancy, and sexual dysfunction. Negative emotional impact, however, is highly individual and is a function of a number of variables such as the woman’s emotional stability, her mate’s attitude, the size of her family, her understanding of the procedure, and whether or not the operation is elective.
Because of the paucity of general findings on the psychological ef fects of sterilization, attempts to understand or predict such effects must focus on the individual and on the factors that are relevant to her particular case. An example of the interrelatedness of such factors was the experience of a twenty-eight-year-old woman who was married and had two children, a boy aged seven and a girl aged five. She had been under treatment for a year for menstrual problems, including irregularity and heavy flow, when her physician advised her to have a hysterectomy and “get it over with.” She related this to her husband, who agreed, whereupon she had the surgery and was hospitalized for about a week. A month or two later, she began feeling anxious and depressed. She believed that her interest in sex, which had always been high, was diminished, and that she was no longer attractive to her husband. She became obsessed with the idea of having an affair, of actively seeking out someone just to have intercourse with—not to satisfy her sexual needs, but to prove that she could attract a man. Although she was relieved of ‘her menstrual problems, she said that she “missed her periods,” and wished she had them back. When questioned, she did not know whether only her uterus had been removed, or her tubes and ovaries as well.
In this case, while the woman and her husband had agreed to the doctor’s advice, the procedure and its implications had not been adequately described to her. Even if the presence of a uterus has little or nothing to do with sexual pleasure, on a psychological level she equated it with her identity as woman and felt bereft when it was gone. Its meaning, and its loss, had brought out old insecurities which had been dormant within the context of a favorable life situation. Also, the irrevocability of the decision to terminate her reproductive capacity with its cyclical reminder of her sexual identity created anxiety and the feelings of depression which often accompany loss of something of value to the individual. Her age was a factor in that termination of the menstrual cycle would be expected to have a different meaning to a twenty-eight-year-old than to a woman in the climacterium or older. She did not understand the role of ovarian function in introducing the climacterium. If the ovaries had indeed been removed, she should have known this so that she could seek hormonal replacement treatment. It turned out that in this case they had not, but that fact had not been explained to her either before or after the surgery. She required several months of psychotherapy in order to free herself of the psychological aftereffects of her sterilization (also see pp. 463—65 on women and the medical profession).
Negative effects have been observed more often following hysterectomy than after tubal sterilization. One study contrasted twelve hysterectomy patients with ten tubal-ligation patients. Both groups had had elective surgery for contraceptive purposes only, but psychological reaction was much more favorable in the latter group. Even so, 20 percent of the tubal-ligation group and 75 percent of the hysterectomy group were rated as having a “poor outcome,” suggesting that more attention should be paid to preparation of the patients and to the possibility of such sequelae (Barglow el al., 1965). Since this was a small sample consisting mostly of low-income black women seen at a public clinic, no generalizations can be made. The findings are merely suggestive, but they are consistent with a common-sense expectation that the tubal procedure would result in fewer problems.
In fact, a more recent study of women’s opinions about various methods of birth control found that among women relying on tubal sterilization and vasectomy, 95 and 97 percent respectively had favorable responses to their method. These surgical methods were seen as highly effective and not related to the act of intercourse (Forrest and Henshaw, 1983). Such a high level of satisfaction indicates that negative psychological consequences to elective surgical sterilization are quite rare.
In recent years, sterilization has become an increasingly popular means of limiting fertility in developing countries as well. Puerto Rico is a case in point. Between 1950 and 1977 the total fertility rate fell from 5.2 to 2.7 children per woman, and much of this decline was owing to the increase in female sterilization. By 1965 one-third of women who had ever been married aged twenty to forty-nine had been sterilized. This figure had dropped only slightly by 1974, the last year for which data are available. This trend was promoted in part by the exodus of women from their homes to work in factories, in part by the lack of government support for clinics offering other means of contraception, and in part by a benign government attitude toward sterilization (Presser, 1980). But since sterilization continues to be a major means of fertility control in the United States and more recently in developing countries around the world, the question of psychological reactions to sterilization is perhaps peripheral to the larger issue of the right to choose freely among options and to exercise control over one’s capacity to reproduce. Safe sterilization procedures now available for both women and men add to those options and, in a larger sense, give people more control over the conduct of their lives.
Contraception
Contraception may be defined as the use of substances or devices whose purpose is to prevent pregnancy resulting from coitus between fertile partners. Although the “discovery” of sperm did not occur until the seventeenth century, an Egyptian papyrus dated 1850 b.c. described three methods of birth control all of them involving introduction into the vagina of substances which might have retarded the motility of sperm or had a spermicidal effect, such as honey, sodium carbonate, and a paste made of crocodile dung. The use of lint or wool tampons soaked in herbs, wine, and a variety of bark or leaf distillations was recommended by Egyptian writers as early as the sixteenth century b.c., a method which continued to be used in Western society as late as the nineteenth century. Soranos of Ephesus, a Greek physician of the second century a.d., presented a long list of vaginal barriers, such as various oils and tampons, and suggested that people should refrain from intercourse when conception was likely. Unfortunately for those who took his advice, he thought the fertile period was around the time of menstruation (Wood and Suitters, 1970).
During the Middle Ages and subsequently, contraception came to be viewed as a sin, and advice on methods could not be openly promulgated unless one wanted to risk swift punishment. Many tracts were written containing advice on how to conceive, and how to avoid errors which presumably would result in failure. A thirteenthcentury Dominican bishop, Albert the Great, wrote about reproduction and the causes of failure to conceive. Mistakes included failure to achieve simultaneous orgasm, and errors of position. If the woman lay on top, the semen would flow out, thus preventing conception. Other female behaviors, such as rising after intercourse, jumping, sneezing, or urinating, would dislodge the semen and interfere with conception. The attention given to such mistakes suggests that these were deliberate methods used to prevent conception (Wood and Suitters, 1970).
Although the origin of the condom, or penile sheath, is lost in antiquity, it apparently was first described by Fallopius, a sixteenth-century physician whose interest in female anatomy resulted in the uterine tubes being designated by his name. Fallopius described a linen condom to prevent syphilis, and by the early eighteenth century condoms of gut were available. The major use of the condom was to protect the male from infection, although Casanova attributed some of his fame as a lover to his considerate use of it to avoid pregnancy for his partner.
Casanova is also credited with the use both of a gold ball in the vagina to block the passage of sperm, and of a hollowed-out half lemon placed over the cervix. During the 1870s commercial devices to cover the cervix began to appear. Annie Besant, a follower of Malthus, sent private circulars to women describing the “womb veil,” a rubber cap on a flexible ring to be inserted into the vagina over the cervix.
During the nineteenth century gynecologists began to prescribe an incredible assortment of items for introduction into the vaginas and uteri of their female patients to enhance fertility, prop up “fallen” or prolapsed wombs, and cure a variety of female complaints all attributed to the reproductive system. One popular device was the so-called stem pessary, which had over a hundred variations. The basic design was something like a long-stemmed mushroom, such that when inserted, the flat disclike part remained in the vagina covering the cervix while the stem went through the cervix into the uterus. In accordance with the eccentric gynecology of the time, these devices continued to be advertised and prescribed both to cure infertility and to prevent pregnancy well into the twentieth century.
A German physician named Graefenberg is usually credited with the invention in the early 1920s of an entirely intrauterine device to pievent pregnancy, although centuries earlier Arab travelers and oriental farmers were known to introduce pebbles into the uteri of their camels and other animals to prevent unwanted conceptions. Graefenberg’s device was a coiled ring made variously of gut, silver, or gold. The precursor of today’s popular IUD’s, the metal varieties had to be abandoned because they often caused uterine infections.
For thousands of years humans have searched for a reliable, reversible contraceptive that could be taken orally. Apparently contraception was not forbidden in early Jewish law, and herbal drinks were given on occasion by rabbis to women who for one reason or another ought not to become pregnant. A fifteenth-century Spanish story, La Celestina, describes contraceptive potions issued by Celestina, a midwife, abortionist, and “something of a witch,” and Daniel Defoe wrote in 1727 of women who took “purgations, potions, and poisons” to avoid childbearing (Wood and Suitters, 1970). But an effective oral contraceptive had to wait until science developed an adequate understanding of the female reproductive system, its hormonal regulation, and the hormones themselves.
The search for the perfect contraceptive continues. Those substances and devices that are available, their effects on women, and the trend of continuing research are the topics of the next section.
Oral contraceptives. The clue to the development of oral contraceptives was the fact that during pregnancy a woman does not ovulate owing to the large quantity of progesterone in her blood. This hormone is secreted by the corpus luteum, the ovarian structure that develops from the site vacated by the ovum as it erupts from its follicle. During the 1930s progesterone was isolated from the ovarian tissues that produce it, and a decade later it was shown to inhibit ovulation in rabbits. However, extraction of the natural hormone from female animals was prohibitively expensive, and serious development of its use on humans did not begin until the 1950s following the discovery that progesterone could be derived from certain plants. Subsequently progesterone was synthesized in the laboratory and a number of related products collectively called progestagens, all resembling progesterone in their actions on the body, became available in large quantities. Early experimental trials with these substances confirmed that some were indeed powerful inhibitors of ovulation, but that they gave poor control over the menstrual cycle with irregular, unpredictable bleeding. Combination of the synthetic progestagen with a synthetic estrogen, however, relieved this problem, and in 1956 such a combination was successfully tested in controlled studies on Puerto Rican and Haitian women. Thus began the era of “the Pill.” In less than two decades the development and production of oral contraceptives became a huge pharmaceutical industry, and the Pill in one form or another became a widely prescribed method of fertility control in the United States.
Several dozen varieties of the oral contraceptive are presently available, most of them consisting of a combination of synthetic estrogen and progestagen in varying strengths and dosages. Basically, the Pill acts by imitating the state of pregnancy. The ingestion of the hormones normally secreted in large quantities during pregnancy causes the pituitary gland to inhibit its production of FSH, the hormone that promotes the maturation of the ovum in its ovarian follicle. Thus no ova mature, and fertilization cannot occur. Also, the hormones have an effect on the intrauterine surface, modifying it so that implantation of a fertilized ovum is less likely to occur; in addition, they cause the mucous plug of the cervix to become more resistant to the invasion of the uterus by sperm.
Typically, a woman takes the Pill for twenty consecutive days, beginning on the fifth day following the onset of her menstrual period. Normally her next period will begin about three days after she takes the last dose. This regimen thus effects a twenty-eight-day menstrual cycle which is highly predictable for most, but not all, women taking the Pill.
A variant is the “morning-after’ pill, involving the administration of large amounts of estrogen for several days following possible exposure to pregnancy to prevent implantation of the zygote in the uterus. While sometimes administered to rape victims, the “morning-after” pill is not used routinely for contraceptive purposes. This is because of negative side effects associated with the high estrogen level. In addition, the estrogen most commonly administered as a post-coital contraceptive is diethylstilbestrol (DES), which has recently been shown to cause excess breast and endocrine cancer in women users. DES had been widely prescribed for many years as an anti-miscarriage agent. It was this use that led to the recent findings that it had caused vaginal cancer in the daughters of some women who took it. In spite of the carcinogenic properties of the drug, it continues to be prescribed to suppress lactation after childbirth, and for such unapproved uses as the relief of acne and the treatment of “mental disorders” (Spokeswoman, March 15, 1978).
Reactions to oral contraceptives. Most of the women who begin taking the combination oral contraceptive pill report physical changes and frequently psychological changes as well. The nature and extent of those changes are dependent upon a number of factors. First, the pills contain synthetic estrogen and progestagen, thus producing symptoms associated with elevated levels of these hormones. Commonly reported physical symptoms include increased breast size with soreness and tenderness, water retention and weight gain, headaches, nausea, vaginal discharge, more regular menstrual cycles, and improvement of acne. Second, types of pills vary in the relative amounts of estrogen and progestagen they contain. Considerable evidence indicates that the gonadal hormones influence mood states in women, although the results are far from definitive (Eagan, 1985). Third, the individual physical and psychological status of the woman herself can be expected not only to interact with Pill-induced changes, but also to determine her perception and tolerance of them and her reactions to them.
While the oral contraceptive pill is the most effective contraception product currently available, it is not without physical risk. Its most serious side effect, attributed to the estrogen content, is the increase of circulatory clotting disorders, such as strokes.
Also the Food and Drug Administration now warns Pill users that the risk of heart attack for those who smoke is Eve times greater than for non-smokers, and ten times greater than for non-smokers who are also non users of the Pill. The risk increases with age and amount of smoking. Regarding the Pill and cancer, both positive and negative effects have been observed. Studies have shown that use of the Pill substantially reduces the incidence of endometrial and ovarian cancer and apparently has no effect on the likelihood of breast cancer. There are indications, however, that Pill use increases rates of cervical dysplasia (a possibly precancerous condition of cervical cells) and of invasive cervical cancer (Eagan, 1985).
Psychosomatic and psychological reactions to the Pill have been assessed through tests and interviews used to evaluate personality and attitudes toward the body before and three months after beginning the use of oral contraceptives. The women reported three kinds of body changes: normal, unusual, and beneficent. Normal changes were those expected because of the high hormone levels, including breast soreness, weight gain, and the others mentioned above. These changes tended to be reported by psychologically normal women, who acknowledged them with normal levels of anxiety or hostility. Unusual changes were the opposite of the expected drug effects, and included smaller breasts, irregularity of menstrual cycle, and more acne. Women reporting these kinds of changes were characterized by passivity, difficulty in expressing anger, and feelings of being used in the sexual relationship. Beneficent body changes were increased energy, reduced appetite, and weight loss. Women who experienced such changes had a high degree of dependency upon the sexual partner for self-esteem, and such positive changes were seen by them as enhancing their value to the partner (Bardwick, 1973).
The subjects in this study also reported on psychological changes subsequent to Pill use. Some of these changes were: feeling less feminine and attractive, increase in depression and anxiety, and decreased interest in sex and frequency of orgasm. Such negative changes were reported by both psychologically healthy and less healthy subjects. The healthier women were expressing appropriate levels of anxiety and resentment as they perceived normal body changes resulting from their responsibility for contraception. The passive women who had unusual changes seemed to be somatically expressing their anger, an indirect form of hostility toward those who might be responsible for their unpleasant symptoms. Dependent women with a high fear of pregnancy were most likely to report positive psychological changes with anxiety reduction and enhancement of self-esteem. Thus the pre-existing personality of the woman interacted with hormonally induced effects to determine to some extent both psychic and somatic consequences of Pill use. Other variables are also important. The woman’s relationship with her partner, her feelings about the sexual use of her body, her motives for avoiding pregnancy—these and other dynamic factors must affect her reactions to the use of any contraceptive, let alone one with such telling effect upon her entire reproductive system (Bardwick, 1973).
Other hormone-based contraceptives. Beside the oral contraceptive, there are some other hormone-based contraceptives now in use. One example is Norplant, a contraceptive implant system containing the synthetic progestin levonorgestrel. In this case, a capsule is implanted under the skin of a woman’s forearm. The synthetic hormone is gradually released. Some pilot clinical studies of the system have found this method to be highly effective in preventing pregnancy for at least five years after a single administration. But there are some side effects, such as irregular bleeding, prolonged menstrual bleeding, and amenorrhea. Roughly 40 percent of the women in the studies mentioned at least one of these problems. (Population Council, 1980).
Meanwhile the search to increase the repertoire of contraceptive technology goes on. A recent report described a promising line of research involving a synthetic luteinizing hormone-releasing hormone (LHRH) as a contraceptive for both women and men. LHRH is naturally produced in the hypothalamus, moving from there to the pituitary, where it triggers the production of LH and FSH (see Chapter 4, pp. 97—133), both of which play key roles in the reproductive cycle. LHRH causes a sharp rise in LH and FSH, followed by a drop below base level. The effect on women is to interfere with the maturation of the follicle from which the ovum erupts at ovulation, and to inhibit likewise the production by the corpus luteum of progesterone, without which the uterine lining is not readied for implantation. In men, the lowered FSH level suppresses spermatogenesis, the effective production of sperm. The efficacy and safety of LHRH are still being tested experimentally, although, as the report states, much more data have been developed on women than on men (Benditt, 1980).
The search for effective male contraceptives has been frustrating to scientists and mostly fruitless. But one substance, Gossypol, a component of cottonseed oil, has been discovered by Chinese scientists and is said to have contraceptive properties. Gossypol appears to suppress sperm production and to affect the structure and motility of sperm in the epididymis (Benditt, 1980).
How do men react to experimental hormonal contraceptive methods? Do they hud them acceptable? Are sexual desire or performance affected? These questions were investigated among small samples of volunteers in Bangkok, Hong Kong, London, Santiago, Seoul, and Toronto. Sexual functioning and acceptability were monitored as the men were administered an androgen-gestagen combination, cyproterone acetate (an antiandrogen steroid), or a placebo. The first two have both been shown to suppress spermatogenesis. The men expressed high initial acceptability to the new contraceptive, rating it higher than either vasectomy or the condom. Those who received cyproterone acetate, however, experienced highly consistent decrements in sexual functioning, both in desire and in performance. As one would expect, their subsequent acceptability of the regimen was much lotver than was that of the other two groups. Even so, their stated intention to use the method in the future was not affected. Since this is said to be the best predictor of future behavior, the researchers concluded that efforts to develop and perfect such contraceptive methods for men should continue (World Health Organization Task Force, 1982).
It is apparent that there is a scarcity of birth control devices for men; one can’t help but notice that the majority of the current methods are for women. Indeed, women are usually the guinea pigs for new products and they, along with their offspring, are susceptible to the risks of scientific experimentation. In addition to the hazards women face, the current lack of more devices for men also tends to burden them to assume much of the responsibility of birth control.
Intrauterine contraceptive devices (IUD’S). IUD’s are small devices either plastic or metal which are inserted into the uterus by a physician. They are believed to act in some way to prevent implantation of the zygote in the wall of the uterus. The IUD remains permanently in the uterus until the woman wishes to become pregnant at which time a doctor can remove it.
Since the IUD is a foreign object, the uterus may attempt to reject it at first. About 10 percent of all IUD’s are expelled in the Erst year, though 40 percent of these will be retained on a second insertion (Westoff and Westoff, 1971). Some women experience cramps and bleeding after insertion, a reaction which usually disappears after a few days or weeks. IUD’s have become very popular in the past ten years especially among women who cannot take oral contraceptives because of negative side effects. They are inexpensive, require no attention, and have no common side effects other than those mentioned. However, they are not as reliable in preventing pregnancy as oral contraceptives are. About 2 percent of women with IUD’s in place become pregnant in the first year of use. After that the risk is less.
A serious but uncommon risk with the IUD is infection from perforation of the uterus. In fewer than one in ten thousand cases, perforation occurs when the device is inserted into the uterus. Although this is a rare event, it can be fatal. Obviously, the skill of the physician is important in reducing or eliminating such a risk.
Other risks include ectopic (tubal) pregnancies and pelvic inflammatory disease. A review concluded that the IUD must be used cautiously, but that it has advantages for many women, particularly those who have had more than one pregnancy, and that it can offer for most a safe and effective means of contraception (Population Reports Series B, #4, 1982).
The diaphragm. The diaphragm is a shallow cup made of thin rubber on a flexible ring, designed to fit over the cervix to prevent the passage of sperm into the uterus. Fitted and prescribed by a physician, it is used with a spermicidal cream or jelly which also provides lubrication. It must be inserted shortly before intercourse and left in for six to twelve hours after in order for the jelly to be effective.
While in principle the diaphragm and spermicide combination is highly effective, in practice it has a failure rate of 5 to 20 percent. There are several reasons for this. Unless advance plans have been made, the woman must interrupt the love-making to insert the diaphragm. One is often tempted not to use it. The diaphragm may be inserted incorrectly, or it may slip during intercourse. Correctly fitted and used, however, the diaphragm is a reliable contraceptive device with no negative physical side effects.
Prior to the advent of the Pill in the mid-1950s the diaphragm was women’s only effective means of contraception. Recently the disillusionment of many women with the Pill and its attendant risks has renewed interest in and popularity of the diaphragm. Its great advantage, of course, is that it does not interfere with the normal physiology of the body.
Other contraceptives. A few contraceptives are available without a physician’s prescription. These include the condom, chemical methods, and douches.
The condom, or penile sheath, is made of thin rubber or sheep intestine. About 7!4 inches long, it is slipped over the erect penis before penetration. It works on the simple principle of containing the seminal fluid so that none of it gets into the vagina. There are several possibilities for failure, however. The condom may be defective; it may break during use; or it may slip off after ejaculation when the penis becomes flaccid or is withdrawn from the vagina. The condom may be inspected before use by blowing air into it. If seminal fluid spills into the vagina owing to breakage or slipping off, contraceptive cream or jelly should be inserted into the vagina immediately. If this is not available, a water douche can be used.
Correctly used, an intact condom is highly effective. Also, it is the best method, other than abstinence, to prevent the spread of venereal diseases. A survey of Consumer Reports readers (most of whom are white, middle-class, and educated) found that condom users believe that its advantages outweigh its disadvantages. Women in particular were pleased because it has no side effects. Of all those who used condoms for contraception, two out of three said they had switched from another method. Most of these had changed from the Pill because of concern over its safety and side effects (Family Planning Perspectives, March/April, 1980).
Chemical methods of preventing conception are spermicidal creams, jellies, and foams. They must be introduced into the vagina a few minutes before ejaculation occurs, and the process repeated if intercourse continues. These substances, while better than nothing, are among the least reliable of the contraceptives, with a failure rate of about 25 percent.
Douches can be used to flush seminal fluid out of the vagina immediately after ejaculation occurs. Water alone, or combined with vinegar or a commercial preparation, is a harmless vaginal wash, but mostly ineffective as a contraceptive. Although water is toxic to sperm, the douche often fails to reach them because they move so rapidly into the cervix. Studies on the effectiveness of douches as a regular means of contraception report a failure rate of about 35 percent.
Teenagers, Sex, and Birth Control
The first time, it was like totally out of the blue. You don’t ... say, ‘Well, I’m going to his house, and he’s probably going to try to get to bed with me, so I better make sure I’m prepared.’ I mean, you don’t know it’s coming (Kisker, 1985, p. 83).
Pregnancy rates for American teenagers are higher than those for their teen counterparts in thirty other developed countries, except Hungary. American teenagers have the highest abortion rates of any of the countries from which statistics are available, and their childbearing rate is higher than that of any of the other countries, except Hungary and Rumania. The high childbearing rate of adolescent blacks, about three times that of whites, does not account for this last difference, since the childbearing rate for whites aged seventeen and younger in the U.S. is still higher than that for teens in any of the countries, except the two mentioned and Greece and Iceland (Westoff et al., 1983).
Over the past decade, the rate of childbearing among teenagers, both black and white, has been declining, though pregnancy rates are continuing to rise along with the increase in sexual activity among adolescents that has been observed since the 1960s. Sexual activity among U.S. teens, however, does not appear to be any higher than in England, Sweden, Denmark, and the Netherlands, where both adolescent fertility and abortions are very much lower than they are in this country (Lincoln, 1983).
What accounts for these differences? In Sweden, for example, teenage pregnancies have declined remarkably in recent years, even though teenage sexual activity is widespread and culturally acceptable. Some proposed reasons for this decline include easy access to contraceptive services, strong ideological support for responsible sexual decisions shared by both partners, integration of contraception education into the wide context of human relationships, and supportive attitudes in the medical community (Lincoln, 1983).
In the United States, by contrast, studies have documented high levels of nonuse and inconsistent use of contraception by sexually active teenagers. A national survey found that more than half of teenagers exposed to a pregnancy risk did not use a contraceptive because they thought they could not get pregnant at that particular time. Some said they used no method because they had not expected to have intercourse. Other reasons included not having a method at the time of intercourse, the partner’s objection, lack of knowledge about methods and their availability, and assertions that contraceptives are too difficult or unpleasant to use. Because of this deficit in contraceptive use, it was estimated that about one in ten U.S. teenagers had a premarital pregnancy in 1982 (Kisker, 1985).
Using group discussion methods with sexually active teenagers, a major study aimed at investigating poor contraceptive use was carried out in five U.S. cities. Participants were mostly white males and females from middle-class and lower-middie-class families.
Exemplified by the girl quoted above, most of the study participants said they had used no method at their first intercourse, primarily because they were unprepared for that possibility. Even in later encounters, many expressed feelings of ambivalence about being prepared:
There could be that casual guy you just met. You know it’s going to be a big thing and you want to have sex with him, and you’re not going to say, ‘Give me a few weeks. Let me get started on the pill’ ... You take a chance (Kisker, 1985, p. 84).
Most of the young women in the study were consciously aware that they could get pregnant in unprotected intercourse, but thought that the chances were small. Some went to a family planning clinic only after a pregnancy scare. One who was very ambivalent about being sexually active said that she did not use contraception because of her fear of pregnancy: “If I did [use a contraceptive] then I’d have sex more. Then it would be too easy. The risk won’t be there ...” (p. 85).
As to sources of information about sex and birth control, most mentioned school and friends, though some were aware that friends don’t always have the right answers: “Sometimes they don’t even have sex and they think they know it all.... ‘Oh, you won’t get pregnant standing up.’ You think you know so much when you are younger.” (p. 85). Parents were not an important source of information, seemingly because of mutual embarrassment and parents’ inability (as seen by the teenagers) to deal with specific behavior in preference to generalities and euphemisms.
Time and again the moderators found that teenage girls could not plan for first intercourse or for subsequent intercourse with new partners because to do so would be to admit that they were sexually active. The confusion and ambivalence many feel about their sexuality stems in part from lack of knowledge, but in part also from the mixed messages they receive from society about values related to sex. On the one hand, premarital sex is not approved, though tacitly condoned. On the other hand, the excitement and romance of sexual encounters are portrayed everywhere in the media, and the prepotent goal promoted for girls and women is to be sexually attractive and desirable to men. She may be “swept away” but not admit that romantic passion leads to intercourse and unprotected intercourse leads to pregnancy.
Though the barriers to effective contraceptive practice among teenagers are formidable, they have been lowered in other countries and can be lower ed here. The study recommended, among others, a national policy supporting reproductive and contraceptive education in all public junior high schools, the use of students as peer teachers of the “facts of life,” widespread availability of information about clinics that can provide information to young people about contraception, promotion of the pill as the best contraceptive for teenagers and of the condom for the prevention of sexually transmitted diseases. Too, the role of young men should not be ignored. Many of the young men in the study assumed that they had no legal obligation to a child fathered out of wedlock or to the child’s mother. Some were quite cavalier in their attitudes about their partner’s use of a method (“That’s her problem”) or about the possibility of pregnancy (“You don’t have to worry about pregnancy if you’re not going to see the girl again, anyway”). Male teenagers need to be educated about their responsibilities and sanctions strengthened against young fathers who refuse involvement, financial or otherwise, with their offspring (Kisker, 1985).
Abortion
Abortion is the practice of terminating unwanted pregnancies. It is probably the oldest and most widely used method of preventing the birth of unwanted children.[35] A Chinese medical text described a method for inducing abortion by mercury five thousand years ago, and Egyptian papyri of the same era describe other techniques. Abortion was common among the Greeks and Romans both for population control and for the preservation of feminine beauty. Greek philosophers favored family limitation for eugenic reasons, and Aristotle spoke frankly to the matter:
If it should happen among married people that a woman, who already had the prescribed number of children, became pregnant, then before she felt life, the child should be driven from her (Taussig, 1936, p. 32).
Presaging contemporary concern with the ethical issues of abortion, Aristotle believed that it should be permitted before the soul entered the fetus, but not after. Since this event was thought to occur at forty days for the male and eighty days for the female, abortion would be restricted to the first forty days. Methods included abortifacient drugs, instrumental interference, and intrauterine injections. Drug-soaked tampons and pessaries made of metal or wood were also commonly used (Bates and Zawadski, 1964).
The practice of induced abortion has been found among nonliterate people all over the world. Methods include the ingestion of supposed abortifacient drugs and herbs, violent exercise, and if these are not effective, beating or stamping on the abdomen. Mechanical means such as an “abortion stick” are also common. Used by a primitive Hawaiian group, the stick is a curved piece of wood about twelve inches in length and one inch in diameter, coming to a sharp point. The handle is carved in the form of the head of an island god.
In Western society, the development of moral and legal sanctions against the practice of abortion is traceable through the corpus of Jewish law and the position of early Christian theologians. The Old Testament contains only one reference to it, stating that a fine may be levied “if men strive together, and hurt a woman with child, so that her fruit depart,” but she herself survives. But if she were fatally injured, then those responsible had to “give life for life.” (Exodus 21:22–23). The Talmud ruled that the unborn child might be destroyed to save the mother’s life. These two references sum up the classic Jewish view: abortion was permissible only to save the mother’s life; otherwise, destruction of the unborn child was a serious offense, but not murder (Jakobovits, 1973). Christian theologians almost from the beginning denounced abortion for any reason whatsoever. Sanchez, a sixteenth-century Italian, allowed that a rape victim could attempt to get rid of her attacker’s semen, but this right was terminated at the moment when the semen achieved “peaceful possession” of the victim’s uterus (Means, 1970).
The history of abortion is the history of women’s attempts, for whatever reasons, to avoid bearing unwanted children and to have some measure of control over their reproductive function. During the colonial period in the United States, the sanctions against abortion were mostly religious and moral, involving strong social taboos. In the nineteenth century, as an independent body of American law developed, most of the states passed laws making abortion a criminal offense unless to save the life of the mother (David, 1973).
On January 22, 1973, the Supreme Court in Roe vs. Wade handed down a landmark decision that upheld a woman’s right to decide whether or not to terminate her pregnancy. The Court, however, did not recognize a woman’s right to absolute control of her body. That right could be limited where the state had a “compelling interest.” Such interests were in protecting the health of the pregnant woman, and in protecting the potentiality of human life. During the first trimester, neither interest is compelling, and the woman and her physician may decide. In the second trimester, the state’s interest in the woman’s health becomes compelling, and the state may then regulate the abortion procedure in ways that are related to her health. When the fetus becomes viable in the seventh month, the state’s interest in the potentiality of life becomes compelling; it may then regulate or proscribe abortion, except where it is necessary to preserve the life or health of the pregnant woman (Hatcher, 1978; Hayler, 1979). In July, 1976, the Court held that the state cannot require consent of a third party (spouse or parent) on a woman’s right to abortion. Consequent to these decisions, 1.6 million abortions were performed in the United States in 1984, making it the most common surgical procedure in the country.
While women’s right to abortion was greatly enhanced by these decisions, in practice it was not equally available to all. First the Supreme Court has since ruled that states are not required to pay for nonthei apeutic abortions for poor women. Also, the so-called “Hyde Amendment”[36] limits federal reimbursement to only those abortions performed when the woman’s life is in danger, when her health is likely to be damaged by the pregnancy, or when the pregnancy is the result of rape or incest. “The practical effect of these decisions is to make abortion a right for women who can afford it and a privilege for the rest” (Hayler, 1979, p. 310). Second, while the number of abortions has increased, their availability remains limited to certain sections of the country. That is, not all clinics and hospitals in all cities, towns, and rural areas have facilities for abortions.
Abortion means the termination of a pregnancy before the fetus is viable, that is, before it can survive outside the uterus. It is generally held that a fetus is nonviable prior to the beginning of the seventh month, although there is considerable variation in the definition of viability (David, 1973). Several medical methods are in use for the induction of abortion, depending upon length of the pregnancy and preference of the physician.
Methods of abortion. Early abortions, performed in the first thirteen weeks after a woman’s last menstrual period, are associated with fewer risks and complications than are those performed later. Since 1972 (when abortion was legal in a few states) the percentage of abortions performed after thirteen weeks of gestation has decreased substantially. In that year nearly 18 percent of abortions were performed in the second trimester. In the 1980s second trimester abortions account for about 10 percent of all abortions (Grimes, 1984).
The most commonly used medical technique for the termination of pregnancy up to thirteen week’s is the vacuum suction method. The cervix is dilated under local or general anesthesia, and a sterile tube attached to a suction pump is inserted into the uterus. The uterine cavity is emptied in a few minutes. This procedure is usually done on an out-patient basis, as hospitalization is not required.
A related practice is menstrual extraction, the removal of the uterine contents in the first week of two after conception has occurred. After pregnancy is confirmed, the physician inserts a tube through the cervix into the uterus. The uterine contents are suctioned out by a syringe attached to the free end of the tube. Since this method has failure rate of 2.5 percent, compared to less than one percent for the suction abortion method, some physicians prefer to wait a few weeks and use the latter method.
Between thirteen and sixteen weeks of pregnancy the procedure of choice is dilatation and evacuation (D & E). Either local or general anesthesia may be used. Since the cervix must be dilated more for second trimester abortions, laminaria rods are often inserted the day before the surgery. The use of laminaria (a small tubular marine plant) promotes slow cervical dilation owing to their moisture-absorbing quality which causes them to swell, thus making unnecessary the use of instruments that may damage the cervix. After dilation, special instruments are used to scrape the walls of the uterus. D & E is usually performed in a hospital on an outpatient basis.
The termination of pregnancies between sixteen and twenty-four weeks is accomplished by instillation methods. These involve injection of either a saline solution, the drug prostaglandin, or urea, a chemical compound, into the sac that contains the amniotic fluid. More recently, a combination of urea and prostaglandin has been used. These abortifacient substances cause labor to begin within a few hours, followed by the delivery of the fetus usually within twenty-four hours. This means that the woman will be in the hospital for one or two days.
The two most important determinants of the safety of abortion are the length of the pregnancy and the method used. In general, the earlier the abortion is performed the safer it is. Studies have shown that for abortions at thirteen weeks or longer gestational time, the D & E results in the fewest complications, followed by a combination of urea and prostaglandin. This combination was significantly less likely than saline solution to result in such complications as fever and hemorrhage, and the interval from instillation to abortion was much shorter. It should be noted that the superior safety record of the D & E is owing to its advantages in the thirteen to sixteen week period. At seventeen or more weeks, its rate of complications was similar to that of the urea-prostaglandin method. (Grimes, 1984).
Psychological effects of abortion. Do women typically experience negative psychological effects as a result of having an abortion? Examination of the literature on the after effects of abortion reveals an almost complete turnabout of medical and psychiatric opinion on this question. Prior to the 1970s it was difficult to find a psychiatric authority who did not believe that the experience of abortion left serious psychological scars on the woman’s psyche, especially depression and guilt. A few years later the emerging research on post-abortion psychological effects is almost unanimous in proclaiming them negligible. Several factors appear to be important in bringing about this change.
First, the climate of belief about abortion and its relation to woman’s role has changed. One typical psychiatric attitude is that since woman’s main role on earth is to conceive, deliver, and raise children, it was to be expected that “when the function is interfered with, we see all sorts of emotional disorder” (Bolter, 1962). As long as doctors and women themselves believed that their main role was defined by their reproductive function, that is, “A woman is a uterus surrounded by a supporting organism” (Galdston, 1958), then the logical extension of this belief led to a prediction of distressing consequences to interference with it. The emergence of different views which valued women’s freedom to define their roles in any way they chose forced a revision in thinking about women which required a changed attitude toward abortion.
Second, it is only since the legalization of abortion in this country that carefully controlled research studies on the psychological sequelae have appeared. Earlier opinion tended to be based on a few case studies or on uncontrolled clinical observation, the resultant data being used to buttress arguments based on the particular belief of the reporter—a marriage of ideology and evidence which may constitute revealed truth to the believer but is hardly science. Objective research directed to this question has generally contradicted psychiatric belief in the emotional-trauma theory of abortion.
Third, the legalization of abortion and its widespread acceptance and availability have largely moved it out of the class of behaviors for which one should, in the traditional view, feel guilty and be punished. Prior to the 1973 decision, a woman living in a state with a liberal abortion law could have a safe legal abortion if a psychiatrist would certify that the continuance of the pregnancy was detrimental to her mental health. Since that time, however, large numbers of women have had legal abortions simply because they did not wish to have a child, regardless of the reasons for such a wish. This removal of abortion from the influence of religious and quasiscientific beliefs permits its effects to be more accurately measured.
The question of whether abortion would have the negative psychological aftereffects which had been attributed to it was the subject of a study (Fingerer, 1973). Tests measuring anxiety and depression were administered to groups of persons as follows: group la, numbering 324 women who came to a clinic for an abortion during a three-week period; group lb, numbering 177 of the women in group la who returned questionnaires after their abortions; group 2, consisting of 207 men and women who accompanied group la to the clinic; group 3, consisting of male and female postdoctoral students in psychoanalytic training programs; and group 4, made up of female graduate and undergraduate psychology students who were asked to role-play either the abortion patient or one accompanying her to the clinic. Groups la and lb were instructed to respond to the tests in accordance with how they felt on the day of the abortion and again afterwards. Groups 2, 3, and 4 were asked to project themselves into the abortion patient’s position and respond as they thought she felt. According to the results, the women who were the abortion patients reported less anxiety and depression than did any of the subjects who were predicting how they would feel. The postdoctoral psychoanalytic group predicted the highest scores for anxiety and depression; the lowest scores came from the responses of the women themselves, after the abortion. In contrast to psychoanalytically oriented predictions of psychological distress associated with abortion, the women themselves reported only a transient mild depression which was not above expectation for any minor surgical procedure. “The psychological aftereffects of abortion seem to reside in psychoanalytic theory and societal myths” (Fingerer, 1973).
A later study investigated emotional reactions to abortion and their relation to other variables in six hundred clients of an abortion clinic in a university town. Using feedback sheets completed by the women at a postabortion checkup visit, the researchers asked the women to describe their major emotional reaction to the abortion. The choices were relief, guilt, happiness, depression, worry, sense of loss, and other. Two-thirds (64 percent) of the women checked either relief or happiness, and were assigned to the positive evaluation group. Depression, guilt, worry, sense of loss, or some combination of these were check by 13 percent, who were designated the negative evaluation group. Finally, 23 percent checked a combination of positive and negative reactions and made up the ambivalent group. Analysis revealed that the women who had negative reactions to their abortions reported heavier and longer periods of postabortion bleeding and more cramping. They were also more critical of the staff and the procedure, perceiving, for example, the doctor as more impersonal, the initial contact as too brief, and the boyfriend as feeling left out.
A second part of this research found that negative outcome women could be reliably predicted by certain preabortion factors. These women reported in preabortion counseling sessions a history of menstrual problems, a greater number of prior health problems, more mental health problems in the family, and prior use of and difficulty with contraceptives.
The important finding in this study is that a large majority of the women gave positive evaluations with positive emotional responses to their abortions. Those that responded negatively were more likely to have experienced preabortion health or emotional problems that affected their physical and mental responses to the abortion (Levy, et al., 1979).
Other studies confirm that psychologically healthy women do not usually suffer adverse effects from the experience of abortion. To the contrary, the termination of an unwanted pregnancy with its concomitant stress alleviates the emotional distress accompanying such a condition. Abortion per se, however, does not necessarily modify a preexisting psychiatric condition. Women with the most severe symptoms before an abortion are likely to show the most severe symptoms later. The abortion is simply an intervening event with no specific causal effect (Sarvis and Rodman, 1973; Shusterman, 1976).
Abortion: The Continuing Controversy
The practice of abortion—its history, methods, and impact on the women who experience it—is of interest not only to behavioral scientists. It has become a moral and ethical issue that has polarized public opinion as few other issues have in recent times.
As Kristin Luker (1984a) pointed out in Abortion and the Politics of Motherhood, until the 1970s the question, Is the fetus a person or only a potential person? was argued mostly by male physicians, some of whom believed that abortion was murder, and others who wanted the right to perform legal abortions that would protect women psychologically and physically. After the 1973 Supreme Court decision that legalized abortion, the debate became public and in the 1980s has become one of the most divisive issues in American life.
Luker’s book describes a five-year study of over two hundred prolife and prochoice activists in an attempt to identify the differences in their lives and belief systems that would account for the depth and intensity of their disagreements on the abortion issue.[37]
Who are the activists? Though males are still prominent in the leadership structure, especially among prolife groups, more than 80 percent of those identified as highly involved on either side are women. And the women on both sides are separated by much more than their views on abortion.
The typical prolife activist in the study is a forty-four-year-old woman who married at age seventeen and has three or more children. A high school graduate, she is married to a small business man and the family income is less than thirty thousand dollars per year. She is most likely to be a Catholic. Her religion is important to her, and she attends church at least once a week.
The typical prochoice activist is also forty-four years old. Married at twenty-two, she has one or two children. She has had some graduate or professional training after her B.A. degree. She is employed, married to a professional man, and her family income is more than fifty thousand dollars a year. She rarely attends church, and religion is not important to her.
The views on abortion of these two groups of women are closely tied to their views on the critical issues of gender, sex, and parenthood. For the prolife activist, men and women have different “natural” roles in life, men being suited to the public arena and women to the private world of home and family. If women go out to compete with men, thereby violating traditional role boundaries, everyone loses. Men and children lose the nurturing that only a full-time wife and mother can provide, and women lose the protection and security provided to one in that role.
In the area of sex, prolife activists see its primary purpose as procreation: “You’re not just given arms and legs for no purpose. There must be some cause for sex, and you begin to think, well, it must be for procreation ...” (Luker, 1984b, p. 107). They are opposed to contraceptives, and many use periodic abstinence or natural methods, rejecting others on social and moral grounds.
Consistent with their views on gender and sex, the prolife activists believe that married couples should be accepting of parenthood whenever it occurs. Since motherhood is a natural role for women, a woman need not plan or prepare for it. She will “learn by doing,” and there is always “room for one more.” The idea of postponing pregnancy in favor of other goals cannot be comprehended, since motherhood is the most satisfying thing that a woman can do with her life.
The world views of prochoice activists on these issues are in sharp contrast to those of prolife women. Prochoice women reject the belief in separate domains for women and men, believing that the two genders have equal rights and responsibilities. Involuntary motherhood prevents the full equality of women with me, relegating women to a low status, unrewarded “women’s sphere,” and taking away from women the ability to choose their life’s course.
Prochoice activists attend more to the emotional qualities of sexuality in contrast to its procreative value. Sex is for pleasure, an end in itself, and it enhances human contact and intimacy. Contraception is therefore a social good, not a moral issue, as it enhances the value of sex for its own sake and frees women from the fear of pregnancy that can endow sex with negative meanings.
Parenthood, for prochoice women, is a social rather than a natural role, and should be entered only when two people are ready to be successful and loving parents to a new baby. Having children requires many resources, such as money, interpersonal skills, and emotional maturity; therefore it should be optional and planned. The elements of choice and timing make it possible to offer a better quality of life to offspring, as well as to parents.
Thus prolife and prochoice women differ sharply on important values that are central to their lives. The debate over abortion, then, is ultimately a confrontation between those women who cherish the traditional roles of a patriarchal society, because those roles are precious to them, and those women for whom traditional roles are not only irrelevant but stifling as well. Both groups of women have deeply vested interests in their chosen ways of life, and the issue of abortion is symbolic of those ways, “the tip of the iceberg,” as one said.
Having in most cases made early life decisions about the roles that children and family will play in their lives and having conducted their lives accordingly, their different stances on the abortion issue are in a sense a defense and a justification for those decisions. Prolife women, for example, having built their lives around the centrality of the family, with their reproductive capability as a valued resource, see any interference with women’s “natural” role as diminishing their value as persons. Prochoice women, who have made lifelong commitments to roles other than motherhood, resist the idea of motherhood as a primary or inevitable role for most women. They share many resources other than their ability to have children and thereby have power that has a wider base, often equal to that held by their husbands. Therefore, they can afford to believe in values that give women the ability to limit their involvement in having children, since that it what they themselves have done:
In short, the debate about abortion rests on the question of whether women’s fertility is to be socially recognized as an asset or as a burden. In a world where men and women have traditionally had different roles to play, and where male roles have traditionally been the more prestigious and financially rewarding, abortion has become a symbol distinguishing those who wish to maintain this ancient division of labor, and those who wish to challenge it. (Luker, 1984b, p. 110).
Thus, according to Luker, the debate will remain heated, passionate, and bitter. Heated, because peoples’ most cherished beliefs are called into question; passionate, because women’s lives, as well as the life of the fetus, are at issue; and bitter, because as one side gains the other loses. If society holds to its decision that a woman can choose whether or not to sustain the life that is developing within her, then those who believe that motherhood is natural for all women and that choice should have nothing to do with it lose. And if the society reverses itself and decides that the developing fetus has rights that are prepotent, and that no other role is more important than that of mother, then women who value other roles will find them devalued, since they will always be relegated to second place, or no place at all, with the advent of motherhood (Luker, 1984).
Birth Control and Public Policy: The China Example
The People’s Republic of China is an example of a developing nation that is struggling to control its population growth by implementing a rigorous policy limiting family size to one child per married couple. This one-child family program is one of the most significant social experiments ever attempted, and certainly one of the most far-reaching as well, because of the number of persons it affects and because of its impact on traditions that are thousands of years old.
China has a population of over one billion people, or 22 percent of earth’s population, with only 7 percent of earth’s arable land. About the same size as the United States, China has five times the U.S. population. China is an economically undeveloped country. About 80 percent of its people are peasants living in rural areas and engaged primarily in cultivation of the land.
Between 1949, when the People’s Republic was founded, and 1979, there was a net increase of 430 million people in China. This explosive growth was not compatible with the country’s ability to feed its people, nor with its programs of modernization intended to increase the standard of living in a land where the per capita earned income is about the equivalent of twenty U.S. dollars per month (Population Research Office, Anhui University, 1982). Consequently, in 1979 the government launched a strong birth-planning program aimed at achieving zero population growth by the year 2000 (Ching, 1982).
The elements of the program include education of the public, economic sanctions, and constant availability of free birth control methods, including abortion. Through the media the public is informed of the dangers of uncontrolled population growth, the ill effects of large families, and the benefits of having an only child. Economic rewards are given to one-child families. Couples who have only one child and who pledge not to have any more may apply for a “one-child certificate,” which entitles them to a bonus and a monthly payment until the child reaches the age of fourteen. Preferential treatment is given for housing, and only children are given priority consideration for admission to school and for jobs. When the one-child couple retires, they get an additional pension over and above what the state normally pays to retired workers. Negative sanctions apply to violators of the one-child rule. The couple may have its income reduced for each additional child and lose its extra retirement benefits (Chen, 1979).
Most of the population has access to local health stations where trained personnel provide contraceptive counseling and, increasingly, perform abortions. Contraceptive supplies and services, including the “four planned birth operations” (insertion and removal of the IUD, vasectomy, tubal ligation, and abortion), are performed free of charge. Also, benefits are paid to the person who has one of these procedures. For example, a woman may get fourteen days paid leave from work for having an abortion. (Chen, 1979).
This social program is of particular interest because of its effects in a country where government-backed drastic limitation of family size comes into head-on conflict with centuries-old traditions of large families and strong preference for sons. In spite of the present socialist government, Chinese values are still rooted in feudal ideology, which is strongly patriarchal and patrilineal, emphasizing the right of inheritance of the oldest son and the passing on by sons of the family name. When a daughter married, she moved in with her husband’s family, took their name, and became a member of their family. Thus a family without a son did not survive as a family. Since sons stayed with their own families, their presence meant not only
the survival of the family but also more hands for production, especially as they brought wives into the household, and security for their aging parents. These values survive in contemporary China, though the marriage law of 1980 states that either partner may join the other’s family, and each has the right to use his or her family name. Such innovations, however, are hardly noticeable in China today: “Despite its official status, the new law will require considerable time and effort before practice becomes widespread” (Ching, 1982, p. 210).
What happens when families want to have many children, especially sons, and the state, which has absolute power, mandates a policy of one child per family? What influences characterize those who cooperate with the birth planning policy and those who resist? One study conducted by a Chinese university found that couples who applied for the one-child certificates were better educated and had higher standards of living than those who did not hold certificates. They also were more likely to have a son for their only child. Looking at one thousand families from each category—holders and nonholders—the study found that of the 1,000 only children of certificate holders, 607 were male and 393 were female. Of the 1,000 children of nonholders, 492 were male and 508 were female. Thus parents of a male child might more easily be persuaded to apply for a certificate, while a substantial number of those with daughters might still wish to try for a boy (Population Research Office, Anhui University, 1982).
Recently, reports of much more ominous consequences of its birth planning policies have emerged from the People’s Republic. While public statements indicate that compliance is won through education, persuasion, and voluntary consent, some observers report a high incidence of coercion, including forced sterilizations and abortions, and female infanticide, the killing of unwanted female infants (Weisskopf, 1985).
Every Chinese belongs to a unit, such as a workplace or rural governing body, and each unit has a birth control committee headed by Communist Party officials. These officials have power over important decisions, such as allocation of bonuses, housing, and advanced study, and regulation of marriages and childbearing. These local officials earn cash bonuses only if their units stay within their quotas for births. Thus couples who want to have a child must make written application, and requests are matched with the government-mandated quotas.
Couples with two or more children are targets for special attention. One parent is required by the state to be sterilized, and four out of five of those who submit are women. In rural areas, “high tides,” or roundups of women of childbearing age with two or more children, result in mass sterilizations by roving surgical teams. Ln one instance, such a team performed sixteen thousand sterilizations in two months. Women who try to evade the surgery are subject to severe penalties: loss of their job or land allotment, cash fines, or confiscation of their family goods. “Who dares to oppose the regulation?” asked one woman. “I have three children. Can I afford to feed them without a job?” (Weisskopf, 1985, p. 8).
One-child mothers are required by national regulation to have IUDs inserted after their child is born. These may be implanted without informing the woman in advance or receiving consent. Women often have the devices removed surreptitiously, sometimes at the cost of injury or death caused by the perforation of the uterus by unsterile instruments (Weisskopf, 1985).
As late as the 1950s abortion in China was punishable as murder. But in a country so threatened by overpopulation, abortion is no longer a moral issue. In 1984 nearly nine million Chinese women had abortions, terminating one out of every three pregnancies (United Press International, Nov. 24, 1985).
Any mother of one child who becomes pregnant again without authorization is supposed to have an abortion. Birth control activists, under the auspices of party officials, closely monitor the reproductive status of women in their units, reminding pill users to take their pills, issuing condoms, keeping track of menstrual periods, and watching for early signs of pregnancy. If a woman is suspected of being pregnant, she is ordered to take a pregnancy test. A positive test calls for an abortion if she already has one child. She may be offered a cash bonus ‘or time off from work if she has an abortion. If she refuses, the pressures begin.
The first level of pressure consists of visits by the activists, who urge the woman repeatedly to have an abortion as her duty to society. Relatives may be eniisted to strengthen their arguments. If the woman resists, local officials appear, warning her of the penalty for an unauthorized birth: possible loss of land and job, public censure, and the denial of benefits to the child. In some areas she is charged a daily “talking fee” for these visits, and in the fourth month fines of up to 50 percent of the couple’s monthly wage begin, to be refunded if she has the abortion (Weisskopf, 1985).
Sometimes women run away to the mountains or hide with relatives until the child is born. In one commune in a southwestern province, a twenty-nine-year-old woman named Meng traveled two hundred miles to have her second child at an aunt’s house. The commune party chief took revenge when she came home. Her family lost half their land; she was fined thrice her annual income; and the child was denied food and clothing rations. She was also forced to stand before one hundred peasants and make a self-criticism, a severe loss of face to Chinese. “Since then,” said the party chief, “we haven’t had an unapproved second birth” (Weisskopf, 1985, p. 8).
An important part of Chinese tradition is exemplified in a Confucian saying: “There is no behavior more unhlial than to have no male descendants.” Because of the very strong preference for sons among the Chinese, many believe that if they can have only one child it must be a son. This has led to the widespread practice of female infanticide, the abandonment or murder of female infants. While the Chinese government has published no statistics on infanticide, analysis of 1981 census data by Western demographers found an unusually high infant sex ratio of 108.5, compared to China’s earlier norm of 104.[38] Furthermore, a Chinese survey of sex ratio by birth order for the same year found that for firstborns the sex ratio was below the world norm of 106 but rose to 115 for secondborns in cities (Weisskopf, 1985), In some rural areas, according to surveys by the All-China Women’s Federation, boys under the age of five outnumber girls by a ratio of five to one (Parks, 1983).
The government condemns female infanticide and has permitted stories about it to appear in newspapers, hoping to influence public opinion to view it as unacceptable and to come to the recognition that girls are as valuable as boys are. But few cases are prosecuted and local officials often look the other way, especially in rural areas where the need for sons is seen as critical both for family productivity and for old age security, in a land where most cannot look forward to retirement pensions and old peoples’ homes.
Thus many baby girls are sacrificed. According to a Canton newspaper, in some villages a bucket of water was kept beside the bed of a woman in labor. If the infant was a girl it was drowned immediately. Corpses of abandoned girls had been found in streams, caves, Helds, and public toilets (Parks, 1983). Women who have access to hospitals often undergo amniocentesis, a test that can determine the sex of the fetus. Female fetuses can then be aborted, and the woman can try again for a son.
Failure to have a son can have serious consequences for a woman. In earlier times a woman could keep trying until she produced a son. Today that is not possible. In spite of the fact that it is the male-produced sperm that determines the sex of the child, a woman who has a daughter may be punished both mentally and physically. A transportation worker in Shenyang was beaten by her husband for having a girl. Later she attempted suicide by lying on a railroad track. When she was rescued in time, her mother-in-law said to her, “If you want to die, go drink DDT. For everyone like you who dies, there is one less to worry about.” A few days later the woman took her life by drinking the insecticide (Weisskopf, 1985).
Though the Chinese government is attempting to enforce its laws against infanticide and has mounted an extensive campaign to change public attitudes about the value of sons and daughters, it seems obvious that the battle to preserve female lives will be a long one, and that there are no easy answers. Population growth must be brought under control, and measures have been put in place to reach this goal. These measures, however, run counter to old traditions of male dominance and to grim realities of survival. The result of the clash is a great loss of female life and the degradation of women who bear daughters.
Birth Control: A Woman’s Right
The availability of safe means for limiting fertility and the legal right to use them are probably more important than any other agents of change during the long course of women’s history. All the evidence indicates that healthy women are in no way harmed by being able to choose whether or not they wish to have a child. Since the widespread use of reliable contraception and the availability of abortion are still less than a generation old, the full effects of chosen motherhood as a matter of course on women and on whole societies will be more apparent in the future. In the meantime, most women want to experience, at least once, woman’s oldest role. The events leading up to the role of mother and their psychological effects are the subject of the next chapter.
9. Pregnancy ana birth
It cannot be argued that childbirth is both an unbearable pain and a bearable pain, both a situation from which all women naturally shrink in dread and a situation towards which all women move readily and happily, both as a danger to be avoided and a consummation devoutly to be desired. At least one aspect must be regarded as learned, and it seems simpler, in the light of present knowledge to assume that women’s attitudes towards childbearing and men’s attitudes towards childbearing have complex and contradictory elements in them....
—Margaret Mead, Male and Female, 1949
Pregnancy and childbirth are turning points in a woman’s life. Variously described in terms ranging from peak experience to utter despair, the experience of bringing forth a child has no equal. Its implications, especially for the first, will change her life forever. Attitudes toward woman’s reproductive status and capacity are characterized by ambiguity. Her fecundity has been seen as analogous to earth’s own regeneration and has inspired the creation of religions and the worship of goddesses in her image. But in recent times her fertility has become problematic as pressures increase to limit population growth. Toward the pregnant woman herself, attitudes are complex and contradictory. She is seen as strong in the fulfillment of her fertile self, yet frail and vulnerable at the same time (Graham, 1976). She is sentimentalized in her role of impending motherhood, yet stigmatized in subtle ways for her visible pregnancy. She is accommodated with attention and special privileges in social situations, but discriminated against in employment and public life (Leifer, 1980). It remains to be seen how these contemporary attitudes about woman’s primary biological function will affect her future status. But clearly the role of woman is changing rapidly in response to demands for equal opportunity to participate in all the goods and activities of the society. Women now are in a stronger position to choose the number of children they want, if they want any at all.
Concern about population growth has generated interest in factors that influence family size. Advances in birth-control technology and the increasing availability of information and family-planning services have only recently provided alternatives to the traditional destiny of women ordained by reproductive capacity. But visions of a brave new world made possible by technology have had to be tempered on more than one front by the sobering recognition that traditional behaviors which come to be seen as hostile to broad social interests may continue in spite of the recommendations of social planners. The availability of the technological means to avoid or to safely terminate pregnancy, for example, does not necessarily lead quickly to results in all affected segments of the population. Reproductive behavior, because of its unmatched importance in the life of the species and of the individual, is a function of accretions of values, beliefs, and attitudes which powerfully affect the ways it will be played out or modified. A change in extrinsic mitigating circumstances inevitably meets resistance from covert motivations which may be difficult to identify or to change. The experience of the woman in all societies has always included the bearing and rearing of children, and thus her performance of and identification with these functions has shaped her concept of herself as a woman and as a human being and has determined in a real sense her value, whether she lived in a palace, a harem, or the slave quarters of a plantation.
Motivations for Having Children
In spite of the decline in the birth rate in recent years, there continues to be a strong and widespread desire for children among couples in the United States. Only 5.4 percent of married women expected to remain childless (U.S. Census Bureau, 1978). One-half of married couples wanted two children, while 15.8 percent wanted four or more. In a later study, college undergraduate women expressed the desire to have between two and three children, and only 9 percent wanted none at all (Gerson, 1980).
At one time, children were an economic asset to the family, but now they represent a financial drain. In addition, they have other important negative consequences such as loss of freedom and worry and concern for parents. Considering all of this, the motivation for having them must be very strong.
Understanding of variations in fertility rates and in cultural and historical trends is facilitated by examination of the possible value of children to parents, particularly to women. A theoretical model for studying such variations included the value of children as one of its elements (Hoffman and Hoffman, 1973). In this system the ways in which children are valued are related to psychological needs that are influenced by the society and thus are subject to cultural variation. These needs all have the potential of being satisfied by some aspect of parenthood, though alternative means of satisfying them are possible.
For a woman, having a child is one way of attaining adult status and identity. The responsibility for new life is expected to elicit mature and conscientious behavior. A new identity emerges: one is now Mother, which is more than just a name. This identity implies a whole new and lasting set of duties, commitments, and values, not the least of which is a new sense of being important, of being truly necessary to another person.
Children are often valued as an expansion of the self, as permitting oneself a kind of immortality. Two persons become three, or five or more, providing a bridge to the future by which one’s physical and psychological characteristics can continue beyond the evanescent self.
Values associated with morality encourage the production of children in some groups. Catholics, for example, are enjoined against the use of birth control on religious grounds and tend to want more children than Protestants do (Rainwater, 1965). The Judeo-Christian tradition clearly viewed having children as a moral duty and barrenness as a curse. Altruistic needs are served by the sacrifices required by parenthood. Lack of interest in having children is often seen as selfish, a sign of unwillingness to share one’s time or goods, whereas the willingness to endure the difficulties, suffering, and sacrifice involved are seen by some as evidence of strength of character, integrity, and other cherished values of American society.
Children make a family and thus supply primary group ties through which affiliative needs can be met. They can add stimulation, novelty, and fun to a household. As they grow and change they provide a continuing challenge to parents who want to experience them and to understand them. The expectation of a new baby is fraught with mystery and anticipation. “Each one is different,” mothers say. Studies of the values of having children find that parents related feelings of joy, and describe their children as a source of happiness to them.
Parents of all social classes report feelings of creativity, accomplishment, and competence from the experience of having and rearing children. A woman with several young children may have few other ways to demonstrate competence and to win recognition; thus the observable results of her skills in this area can give her a deserved feeling of achievement. For the mother especially, having one or more children gives her a degree of power, the ability to command service or concessions from others that she would otherwise not have. Children are also seen as a chance to have an effect on the world, particularly by persons who are otherwise powerless. For persons who are disadvantaged in the population because of race or social class, or for women of all classes, a baby holds forth the chance of making a difference. Having a baby is something one can do.
The economic value of children varies greatly from one society to another. In developing countries with rural, subsistence economies, children provide valuable work when they are young, and later they give care to aged parents. In the United States, however, the economic value of children is very low, as in all industrialized countries with higher standards of living, child labor laws, and compulsory education.
Given these values associated with having children, is it possible to predict a person’s or a group’s desire for children? There are four motivational variables whose relative strengths are determinants of the desire to have or not to have a child: alternative sources of the value, costs, barriers, and facilitators (Hoffman and Hoffman, 1973). Alternatives are other means besides children for actualization of a value. For the woman, a career and the independent life style it affords can serve many of the same values associated with having children. The availability of such alternatives could be expected to affect the number of women desiring children, as well as the number of children desired by individual women. Costs pertain to how much one must give up or sacrifice in order to obtain the values associated with having a child. For example, freedom of activity and flexibility of one’s personal schedule are drastically reduced when one has small children. Barriers and facilitators are the factors which realistically lower or raise the probability that the value can be realized by having children. For example, the prevailing belief that having more than two children is inconsistent with genuine concern for the future of humankind is a barrier, while the desire of one’s parents for a grandchild is a facilitator.
Even though alternative sources of gratification are increasingly available for women, and the costs and barriers seem to outweigh the facilitators, there is no evidence that even a high-status, interesting career is a completely adequate substitute for having children. Even though the seventies brought a dramatic shift in family size aspirations of college women, most still planned to have children. The “lure of motherhood,” the expressed desire to have children, is related to several factors. Unique psychological variables include positive memories of early childhood maternal love. Women with traditional gender-role identification and antifeminist attitudes also are more likely to desire children, and women from large families express more desire to have children than do women from small families (Gerson, 1980).
I he reproductive events leading up to motherhood not only define the major experiential differences between women and men, but because of the dramatic and compelling nature of both their biological and psychological effects, they have a profound impact on any women who experiences them. Men themselves have never been indifferent to the procreative power of women, reacting not only with wonderment and envy, but even with vicarious participation, taking on the very identity of woman as she moves through the reproductive process. In the next section we shall review the biological sequence leading to the advent of a new life, and then consider some psychological and behavioral factors that are relevant to pregnancy, childbirth, and breast-feeding.
Pregnancy
The average duration of human pregnancy is 266 days, or nine months, although premature birth is not uncommon, and much longer pregnancies have been recorded.[39] Obstetricians think of pregnancies in terms of trimesters, or three-month periods. Each trimester has its characteristic features in terms of both the experiences of the mother and the development of the fetus. Our discussion will focus primarily on the experiences of the mother.
The first sign of pregnancy is usually a missed menstrual period, an event which is unlikely to be viewed with equanimity by any woman, whether joyous or distressed at its possible meaning. Failure to menstruate can be caused by other factors, however, such as psychological stress or malnutrition. Also, it is not uncommon for cyclic bleeding to persist during the first months of pregnancy, so that presence or absence of the menses is not always a reliable indicator. By the eighth week, the pregnant woman will begin to have other signs. Responding to greatly increased levels of estrogen, the breasts become somewhat enlarged and tender, and the woman experiences feelings of fullness and tingling with increased nipple sensitivity. “Morning sickness” or nausea, sometimes accompanied by vomiting, occurs in about 75 percent of pregnant women during the first six to eight weeks. Although this symptom has been widely held to be psychogenic, the present tendency is to view it as a physical consequence of hormonal changes, inasmuch as it also occurs in women receiving estrogen therapy and is a common side effect of the oral contraceptives containing estrogen. Other signs of pregnancy in the first weeks are increased frequency of urination, unusual sleepiness or fatigue, and deeper pigmentation of the nipples.
Having missed a period, many women wish to know as soon as possible whether or not they are pregnant, especially if they are contemplating an abortion. Endocrine tests have been developed which can accurately diagnose pregnancy from two to six weeks after the first missed period. The most popular of these is the agglutination test which relies upon the presence in the pregnant woman’s urine of a hormone secreted by villi protruding from the implanted fertilized ovum. A sample of urine is mixed with chemicals. If agglutination (clumping) occurs the woman is not pregnant. This test will detect pregnancy two weeks after the first missed period with about 97 percent accuracy. Simple-to-use home pregnancy tests are available in drugstores and will detect pregnancy with about 97 percent accuracy nine days or more after a missed period. Negative results at this stage are about 80 percent accurate, though the accuracy rate rises to 91 percent a week later (Shephard and Shephard, 1982).
A physician can usually diagnose pregnancy by examination at about the sixth week. By this time the uterus has increased slightly in size and the cervix has softened considerably. The physician will look for “Hegar’s sign,” a soft consistency of the area between the cervix and the uterus, which can be felt on pelvic examination. Even without endocrine tests, these changes together with some or all of those previously mentioned in a sexually active woman are usually considered as rather firm evidence of pregnancy.
Very early in the Erst trimester, the placenta, the organ which supports the life of the fetus, begins to develop from both fetal and maternal tissue. Sometimes called the afterbirth, it is a large, flat mass of vascular tissue which is connected to the fetus by the umbilical cord. The placenta mediates, in a sense, between the fetus and the mother. Through it pass oxygen, nutrients, and waste materials, as well as certain antibodies, drugs, and other materials which may be beneficial or harmful to the child in utero. The placenta has effects upon the mother too. It functions as an endocrine gland, producing a variety of hormones all during the pregnancy. One of these is human chorionic gonadotropin (HCG) which assists in the maintenance of the pregnancy by stimulating the continued production of progesterone during the Erst trimester. The placenta itself secretes large quantities of progesterone and estrogen until just before the onset of labor. The sudden decline in the level of these hormones is believed to cause labor to begin. Other hormones produced by the placenta prepare the mammary glands for lactation, the process of secreting milk. These hormones also inhibit the pituitary gland from releasing the actual milk-forming chemical until it is needed.
Miscarriage, or spontaneous abortion, is most likely to occur during the first trimester. An estimated 10 to 15 percent of all pregnancies end in miscarriage, and most of theSe happen before the fourteenth week. Although miscarriage may be caused by physical trauma or by illness of the mother, in most cases the reasons are not known. About half of all miscarried fetuses are defective in some way.
The second trimester brings abundant evidence to the woman of the dramatic changes in her body as a result of her pregnancy. Confirmation of the pregnancy can now be made by physical signs alone. The physician can monitor the fetal heartbeat, and both can feel the movements of the fetus, which by the end of the sixth month, is about fourteen inches long and weighs about two pounds. The waistline of the pregnant woman thickens, and her abdomen begins to protrude; she is recognizably pregnant. Many women experience this period as the best time of their pregnancy. Most of the earlier symptoms have ameliorated or disappeared, and the woman is usually quite able to continue with her normal activities, barring complications. Many women experience feelings of serenity and well-being during this time, probably as a combination of attitude toward their condition and their high estrogen level.
Certain hereditary and biochemical defects of the fetus can now be detected during the second trimester of pregnancy by a procedure called amniocentesis. Fetal cells are obtained by tapping the fluid in the sac surrounding the fetus. These cells are cultured, and from them information can be derived on the child’s chromosomes and cell biochemistry. The test has been used successfully to diagnose Down’s syndrome, adrenogenital syndrome, and Tay-Sachs’ disease,[40] among others. The value of amniocentesis in genetic counseling was demonstrated in one study of fifteen women with a 25-percent risk of delivering a child with Tay-Sachs’ disease. Six cases of the disease were diagnosed; five were confirmed in the fetus after therapeutic abortion, the other after birth (O’Brien et al., 1971). In another study of one hundred fifty pregnant women the test showed that the fetuses of fourteen had chromosonal disorders. Abortion was requested by thirteen of the women, and in each case the diagnosis of some chromosomal disorder was confirmed upon examination of the aborted fetus. The fourteenth woman delivered a child with Down’s syndrome (Nahum, 1970).
During the last three months the fetus grows very rapidly and is quite active, kicking, twisting, and turning, its vigorous movements sometimes interfering with the mother’s sleep. Weight gain can be a problem during this trimester, when appetite increases and activity level usually slows. A weight gain of about twenty pounds is considered optimum for a full-term pregnancy, though many women may gain more or less than this and be perfectly healthy. The baby at birth accounts for about a third of this weight. Two or three more pounds will be lost at birth with the placenta and the amniotic fluid. The remainder results from enlargement of the uterus and breasts, and from retained fat and fluids.
About 7 percent of babies born in the United States are premature. Prematurity is a function of the weight of the baby, not of the length of the pregnancy. An infant weighing less than five and a half pounds at birth is considered premature. The less the infant weighs, the poorer its chances for survival. Babies who weigh less than four pounds at birth often develop fatal respiratory difficulties. In addition, premature babies who survive are more likely to have congenital disorders such as mental retardation and brain damage. With today’s modern pediatric care, however, even babies who are born very small have a good chance to grow into normal healthy childhood (Macfarlane, 1977).
During the seventh month most babies move into a head-down position in the uterus. This is the most common birth position and is the most free from complications. A few remain upright in the so-called breach position, and some turn sideways in their orientation to the birth canal. Both these last positions can result in more difficult deliveries. But about 97 percent of full-term babies have turned to the head-first position.
Childbirth
Until the middle of the nineteenth century, in America the delivery of the child was exclusively the province of women. During labor and delivery and for the period of “lying-in” that followed, women were attended by female relatives and friends, and usually by a midwife as well, a woman whose work it was to minister to women who were giving birth, and often to perform other household services as well. Sometimes a mother or other female relative of the expectant woman would stay with her for several weeks before and after the birth, so that she could remain in bed, initiate the nursing of the baby, and be free of the care of other children and the household until she had regained her strength. The practice of women attending each other made of the birth a social event, an occasion for female solidarity (Wertz and Wertz, 1979).
As the profession of medicine began to be organized and practiced, physicians, almost all of whom were male, included the delivery of babies as one of their services. As American women increasingly chose them to deliver their babies, birth was transformed from a social event to a medical event and came eventually under the control of the medical profession. The event of birth moved from home to hospital; whereas in 1900 less than 5 percent of women delivered in hospitals, by 1939 half of all women and 75 percent of urban women had hospital deliveries (Wertz and Wertz, 1979). Anesthesia began to be widely used to ease the pains of birth. Numerous interventions were developed, such as the use of forceps to pull the child from the birth canal. Caesarian deliveries became common, as birth was defined as a pathological process, with only a small minority of women capable of having a normal, problem-free delivery. As one writer in a medical journal put it:
It is a common experience among obstetrical practitioners that there is an increasing gestational pathology and a more frequent call for art, in supplementing inefficient forces of nature in her efforts to accomplish normal delivery (Ritter, 1919).
As we shall see later, it is only in the last few years that aspects of the medical model of anesthesized, hospitalized birth have been challenged. So far that challenge has affected only a small number of women, though its repercussions have had their effects on traditional practice to some extent—in the direction of making it a less alienating, more human experience for the woman and her family.
Cross-cultural attitudes and practices
Labor and birth are subjects of widely varying beliefs, attitudes, and practices around the world. While this discussion of the reproductive events in women’s lives is primarily from the perspective of our own society, we should be aware that these experiences are patterned in very different ways in other societies. An appreciation of this basic fact can give perspective on our own practices and show the effects of social forces on the conduct of these natural biological events.
Patterns of behavior have been related to birth in nonliterate and traditional cultures, using both medical and anthropological sources (Newton and Newton, 1972). First, the attitudes surrounding the birth experience, such as privacy and sexual implications, achievement connotations, “dirty” or defiling effects, and the attitudes toward birth as a painful illness or as a normal process were examined. Second, practices in the conduct of labor and birth which result in different sorts of experiences for the mother were studied.
While all the cultures placed great importance on the phenomenon of birth, they varied greatly in their attitudes toward specific aspects of it. For example, the Navaho were very much interested and very open in their observance of birth, moving freely in and out of the hogan where a baby was being born and partaking of food and drink provided there. Others, such as the Cuna of Panama, surrounded birth with secrecy, concealing facts about it from children as long as possible, preventing them even from seeing animals during labor or birth.
In contrast to our own society, where the birth is often seen as an accomplishment of the obstetrician, the Ila of Northern Rhodesia shout praises of the woman who has given birth. Her husband and male relations give her gifts and congratulate her. Other groups feel that birth is a “dirty” process which defiles and contaminates both the woman and those who come in contact with her. For example, among the Kadu Gollas of India the laboring woman is isolated in a hut and is impure then and for three months after delivery. She and the child may not go home until permitted to do so by the deity.
People in many parts of the world view childbirth as a normal and even casual procedure, experienced with little apparent discomfort. Others combine an expectation of intense pain with strong social sanctions against crying out since such a display brings disgrace on the woman. The Aranda of Australia report pain only at the onset of labor, but make “little fuss” during the rest of the process.
There is also a great variety of practices in the conduct of labor. Food and drink may be prohibited or freely given to the woman in labor. She may be required to lie down or to stay in one place, or encouraged to walk about and actively exercise. While most births are social acts, occurring in the presence of others, a few are unattended by any other person. In almost all nonliterate groups, birth is women’s business, and men are excluded. The delivery itself occurs in many different positions. In contrast to the usual supine position familiar to Americans, a survey of seventy-six non-European societies found that sixty-two used upright positions of kneeling, sitting, squatting, or standing, or combinations of these (Newton and Newton, 1972).
In looking at other ways of feeling and behaving, we can perceive and react to our own ways more clearly. Our society’s attitudes and practices about childbirth are always changing, and some of the changes reflect lessons learned from people from other cultures.
Labor and birth
The onset of labor is triggered by hormonal changes resulting in the disinhibition of oxytocin, a pituitary hormone which is believed to initiate the contractions of labor and delivery. The entire process of childbirth, called parturition, occurs in three stages. The Erst stage begins with the earliest signs of labor and ends with the full dilation of the cervix. As a woman approaches the end of her pregnancy, she may experience back pains and irregular contractions of the uterus. Many a woman has gone to the hospital with such “false labor,” only to return home and wait another few days or weeks. Several signs suggest that labor is imminent: regular uterine contractions at intervals of fifteen or twenty minutes, lasting about thirty seconds, mild and rhythmic in the beginning, and later increasing in frequency, intensity, and duration; the expulsion of the cervical plug, which appears as blood-tinged mucus; and the rupture of the amniotic membrane, or “bag of waters,” which produces a clear fluid from the vagina.
By the time the cervix is fully dilated, which may be twelve to sixteen hours for first births, the woman is experiencing contractions every three to four minutes each lasting for about a minute. The powerful muscular walls of the uterus push the baby downward toward the birth canal. At about this time the woman is likely to be taken to the delivery room.
The second stage of labor begins with the full dilation of the cervix and concludes with the expulsion of the fetus from the mother’s body. Powerful uterine contractions stimulated by the pituitary hormone continue to move the baby along the birth canal until its head is visible at the vaginal opening. In order to accommodate the passage of the infant’s head and shoulders, which are the largest parts of its body, the opening of the vagina must stretch tremendously. In order to avoid tearing of the tissue between the vagina and rectum, the physician may perform an episiotomy, a surgical slit which is stitched after the birth and heals within a few days. Also during this period the mother is now instructed to push, or to bear down, to facilitate the emergence of the baby from her body. Once the head and shoulders are born, the rest of the body appears quickly. When respiration and independent blood circulation have been established in the infant, the umbilical cord is cut and clamped.
The third stage of labor consists of the delivery of the placenta, which separates from the uterine wall and moves out of the vagina a few minutes following the birth of the baby. Muscular contractions shrink the uterus and facilitate the detachment of the placenta. If an episiotomy was performed, it is now repaired with catgut stitches. This incision heals rapidly, after a few days of mild discomfort and itching.
In a typical hospital delivery, the newborn infant may be handed to its mother (and father if he is present) for a few minutes, then weighed, measured, and taken to the nursery. Sometimes the parents have the baby with them for an hour or so immediately following its birth. This is now believed to facilitate a special attachment between the parents, especially the mother, and the baby.
In some hospitals, delivery room practices are becoming more humane, structuring the event around a more holistic concern for the individuals involved rather than as an exercise in medical technology. An example is Dr. Frederick Leboyer’s advocacy of “birth without violence,” based on his belief that birth is a traumatic ordeal for the infant and that its entry into the world should be as gentle and soothing as possible. Instead of the usual bright lights, noises, and less than gentle handling that characterize the traditional experience of the neonate, Dr. Leboyer advocates a quiet, semi-dark room. When the baby is born, it is placed immediately on the mother’s body so that she can massage it gently as it takes its first breaths. Then it is placed in a basin of warm water, a simulation of the uterine environment (Leboyer, 1975).
Preparation for Childbearing
In contemporary society many young women grow up with little or no exposure to the verities of childbearing. Smaller families, the decline of the extended family, and the increased mobility of young married couples make it less likely today than in the past that a young woman will be near her mother, older sisters, or other supportive friends and relatives who, though often misinformed, can often give emotional support and offer examples to her as she approaches labor and delivery. As the setting for birth moved from the home into the hospital, it became ever more impersonal and removed from daily life. Women had few sources of information about what to expect when their time came, except for the often terrifying accounts of others. Most hospital births in the first half of the century took place with the mother under general anesthesia, so that many women had no recollection of the experience at all after the first stage of labor. A new mother would not see her baby for hours after its birth, when it would then be brought to her every three or four hours for feeding. There was little opportunity for the mother, and even less for the father, to become acquainted with the baby and to begin to feel comfortable with it before the trip home. Also, hospital stays of ten days to two weeks were common, disrupting family life, especially if there were other children at home, and making the hospital-to-home transition even more difficult.
In contrast, today’s practice in this and other Western countries provides women with the option of another kind of childbirth experience which includes instructional preparation for both the woman and her husband, his presence at the delivery, minimal or no anesthesia to allow for her full participation in the birth, and immediate contact with the newborn, sometimes continued with the rooming-in of the baby with its mother during the hospital stay. The rationale for this kind of experience includes reduction of pain and anxiety for the mother, elimination of risk to her and to the infant from the use of conventional anesthesia, and the psychological benefits derived from sharing the event with her mate. Advocates of roomingin also point out that the parents have a chance to become acquainted with the baby before they are confronted with the sole responsibility for it at home.
The Read and Lamaze methods
Two kinds of preparation for childbirth are growing in popularity in this and other countries. Called the Read method and the Lamaze, or psychoprophylactic (PPM) method, they and variants and combinations of the two are variously referred to as “prepared,” “participatory,” or “natural” methods of giving birth. The term “natural,” while older than the others, has fallen into disfavor because of its implications that other methods, particularly those in which anesthesia is used, are unnatural. Neither the Read nor the Lamaze method precludes the use of anesthesia, although the mother’s full, conscious participation in the birth is a key element in the training of both methods.
The Read method was introduced by the English physician Grantly Dick-Read through his book Childbirth Without Fear (1944). The theoretical basis of the Read method is the elimination of the vicious circle of fear-tension-pain-fear which is the result of ignorance and anxiety about the process of labor. Fear of anticipated pain causes contraction of the uterine muscles, creating a resistance against cervical expansion. The resultant tension state, according to Read, is interpreted by the woman as pain, which increases her fear and tension and augments the pain. The method prevents this cycle from getting under way by focusing on the reduction of both fear and tension. Through learning about the phenomena of pregnancy, labor, and delivery, she loses her “unreal” superstitious fear of the unknown. Beginning about the fourth or fifth month of pregnancy, she is trained in techniques of muscular relaxation, on the theory that if she can completely relax, she will not “fight” against the uterine action, thus permitting the cervical stretching and uterine muscular activity to effect an unimpeded and relatively painless delivery. Deep chest breathing and muscular exercises help the woman to achieve a state of relaxation during labor.
The Lamaze method was first developed in Russia, and was brought to France by the French physician Fernand Lamaze and popularized in the United States by Marjorie Karmel’s book Thank You, Dr. Lamaze (1959). This method is based on Pavlov’s conditioned-reflex work and relies upon re-educating the woman to dissociate pain sensations from labor. Any implication that uterine activity in labor is painful is avoided, and other physiological responses are conditioned to the sensations of labor so that these are not experienced as pain. These include rhythmic breathing or panting and abdominal effleurage (moving the fingers over the abdomen in a light, circular motion). Women are taught the physiology of labor and delivery and are trained to be aware of their body sensations in labor so that they can adjust their breathing and pushing activities accordingly. While both the Read method and the Lamaze method have in common the twin aims of educating the woman for childbirth and reducing or eliminating pain so that she can be conscious during the birth, they differ in that the Lamaze method actively engages the woman in the labor process while the Read method emphasizes relaxation and dissociation from body processes. Both methods and their variations stress the participation of the husband in both the training and the labor and delivery.
Many enthusiastic claims have been made by women who have had a childbirth preparation course. Lamaze training was related to participants’ postpartum recall of experiencing feelings of mastery, personal control, and coping power during labor (Oliver, 1972). In another study twenty-two women who took a childbirth course were compared with fourteen who had delivery by conventional methods. Pain reduction was a joint product of taking the course and having a good menstrual history (Tanzer, 1973). In addition, women whose husbands were with them at delivery were more likely to describe it as a “peak” experience, a rapturous gratification of emotional needs.
Benefits other than psychological have recently been shown to be associated with Lamaze training. In the most comprehensive study of its kind, five hundred Lamaze births were compare to five hundred other births to women of similar ages, races, educational backgrounds, and health conditions. The Lamaze mothers had only one-third as many cases of toxemia, post-delivery infection, and breech delivery as the other women in the study. They had one-fourth as many Caesarian deliveries, and one-fifth the amount of fetal distress. While the reasons why the Lamaze mothers had more nearly problem-free deliveries are not clearly understood, it does appear that the method helps to effect more healthful birth experiences for women, in addition to easing the anxiety and pain traditionally associated with childbirth in Western society (Spokeswoman, July 15, 1978).
Meanwhile, an extensive review of the psychological mechanisms believed to be related to the efficacy of Lamaze training noted that many of them have been shown to reduce anxiety and distress in a number of medical and nonmedical situations. Social support, for example, is a prominent feature of Lamaze in the role of the husband-coach and in the group setting of the training. Social support has also been found to have an ameliorative effect on risk for mental illness as well as for physical illness (Wideman and Singer, 1984). Thus it is possible, even probable, that Lamaze techniques are not specific to childbirth preparation, but also have applications in behavioral medicine in general.
In any case, the Lamaze method has effected major changes in hospital birthing practices. A survey of four hundred U.S. hospitals found that almost all the obstetricians connected with them encouraged Lamaze preparation for their patients. Ninety-nine percent of the hospitals allowed fathers to be with mothers in the labor and delivery rooms, and 89 percent allowed persons other than the father into these areas. The survey found that Lamaze training was used throughout the United States without regard to income level, ethnic origin, or socioeconomic status of the participants (Wideman and Singer, 1983).
Since neither the Read nor the Lamaze method precludes anesthesia if the woman wants it, and since both result in a more knowledgeable participation in the childbearing process, it is difficult to see how the various components of the training could result in a worse experience than the woman would have had without them. Certainly, the informational aspects of the program and the rehearsals for labor seem to reduce the fear of the unknown and the sense of helplessness and isolation for first-time mothers and to give the father a more intimate role in the bringing forth of the child.
Alternative experiences in childbirth
Since the early 1970s, the feminist movement and consumer activism have challenged traditional methods of providing care in the birthing process. Women began to call attention to the fact that pregnancy and birth are natural processes that intimately affect the family. Many wished to share the event of birth with family members in a warmer more personal environment than the traditional hospital allowed. To meet these needs, many hospitals now provide birthing rooms for women who want to use them. Birthing rooms are informally furnished and decorated, much like a bedroom—sitting room. The mother-to-be stays in this room for both labor and delivery, the father staying with her throughout. In some instances, other family members may also be present, at the parents’ option. Some traditional procedures, such as enemas and episiotomies, may not be performed. Frequently mother and baby remain only a few hours after the birth, leaving for home if all has gone well (Shephard and Shephard, 1982).
During the 1970s, some women began insisting on returning the event of childbirth to the home. They preferred to have their child delivered by a midwife. This was in contrast to the prevailing medical model whereby the woman is hospitalized and the birth treated as a surgical procedure rather than as a natural event. In the United States most babies are born in hospitals, but in many other industrialized countries, the physician-attended hospital birth is not the norm. Babies are much more likely to be born at home or in maternity clinics, attended mostly by nurse-midwives. In the Netherlands, for example, 50 percent of all births occur at home, and most are attended by midwives (Macfarlane, 1977).
In the United States women who wish to give birth at home usually turn to midwives for prenatal care and delivery, since physicians are usually unwilling to deliver babies outside the hospital. About two-thirds of the states have licensing laws regulating the practice of lay- and nurse-midwives, though together they account for less than 1 percent of all births each year (Wertz and Wertz, 1979).
Women who have their babies at home with the assistance of midwives give several reasons for their unorthodox choice. They want the birth to be a family event with the husband in attendance. They want a more relaxed atmosphere, in which they are in control, in the familiarity of their own home. Many feel that the midwife is more patient, more gentle, more willing to wait for nature to take its course. They cite the few available studies which show that having a baby at home is at least as safe, if not more so, than having one in the hospital. Finally, it is far less expensive, though this reason alone is not an important motivator. Physicians, by contrast, are more likely to cite the possible risks of home births for mother and infant, should emergencies arise during the labor and birth process. Also the hospital, with its equipment and routines for medical procedures, is far more convenient for the medical staff. Perhaps a combination of the best features of home and hospital deliveries, as in the maternity clinics of some European countries, would effect a more humane, less alienating environment for the occurrence of birth.
Feminists, however, see the renewed interest in home birth and midwifery as women’s retrieval of something that had always rightfully been theirs but had been lost: the control and celebration of their own bodies, especially as they labor and bring forth- life.
Effects of Maternal Behaviors
Can the emotions and behavior of a pregnant woman have an effect upon her unborn child? A few years ago such a suggestion would have been dismissed as an old wives’ tale, but contemporary research responds with a qualified affirmative. Several studies have found a relationship between the mother’s emotional state during pregnancy and the infant’s well-being and progress during the first few months of life. One study investigated the psychological adjustment during pregnancy of 177 women and found that among the multigravidae (women who had given birth before) those expressing more fears for themselves and their babies, and more tension, depression, and withdrawal, had babies who weighed less at birth and had a lower Apgar score than did those women not so affected (Erickson, 1965).
A Japanese study reported on maternal emotional characteristics and body-weight gain of infants in the early neonatal period (Murai and Sato, 1971). Babies whose mothers had scored high on tests of hypochondria and neuroticism during the second trimester showed inferior weight gain compared to babies whose mothers had scored in the normal range. The results suggested that emotional stress during pregnancy has a biological influence on the fetus, causing retardation of weight gain after birth. Another study revealed that experimentally induced stress could cause intense uterine contractions in pregnant women. The damage from psychological stress was thought to be a contributor to the higher incidence of stillborn babies among illegitimate, as compared to legitimate, births (James, 1969).
Infants born to mothers who were schizophrenic during pregnancy were compared to infants whose mothers became schizophrenic postpartum and to infants whose mothers had a physical illness (Yarden and Suranyi, 1968). All the children were studied during their first six months while they were being cared for in a special facility for newborns. The children in the first group had the lowest weight gain in the first six months, suggesting that a stress factor operates during the pregnancy of schizophrenic women which later influences the child’s development. Interestingly, the girl babies in this study weighed more than the boys, contrary to the usual finding, additional evidence that boys are more vulnerable to adverse conditions.
Numerous studies attest to the effects on unborn infants of various drugs taken by the mother. The widely publicized effects of the sedative thalidomide are a dramatic example. Many pregnant women who took this drug before it was banned gave birth to infants who had a condition called phocomelia, in which the hands and feet are attached to the body by short stumps rather than by normal arms and legs. Babies born to narcotics addicts are highly likely to be addicted at birth and to have withdrawal symptoms. They also have a high incidence of prematurity, low birtn weight, and mortality (Perlmutter, 1967). Babies born to addict mothers treated with methadone are much less likely to manifest these effects (Blinick, 1968).
A six-year English study found that women users of amphetamines, marijuana, and LSD have a higher-than-average rate of congenitally malformed babies and more stillbirths than nonusers (McCary, 1973). Whether these substances caused such effects in the babies is not clear, however, in that it is possible that other factors in the lives of drug-using women may have contributed to both their drug use and their tendency to have defective infants.
It is estimated that about one-third of women of childbearing age smoke cigarettes. Cigarette smoking has been found to have harmful effects not only on the mother but on the developing fetus as well. Since 1985 one of the messages that tobacco companies are required to print on their advertising and on cigarette packages is “Surgeon General’s Warning: Smoking By Pregnant Women May Result In Fetal Injury, Premature Birth, And Low Birth Weight.” Carbon monoxide gas, inhaled by the pregnant woman, crosses the placenta and forces oxygen out of the blood of the fetus. In a heavy smoker, the fetal oxygen supply may be reduced by as much as 50 percent. Nicotine also crosses the placenta, constricting fetal blood vessels and diminishing the supply of nourishment to the fetus (Shephard and Shephard, 1982).
Although there is no direct contact between the mother’s nervous system or blood circulatory system and the fetus, many substances can pass from her blood vessels in the walls of the uterus into the umbilical blood vessels which serve the fetus. These include chemical substances as well as food and oxygen. Maternal factors affecting the fetus, aside from gross physical trauma, exercise their effect through this transfer mechanism. Special talents, physical stigmata, or personality traits of the child are not caused by specific maternal exposure to similar or seemingly related events, e.g., artistic talent in a child is not caused by his mother’s frequent visits to an art gallery during her pregnancy!
Imitations of Pregnancy
The ambivalence aroused by the phenomena of pregnancy and birth with their multiple meanings are nowhere more apparent than in the psychosomatic disorders and cultural practices whose distinguishing characteristic is an imitation of these great human events. Both females and males can manifest symptoms of pregnancy in the absence of an underlying reality. Pseudocyesis or false pregnancy is a psychosomatic condition in which a woman develops all the symptoms of pregnancy, including amenorrhea, abdominal distention, weight gain, and breast changes. It is found in about 0.1 percent of American women who consult an obstetrician (Katchadourian and Lunde, 1975). The couvade syndrome is likewise psychogenic, affecting a man during his wife’s pregnancy with symptoms resembling those of pregnant women.
Pseudocyesis is an example of the close reciprocal relationship between a woman’s emotional life and her body. The hormone-regulating function of the hypothalamus responds to conscious and unconscious feelings to produce many of the profound body changes of pregnancy. The psychodynamic interpretation of pseudocyesis is one which emphasizes the woman’s conflict over her wish for pregnancy and her fear of it. Immature dependency and hostility toward her own mother may cause anxiety and a dread of pregnancy and its consequences. On the other hand, a pregnant state permits gratification of succorant and dependency needs. Thus the false pregnancy temporarily resolves the conflict.
Couvade symptoms may occur in men at any time after the third month of a wife’s pregnancy (Enoch, et al., 1967). The physical symptoms, including nausea and abdominal distention, are seen as manifestations of anxiety resulting from the threat of his wife’s pregnancy to his own dependency needs, revival of old sibling rivalries, and envy of her new status.
The conscious or deliberate imitation of pregnancy as a superstitious or magic ritual among primitive groups has been observed all over the world (Frazer, 1950). Among the Dyaks of Borneo, if a woman is having a hard labor, a wizard outside the house ties a large stone to his abdomen and then proceeds to imitate the behavior of the woman in labor, moving the stone down his body in the belief that this will facilitate her labor. Several groups accomplish adoption of a child or an adult by an imitation birth ritual. The woman covers herself with a drapery, and the adoptive candidate crawls out from between her legs. The most commonly reported form of couvade, however, is that practiced by the man whose wife is in labor. He takes to his bed or hammock, writhes and moans as if in great pain, and finally “gives birth” in conjunction with his wife. Subsequently, he requires a period of convalescence during which he must be nursed and cared for. Explanations for the couvade include the man’s envy of and wish to identify with the woman’s creative act, as well as his need to establish a bond with the child through giving symbolic birth.
Sexuality and Pregnancy
Taboos against intercourse with a pregnant woman are very common in undeveloped countries and have historically been observed as part of religious rules among some people. Among the Ashanti of Ghana, the pregnancy taboo begins as soon as the pregnancy is determined. The husbands, tiring of abstinence, often take another wife, and it is not uncommon for women to practice abortion in order to avoid the long taboo (Saucier, 1972).
In our society the continuation of sexual activity by pregnant women is not only common practice but is generally sanctioned by physicians though precautions apply here as in other kinds of physical activity at this time. Although there is no evidence that sexual intercourse and orgasm harm the fetus or cause miscarriage or premature birth, women who have a history of miscarriage may be advised to avoid sexual relations for the first few months. Some obstetricians advise women to abstain during the last few weeks of pregnancy. Reliable studies of actual sexual practice during pregnancy are few, and results are equivocal or contradictory, but some trends emerge which may reflect the experience of a significant number of women.
A study of 101 women revealed an increase in sexual tension and performance during the second trimester which they attributed to the increased pelvic vascularity associated with pregnancy (Masters and Johnson, 1966). But other studies are in general agreement that sexual interest and activity fall off during pregnancy, especially during the last trimester (Solberg et al., 1973). Interviews of 260 women in the immediate postpartum period were conducted for information on frequency of coitus, orgasmic function, sexual behaviors other than coitus, coital positions, and relation of sexual activity to prematurity. For most of the women, coital activity declined, though rate was related to sexual-interest level. Women whose sexual interest level had been high before pregnancy had higher orgasmic rates during pregnancy. Of the 44 women who had used masturbation to achieve orgasm during the two years before pregnancy, more than half did not use it during pregnancy. Hand stimulation by the woman’s partner and oral-genital stimulation similarly declined. Side-by-side or rear entry became the preferred positions as pregnancy advanced. Prematurity and condition of the infant at birth were unrelated to sexual behavior of the mother during pregnancy.
Women who reported a change in their sexual behavior during pregnancy gave these reasons: physical discomfort, 46 percent; fear of injury to baby, 27 percent; and loss of interest, 23 percent. Less frequently reported reasons included awkwardness and loss of attractiveness. Of the 260 women, 29 percent were instructed by their physicians to abstain from coitus from two to eight weeks before the estimated time of delivery. Ten percent were advised about positions that might be more comfortable than the male superior position, and 2 percent received suggestions for sexual activities which-could be substituted for coitus (hand stimulation for both partners in all cases). These data reveal a notable paucity of discussion between doctor and patient of sexuality during pregnancy.
While the authors conclude that many women experience a generalized loss of libido with advancing pregnancy, they also note that women’s sexual interest and behavior during pregnancy is quite variable, emphasizing again the highly individualistic nature of female sexuality and its relative freedom from the hormonal, instinctual, and other nonlearned determinants that mediate the behavior of females of other primate species.
The resumption of coitus after the woman has given birth follows no’particular pattern, and its regulation and prescription vary widely from culture to culture. Intercourse with a lactating woman is tabooed among some groups. The Abipon women of Paraguay, for example, nurse their children for as long as three years during which they have no intercourse with their husbands. Where there are no religious or cultural taboos against postpartum intercourse, abstention may be practiced for a few weeks for a variety of reasons relating to the woman’s health and comfort (Saucier, 1972). Four out of six women in one study experienced erotic arousal four to five weeks after delivery, but their physiological responses—vasocongestion of the labia, lubrication, and orgasmic contractions—were reduced in degree and intensity. About half of this large sample of 101 women reported a low level of sexual response, their reasons including fatigue, fear, pain, and vaginal discharge. By three months, however, most of the women had returned to their pre-pregnancy level of activity (Masters and Johnson, 1966).
While there are data regarding sexual behavior during pregnancy and the postpartum period, these are only observations. What are the explanations for this behavior? For a possible answer to this, we look toward cultural and personal meanings of the relationships between a woman’s sexuality and motherhood. The ancient paradigms of woman as Eve, defined by her sexuality, and Mary, the asexual perfect mother, conflict with each other in the pregnant and lactating woman. The ideology of asexual motherhood, the belief that sexuality and motherhood do not coexist in “good” women, is prevalent in our society and has been internalized by many women who are uncomfortable and conflicted with their sexual feelings when they are pregnant or nursing their babies (Weisskopf, 1980).
Psychoanalysts have generally argued that sexuality and maternalism are separate entities, that in the mature woman erotic feelings give way to motherly concern. But theorists from Freud on have also recognized that babies and young children have erotic sensations and respond erotically to their mothers’ ministrations of nursing, caressing, diaper changing, and so on. According to psychoanalytic theorists, the erotic nature of mother-infant contact is not supposed to be reciprocal. Therein lies the taboo on maternal sexuality (Weisskopf, 1980).
As we have seen, the sexual activity of women declines as pregnancy advances. While this may be partly due to discomfort and fear of harming the fetus, it has been suggested that the decline, which is highly variable cross-culturally, is owing in part to some women’s internalization of the taboo against combining sex and motherhood. They feel embarrassed, awkward, guilty. Their fear of harming the baby, especially, is a symbolic rationalization. Their thinking goes as follows: sexual activity could harm the child; a good mother protects her child; therefore, a good mother does not have sex during pregnancy (Weisskopf, 1980).
Breast-feeding, too, evokes conflicts for some women because of its erotic qualities. Twenty-five percent of one group of women who decided not to breast-feed did so because of the erotic sensations aroused by the experience. Another 25 percent who were stimulated sexually by nursing reported marked guilt feelings (Masters and Johnson, 1966). As the sexuality of women becomes more liberated from the prohibitions of the past, we can expect less conflict involving the sexual aspects of pregnancy. Perhaps in the long run the woman’s feelings of safety and well-being are the most important variables.
Psychological Aspects of Pregnancy
A number of influences converge to determine and to mobilize the psychological adjustment of the woman during pregnancy. First, the physical changes in body physiology and in body size and shape, which can evoke feelings in part dependent upon her perception of these changes. Second, her pre-existing psychological status, her capacity to handle whatever stresses accompany her pregnancy; third, her real-life situation, marital status and relationship, and the number and ages of her children; and finally, the psychodynamic meaning the pregnancy has for her, with its potential to evoke conflicts around dependency needs, rivalries with mother or siblings, hostility toward the husband, and unconscious attitudes toward the self and female functions. All these variables contribute to the woman’s reactions to the pregnancy experience, their relative importance depending upon the individual.
Unfortunately, the research on the psychology of pregnancy is sparse. And while most of it deals with unusual or pathological maternal behaviors, pregnancy and childbirth are normal physiological events, and most are uncomplicated by serious physical or psychological pathology. The experience is not bland, however, and women have a wide range of feelings and reactions which are individual and yet part of a commonly shared experience.
Self-image
Changes in body size and shape are dramatic in the second and third trimesters, requiring radical alterations of the body image, of the way the woman perceives her physical self. One study found that the pregnant women, compared to the nonpregnant control group, felt less feminine and had increased levels of concern over the body and its functions. (Treadway et al., 1975). Although there are no data bearing on this, we should note parenthetically that the feelings a woman has about her figure changes can be expected to reflect her attitude toward her pregnancy. An emotionally secure woman who wanted to be pregnant may well be proud of the visible evidence that she is expecting a child. On the other hand, a woman whose feelings of worth derive largely from living up to a conventional standard of sexual attractiveness may be anxious about what the pregnancy is doing to her figure. These observations demonstrate the important point that there is no direct causal relationship between the physical changes of pregnancy and the psychology of the pregnant woman. Rather, her psychological status is the result of interaction among the variables we are discussing.
Stress and anxiety
Pregnancy, particularly the first one, is a developmental crisis in a woman’s life, in that it ushers in a new stage of life with new tasks and problems which require adaptations and solutions that have yet to be learned. As a crisis, it escalates the total amount of stress experienced by the woman, making additional demands upon her psychological adjustment and coping ability. Consequently, her characteristic psychological status, as it is affected by the additional stress of pregnancy, is one determinant of her adaptation during pregnancy. Women with a history of menstrual symptoms, marital conflict, and anxiety had more physical symptoms during pregnancy, and anxiety during pregnancy was related to the amount of pain relief required during labor (Zuckerman, 1963). In another study a group of pregnant women with hyperemesis (pathological vomiting) were compared with nonvomiting pregnant women. Hyperemesis was more likely to occur in women who had repeated severe life stresses and previous illnesses. They also had a higher rate of prematurity and labor complications (Tylden, 1968).
Women who tend to be anxious and who have a timid or fearful approach to life and to new situations in particular can be expected to show elevations of these reactions to the experience of pregnancy with its perceived and real potential for demanding adaptations and life changes. For example, women who were afraid of pregnancy were more likely to manifest depression when pregnant (Kutner, 1971). But a large-scale survey of attempted suicides found that the incidence of such attempts was not greater for the pregnant group. In only one-sixth of the pregnant women did their pregnancy seem to be the dominant cause of the attempt. For most, the pregnancy was incidental to the attempt, which was related to the same kinds of emotional instabilities and interpersonal problems that characterized the attempts of the nonpregnant women (Whittack and Edwards, 1968).
Depression
Physical changes during pregnancy which are most closely related to psychological state are changes in gonadal hormone levels and changes in body size and shape. Elevations in estrogen and progesterone in pregnant animals have been shown to be related to decreased levels of norepinephrine (NE), a chemical substance manufactured in the brain. A review of the evidence for an association between decreased NE and depression indicated that many clinical depressions may be related to NE deficiency (Schildkraut, 1965). To test this hypothesis, a biochemical and psychological assessment of twenty-one pregnant women and a control group of nine women, all with no history of psychiatric illness was conducted. Urinary excretion of NE was significantly lower in the pregnant group, and the deficiency was found to be correlated with increased scores for depression in the psychological evaluation. It is hypothesized that the reduction in NE linked to the gonadal hormone changes of pregnancy might be responsible for the increased depression (Treadway et al., 1975). This interpretation is based, however, on the important assumption that depression as measured by test scores of pregnant women is similar to clinically observed depression, and not all of those with reduced NE had test scores reflecting depression. The findings lead to a tentative conclusion that pregnant women have an increased biologic susceptibility to affective (mood) disorders, suggesting that other factors are important determinants of whether or not a given woman actually manifests a depression during pregnancy.
Reality factors in the woman’s life affect her psychological adaptation to pregnancy. Several themes emerged from a group of young married women who were both working to support their husbands and pregnant for the first time. There were concerns over bodily changes and fears about delivery, concerns about the normality of the infant, increase in wanting to be cared for and irritation toward the husband for not meeting this need, and fantasies about the babies and their own ability to function as mothers. Most had not planned on becoming pregnant, and the advent of a child in their lives was clearly disruptive to their present life styles. The same study included a sample of unmarried women who were pregnant for the first time. Their responses brought out the influence of sociocultural factors and attitudes toward unplanned and unwanted pregnancies. These women expressed feelings of depression and dependency, and saw their pregnancy as a disgrace to themselves and their families. Major themes were their desire for a dependent relationship with a man and ambivalence about giving the child up for adoption. Although such pregnancies are easier to terminate now than they were at one time, there is no reason to doubt that the initial feelings they evoke are any less prominent (Loesch and Greenberg, 1962).
In general, first pregnancies present more problems of a psychological nature than later ones do. Women who were pregnant for the first time were compared with women who had given birth before. The former expressed more anxiety about themselves and the baby, while the latter had fewer of these concerns but expressed more generalized feelings of irritability and tension (Erickson, 1965).
Relationship with one’s mother
Finally, the psychological reactions of a woman to her pregnancy are to some extent dependent upon intrapsychic variables which may be largely unconscious. In addition to the physical and emotional stresses, pregnancy has the potential of evoking old conflicts around dependency needs, particularly with regard to one’s mother.
The woman’s relationship with her own mother has moved from the total dependency of infancy to the relative independence of adulthood, sometimes accompanied by chaotic struggles to free herself as well as by regressions to the old safe role of childhood. Pregnancy holds the promise of putting her finally on an equal level with her mother and of achieving a mature relationship with her. Two kinds of relations to their mothers have been observed among pregnant women. One type displayed an increased dependence on their mothers’ support and advice, and were overinvolved in their mothers’ attention and competitive for it with the other members of the family. As the pregnancy progressed, many of these women began to disengage, to begin to make their own decisions with an accompanying rise in self-esteem. Another type were belligerently independent at first, as if old grievances were evoked bringing out a determination that mother would not interfere with the baby as she had with her daughter. This reaction also ameliorated in time in these normal women, who became more tolerant and accepting of their mothers and expressed increased understanding of them from their own new perspective of impending motherhood. When such submissive or rebellious mother-entanglements are of pathological extent, however, they resist such smooth resolution, carrying over old conflicts into the new mother-child dyad (Bibring, 1975).
Positive Effects of Pregnancy
Pathological reactions to pregnancy have attracted the most research attention, resulting in a less than adequate concept of normal psychological changes during this period. The focus on pathology gives a biased picture of the meaning of pregnancy for many, if not most, women. Some epidemiological studies, for example, indicate that the mental health of women improves during pregnancy. Severe psychopathology decreases with pregnancy, psychotic reactions are rare, and admissions to psychiatric hospitals decline (Leifer, 1980).
It may be that symptoms of emotional disequilibrium in pregnancy are actually adaptive signs of growth, in preparation for motherhood. Anxiety directed toward the unborn child, for example, was found to be a reflection of the developing maternal bond, not of pathology of neuroticism (Leifer, 1980).
We have been discussing the sources of influences that affect the psychological reactions of a woman to her pregnancy. It should be clear that such reactions, both positive and negative, develop from the interactions among these influences and their relative strength as determinants for the individual woman in her unique situation. While it is not uncommon in clinical or educational settings to hear young women express ambivalence or even strong negative feelings about pregnancy, one often finds that these feelings either diminish or are repressed when the woman actually becomes pregnant, particularly if her life situation is compatible with such an event. Childbearing continues to be for most young women a major developmental challenge, with achievement connotations that are often ignored or unrecognized. The motive for doing it well can be quite strong, with positive, maturing consequences for the woman. If she is physically and psychologically healthy, if the pregnancy is a wanted one, if she has a history of relatively satisfying relationships with the important persons in her life, then she is likely to experience this developmental event as rewarding and growth enhancing.
The Postpartum Period: Mother-Infant Bonding
In recent years a few researchers have become intrigued by the phenomenon of mother-infant bonding—the forming of unique affectional ties between the new mother and her child as a result of physical contact for a period of time immediately following delivery. It is typical in American hospitals for the newborn to be separated from her mother soon after being born and to be returned to her at three- or four-hour intervals only for feeding. Such separation of mother and child is probably not “natural.” It is more a result of modern hospital “efficiency” than of human evolution. In less technological societies, the infant is not separated from the mother. What, then, is the effect of separation on the mother-child relationship, or conversely, what is the effect of prolonged postpartum contact on that relationship?
The results of a series of studies indicate that the immediate postpartum period is highly significant for the development of maternal attachment (bonding) and that its occurrence or nonoccurrence can affect the mother’s behavior toward her child for as long as two years after its birth. In a Guatemala hospital, nine mothers were given their naked babies right after delivery, while nine others were separated from their infants in accordance with usual hospital routine. Twelve hours later all the babies were returned to their mothers for their first feeding. The mothers who had had early contact with their babies were more likely to fondle and kiss them, to gaze at their faces, and to hold them close than were the mothers whose babies had been removed (Klaus and Kennell, 1976). In a similar study of American mothers, fourteen had the traditional brief contact plus feeding visits, while another fourteen had contact with their babies for one hour postpartum plus an additional five hours in each of the next three days. One month later each of the twentyeight mothers was observed with her baby. The mothers who had had the extra hours of contact were more likely to pick up their babies when they cried, stood closer to the baby when it was being examined, and were more likely to soothe it if it became upset. At a similar observation a year later, the extended-contact mothers spent more time helping the doctor and soothing the child if it cried. At two years, the extended-contact mothers, in talking to their children, used twice as many questions, more adjectives, and fewer commands. It appeared, then, that the extra contact at birth still had an effect two years later (Klaus et al., 1972; Klaus and Kennell, 1976).
These data support the possibility of a sensitive period in human mothers, during which close contact with their infants facilitates feelings of attachment that carry over into maternal behavior. They also raise questions. What is the mechanism whereby such bonding takes place? Is it hormonal or neurological or both? What about fathers? Can they become “bonded” to their infants, and if so, how? The occurrence in fathers of anything similar to maternal attachment would not make sense from an evolutionary perspective since fathers were not necessarily identifiable and were not usually present at births. Apropos of this is an interesting observation by Klaus and Kennell (1976). Two Israeli mothers were given each others’ babies by mistake. When the mix-up was discovered two weeks later, each mother had become so attached to the baby she had that neither wanted to give it up. It was the fathers who wanted the error corrected, citing family reasons.
The Postpartum Period: Reactions and Adaptations
The hours, days, and weeks following childbirth are noteworthy for the personal and emotional adjustments the woman must make, as well as for the physical changes which occur in her body. She is confronted with the reality of the baby, the irrevocable fact that it is here to stay, and that its imperious demands must be met at whatever cost to her own needs and time. Especially with a first baby, her life style changes drastically because of the total dependency of the infant whose needs now come before her own, a state of affairs which can provoke anxiety approaching panic in new mothers. It becomes clear to her that her life will never again be the same, that she is now responsible for the care and well-being of a helpless infant whose very life is in her hands. Under the best of circumstances, with a sharing mate and helping friends and relatives, the postpartum period makes adaptive demands many women find difficult to meet.
Reactions of women in the postpartum period cover a wide spectrum, from transient and mild to lasting and severe. The experience of any given woman is the result of a number of factors with origins in her self, her immediate experience, and the cultural milieu. “Baby blues,” with mild depression, tearfulness or crying spells, and irritability are common and usually pass in a few weeks. Feelings commonly reported by postpartum women include inability to concentrate, fantasies of running away, anger toward the baby and her husband, helplessness, inability to cope, and lethargy and fatigue. Serious psychiatric conditions requiring hospitalization and treatment are rare, affecting one or two women per thousand in the postpartum period (Brown and Shereshefsky, 1972).
The high pregnancy levels of estrogen and progesterone drop rapidly after delivery, effecting endocrine changes which can influence mood states. While these have been implicated in postpartum reactions, other factors must be considered in trying to understand individual reactions and the more serious manifestations (Dalton, 1971). A Swedish study of adjustment during and after pregnancy of 165 women found that more than a third had some symptoms of postpartum mental disturbance. Number and severity of symptoms were related to the woman’s attitude toward her reproductive function, her relationship with the child’s father, and conditions at the time of the birth (Nilsson and Alnigren, 1970).
Further evidence suggests that postpartum adjustment has important determinants other than the physiological. The following “signals” in the background of women with adverse reactions were found: family home broken by death or other separation; previous emotional disorder in self, parents or other immediate family; physical illness or complication of pregnancy; marital differences in religion or age, marked shift on economic social ladder; recent move; older parents; unplanned pregnancy; and acute strains during pregnancy, such as husband away or no outside help in the household (Gordon and Gordon, 1967).
Summarizing, the research findings suggest that a model for explaining and predicting postpartum adjustment must include four major components; the woman’s personal vulnerability to stress, immediate environmental conditions, relations with significant others, and biochemical changes.
Lactation and Breast-feeding
Lactation is the formation and secretion of milk. The first secretions of the breasts are not milk but colostrum, a protein-rich liquid which is present soon after parturition and meets the baby’s nutrient needs, if breastfed, for the first two to four days of life. Colostrum is also thought to give the baby protection from certain infectious diseases for the first few months of life. The production of milk is induced by prolactin, a pituitary hormone, and within a few days the ducts in the breasts become engorged with milk. Oxytocin, the same hormone involved in uterine contractions, brings about the “letdown” response of the milk when the nipple is stimulated by the baby’s sucking.
The practice of breast-feeding the infant varies by era and by place. Some primitive groups breast-feed babies for several years, or until a new arrival forces the older child from the breast. In undeveloped societies breast-feeding may be necessary for the child’s survival, although artificial feeding has been practiced all during historical times, as attested by finds of clay nursing bottles and other related artifacts. Wealthy Roman women avoided breast-feeding in order to keep the youthful appearance of their breasts, and even today women express anxiety that nursing will cause their breasts to sag. In the United States, the incidence of breast-feeding has fluctuated with availability of alternative methods as well as with fashions and value systems. At the turn of the century, 90 percent of babies were breastfed for at least a few months. By 1946, when prepared baby foods and canned milk were available in all grocery stores, the figure had dropped to 33 percent, and ten years later, in 1956, only 12 percent of babies leaving the hospital were breast-fed (McGary, 1973). By 1966, the trend turned upward, and 20 percent of mothers were breast-feeding their infants. A decade later, the figure had increased to 40 percent, a phenomenon attributable mostly to middle-class, well-educated women (Brody, 1977).
The current revival of breast-feeding has a variety of sources, among them the counter-culture movement with its emphasis on simplicity and natural substances, the participatory childbirth movement, loosening of taboos about body parts and functions, and of course, the belief that mother’s milk is better for the child. Still, a sizable percentage of women choose not to breast-feed their infants, and others who want to become discouraged and terminate their attempts after a few days or weeks. Several factors exert pressure against the decision to breast-feed. Most hospitals still separate mother and infant right after birth and bring the baby to her every three or four hours for feeding. The first few days or weeks of the nursing experience may be discouragingly uncomfortable. Swollen, tender breasts and cracked nipples are not uncommon. Hospital medical staff often do not take the time to provide instruction and to reassure the anxious mother who fears the baby is not getting enough milk, or to advise the one whose nipples become sore. Too, some mothers do not wish to be tied down to the baby’s feeding needs. Sometimes husbands complain, or relatives decry breast-feeding as too confining or old-fashioned. Considering all these pressures, the wide availability of substitutes for mother’s milk, and the less-than-mandatory nature of breast-feeding, perhaps it is surprising that it continues to be popular with many women.
Some researchers have wondered if there are personality differences between breast-feeding and bottle-feeding mothers. One study compared these two groups and found no differences between them in personality. They did differ in other ways however. The breastfeeding mothers were rhuch more likely to cite their concern for the baby’s health and their own personal gratification as reasons for choosing to nurse. Bottle-feeding mothers cited convenience and their own “personality.” A notable finding was that 70 percent of the breast-feeding mothers had attended preparation for childbirth classes, compared to only 30 percent of the bottle-feeding group. It appeared that infant feeding decisions were related to learning, practical considerations, and attitudinal differences rather than to personality (Golub, 1978).
Success with breast-feeding has been closely related to the mother’s attitudes. Those who felt positive about it as new mothers were those who-were successfully nursing by the time they left the hospital. Other attitudes differentiated them also. They felt that women have more satisfying lives than men do, and that their labors had been easy. They showed strong interest in their infants, and were more likely to engage in close body contact with them, such as sleeping in the same bed. Furthermore, they were more open in their views of sex and nudity and were more tolerant of sex play and masturbation in their children (Newton, 1968).
Human milk has always been endorsed by the medical profession as preferable to commercial formulas prepared from cow’s milk. The endorsement, however, has been half-hearted, conveying the message that, though breast-feeding is better, the difference is not significant enough to be important. The formula industry capitalized on this attitude and persuaded both physicians and the lay public that their product was not only as healthful as breast milk, but that it was convenient, hygienic, and, most of all, liberating, freeing women from the messiness of dripping breasts and the need to be available to the infant at all times. In the absence of a strong counter-argument, most women chose, and still choose, not to breast-feed their infants.
In the past few years, new scientific Endings have greatly increased knowledge about nutrition and human milk, casting serious doubt on the earlier complacency regarding the relative merits of human versus cow’s milk for infant feeding. Human milk has a wide range of protective effects against infectious diseases, which is especially important where hygiene is poor, as in developing countries. It is also the best protection against food allergies, for about 1 percent of bottle-fed babies develop an allergy to cow’s milk. In nonindustrialized societies, breast feeding has a large statistical effect on the birth rate, since children are naturally spaced further apart owing to the effects of long periods of nursing on fertility. Formula feeding is also prohibitively expensive for poor people. In developing countries, for example, it would take as much as half a family’s income to feed one infant adequately with formula (Jelliffe and Jelliffe, 1977).
The scientific community now has a significant knowledge base to support a strong case for breast-feeding. As one physician wrote, .. one must be careful and humble before attempting to modify nature” (Barness, 1977). Even so, the practice of breast-feeding often comes into conflict with the social realities of modern societies. Many mothers of infants are employed outside the home, in places with no provisions for the care of babies. Some women do not want to nurse for personal and practical reasons, and a few cannot for physical reasons. Also it is obvious that babies do thrive on formulas. A balanced appraisal would support the approach which includes information giving, counseling, availability of options, and sensitivity to the woman’s needs and preferences as well as the baby’s.
In this chapter we have looked at some reasons why people choose to have children and have reviewed the events, both biological and psychological, which are part of the reproductive sequence. By now it should be plain that in this area of woman’s experience, the biology and the psychology of women are so intertwined that it is not productive to try to think of them as discrete sets of events, one belonging to the body, and the other to the mind. Pregnancy affects the way a woman thinks and feels, and the way she thinks and feels affects her pregnancy and labor. But neither of these is a sole determinant of the other. A third important source of influence emanates from the society she lives in and its attitudes toward her and toward her reproductive and social roles. We have seen how attitudes toward woman’s reproductive role have changed drastically in recent years. These changes are bringing about modifications in her social roles as well as value shifts which are requiring different adaptations of both women and men. These modifications and adaptations as they are reflected in contemporary life styles are the subject of the next chapter.
10. Women’s lives: tradition and change
Il is my thesis that the core of the problem for women today is ... a problem of identity—a stunting or evasion of growth that is perpetuated by the feminine mystique.... [O]ur culture does not permit women to accept or gratify their basic need to grow and fulfill their potentialities as human beings, a need which is not solely defined by their sexual role....
—Betty Friedan, The Feminine Mystique, 1963
The very importance of children, family, the home that is a constant of our consciousness today is based not only on the real needs of men and children for nurturing and loving care and the “complementary, ” “female” abilities of women— but also on the needs of women, equally real and basic to the human condition, for mastery, power, assertiveness, security and control. And evolving self-realization for us all....
—Betty Friedan, The Second Stage, 1981
Until fairly recently, most American girls could count on following the traditional path for women, exemplified by their own mothers’ commitment to domesticity and to the primary roles of wife and mother. Most girls looked forward to marriage and motherhood, with their attendant meanings of adult status and security. Further, any other way of living one’s life was considered second best. Not only were choices few and unattractive, but the assumption was that the woman who opted for an alternative to the domestic life did so, not by choice, but by the necessity forced upon her by the lack of a husband. While most young women still look forward to one day marrying and having children, they recognize that other possibilities exist and that they have options their mothers never had. The combination of married life along with either a job or a career is the norm today. Deferred marriage, staying single, divorce, childlessness—all are in the experience of many American women, and all represent alternatives that are at least as viable as, and to many more attractive than, the life prescribed for their counterparts less than a generation ago.
While the roles of wife and mother are still primary for most women, particularly at certain stages of their lives, the lives of others may depart drastically from this model; and in between, are degrees of conformity and innovation that suggest a spectrum of ways to live for women in today’s world.
Although society is more open to women today, the freedom to choose and to shape one’s life is still an illusion for many. Excursions of women into the work world outside the home, for example, are— often from economic necessity—adding to their repertoire another role. The work is usually of secondary importance and often a paid and formalized version of one of the primary roles: nurse, teacher, or waitress. The woman who combines a job outside the home with her domestic roles is no longer a curiosity, though the wife and mother with a strong commitment to a demanding career is still in a small minority of unusual women.
But radical social changes are sweeping the old institutions and challenging old beliefs and prejudices, and demographic and technological developments facilitate the spread of their influence and soften resistance to them. Egalitarian ideology becomes practical as women acquire the means of economic independence and freedom from childbearing. These realities promote redefinition of goals and values and effect fundamental changes in social structure and in the relationships between women and men.
In this chapter we shall examine some aspects of the life styles of contemporary American women in the traditional roles and their variations, and in young, emergent models which may become the norms of tomorrow.
The Traditional Role
A woman enters the traditional female role-dyad of wife and mother through the event of marriage, which occurs in this country at the average age of 23.3 for women and 25.5 for men. The rituals preparatory to and culminating in the wedding are in a sense a rite de passage between girlhood and adulthood. Her friends and her mother weep as she is given away by her father to a man whose name becomes hers. She is expected to give up the ways of her childhood and to take up the tasks that are appropriate to an adult woman. The event marks for her transition into a new status and a new role, that of wife.
Women in American society move into, function in, and abandon roles in a rough chronological order that corresponds to the developmental life cycle. The cycle has changed drastically over the last century as the life span has become longer and the years devoted to childbearing fewer, but its major events are the same. Women today, however, are marrying later, postponing childbearing, having fewer children, and, in some cases, choosing to remain childless. During the late 1950s, 70 percent of white women had their first child in the first two years of marriage; fifteen years later, fewer than 60 percent did so (Van Dusen & Sheldon, 1976). During the 1970s the birth rate reached a record low of fourteen live births per one thousand population at mid-decade, but in 1979 the bureau of the Census reported a slight increase. Although most women expect to have children, the number of all married women who intend to remain childless has increased by 25 percent in the past twenty years. Today’s young woman can expect to live forty-six years after her last child starts to school, compared to only thirty in 1890. At that time, too, she was widowed before the marriage of her last child, whereas today she still has sixteen years of married life after that event, greatly increasing the amount of time that she and her husband will be alone with each other.
Co-ordinated with this chronology are the following transitions and stages in the lives of women which define their more important roles at any particular time: from the socializing home and family environment of early childhood to school and work situations; from the multidimensional life of the young adult to a new identity as married woman and housewife; from the life of young wife to that of new mother; from almost total immersion in the care of small children to a stage of increasing competence as housewife, confrontation of children’s problems as mother, habituation as wife, and varying degrees of participation in community activities; from full participation in family life, seen as ideal for women, to constriction or loss of roles as children leave home and husband dies; and from being the sole member of a household to one of a variety of life styles until death (Lopata, 1971).
With the exception of that brief interlude before marriage, the stages and transitions characterizing the lives of most women are all described in terms of the roles of wife and mother. Even though the eighties found more than half of all adult women in the work force, most of these, as we shall discuss later, are clustered at the lower end of the wage distribution, and they themselves consider their work roles to be secondary to their roles at home.
When we think of the traditional family life style, we visualize a bread-winner father, a stay-at-home mother, and one or more children. But only a small minority of adult Americans really live in such a household. As the data in Table 10.1 show, more adults head single-parent families, live alone, live in child-free marriages, or in dual-breadwinner families than live in single-breadwinner nuclear families. Regardless of the constituency of the household, however, 95 percent of all women aged thirty-five and older have been married at least once, and 90 percent of them have had at least one child (Van Dusen and Sheldon, 1976). Thus the great majority of American women do experience, for part of their lives, the responsibility of being a wife and mother.
Table 10.1 Distribution of adult Americans by types of household
| Heading single-parent families | 16% |
| Other single, separated, divorced, or widowed | 21% |
| Living in child-free or post-child-rearing marriages | 23% |
| Living in extended families | 6% |
| Living in experimental families or cohabiting | 4% |
| Living in dual-breadwinner nuclear families | 16% |
| Living in no wage-earner nuclear families | 1% |
| Living in single-breadwinner nuclear families | 13% |
Source: News release, Bureau of Labor Statistics, 8 March 1977.
The role of housewife
Marriage introduces women to sets of activities and duties which cluster into their customary roles in the home. The expectation that women would move into these roles in the normal course of their lives and would perform the associated tasks gladly and well is traditional in our society and persists to the present time. Coexisting with it for over a century, however, is another view whose proponents see the identification of women with the domestic role as an assignment to a “place” which inevitably precludes equality between the sexes. The extremes of feelings of these views are defined by the two following positions:
First, woman’s place is in the home, fashioning it into a clean, comfortable, attractive place where good food is served, order is maintained, and the personal needs of the occupants are met. She does whatever is necessary to manage this, and she does it not for money or personal gain, but because it is her duty to her loved ones. Furthermore, it is an exalted role, the highest that a woman can have. Any woman who does not believe this, who wishes or tries to do something else, is unnatural, immoral, and unwomanly.
Second, the work that is necessary to maintain people comfortably is not special or different from any other tedious and repetitive labor. It can be done equally well by both sexes. The beneficiaries of such work should share in doing it or pay a fair wage to have it done by someone who chooses to do it. The exemption of men from this work and the assignment of it to most women is a major source of oppression and the chief reason preventing women from developing their potential and making their full contribution to society.
While neither of these positions represents a majority view, they reflect climates of opinion which have existed in our society both in the past and in the present, although it is fair to say that the first statement would have found more supporters in the 1800s than today.
Domesticity and skill in the domestic arts were highly prized in young women during the eighteenth and nineteenth centuries; it was lack of ability in this area or expressed interest in some other role that was deplorable. For example, the English journalist William Cobbett wrote in 1829 of how he fell in love with his future wife:
It was now dead of winter, and, of course, the snow several feet on the ground and the weather piercing cold.... In about three mornings after I had first seen her our road lay by the house of her father. It was hardly light, but she was out on the snow, scrubbing out a washing tub. “That’s the girl for me,” said I ... (in Klein, 1971, p. 176).
The celebration of the value of housekeeping skills for women was affected by the Industrial Revolution and the resultant technology with its production of labor-saving equipment for the home and its usurpation of many of women’s traditional jobs. Factories not only took over the spinning and weaving of cloth, the manufacture of clothes, the processing of food and other products formerly made by women at home, but they also gave women the chance to become economically productive. As housework became easier, and work away from home became available, the role of the stay-at-home woman declined in status. The doors continued to be closed, however, to the kinds of education and work that might interest upperclass women, who became consigned increasingly to lives of barren routine and trivial interests.
Toward the end of the last century, a movement began to appear whose goal was to elevate the status of the housewife role to something approaching equality with the male professions. Women were told, in effect, that housework was real, important work requiring complex skills which were just as vital as those necessary to the practice of law or medicine. The acquisition and practice of these skills in home management was a unique mission of woman, and if approached in these terms, would constitute for her a “career” as deeply satisfying as any that man could aspire to. Books were published on domestic science and domestic engineering, and courses in
Home Economics appeared in the curricula of schools and colleges.[41] One book was The American Woman’s Home: Or Principles of Domestic Science, by the nineteenth-century authors Catherine Beecher and her sister, Harriet Beecher Stowe. While contemporary feminists argued for the legal and economic equality of women, Beecher and Stowe took a different tack. Realizing as well as the feminists did that something was wrong with the lot of the American woman, they sought to improve it by legitimizing her domestic function and by bringing to it some of the dignity that invested male activities:
It is the aim of this volume to elevate both the honor and the remuneration of all the employments that sustain the many difficult and sacred duties of the family state, and thus to render each department of woman’s true profession as much desired and respected as are the most honored professions of men (p. 13).
The promotion of the housewife-mother role as the only truly important and rewarding one for women continued unabated through the 1970s. A study of women’s roles in women’s magazine fiction from 1940 to 1970 revealed that the only proper role portrayed for women was the role of housewife and mother. The nature of the role involved total dependence on the husband and complete dedication to her family. The role is validated by contrasting it to the “deviant” roles of spinster, divorcee, career woman, or any childless woman. The housewife-mother in these stories might briefly envy such a woman, but when she attempts to emulate her by going to work, taking a trip alone, or even eventually attaining some of her freedom when her children get older, she is brought to a realization of the much greater worth of her position by her family’s constant need for her or by her own guilt which she assuages by staying home and/or having another baby (Franzwa, 1975).
A far different evaluation of women’s place and the life that went with it had supporters at the same time that the domestic reform movement was attempting to elevate its status and convince women of its high mission. Marxist and socialist ideology included attacks on the family itself as a major oppressor of women. Marxist and feminist writers (see in The Feminist Papers [Rossi, 1973]) were vocal critics of women’s assigned roles. Friedrich Engels, a nineteenth-century Marxist and bitter critic of the modern family, wrote that it is “founded on th? open or concealed domestic slavery of the wife ...” (p. 486), and the economist John Stuart Mill, reflecting in 1869 on why women had achieved so little, said that the supervising of a household “is extremely onerous to the thoughts; it requires incessant vigilance, an eye which no detail escapes, and presents questions for consideration and solution, foreseen and unforeseen, at every hour of the day, from which the person responsible for them can hardly ever shake herself free” (p. 228). Feminists of the time, while stopping short of attacking marriage itself, were under no illusions about what it meant for women. Sarah Grimke in 1837 commented that women are brought up with the belief that keeping a husband’s house and making him comfortable was the end of their being, and called such indoctrination “dangerous and absurd” (p. 312). Two decades later, soon after the birth of her sixth child, Elizabeth Cady Stanton wrote to Susan B. Anthony, “I pace up and down these two chambers of mine like a caged lioness longing to bring to a close nursing and housekeeping cares ...” (p. 380).
Today, feminists see the confinement of women to traditional roles as major deterrents to the realization of the goals of equality and freedom of choice. They reject the glorification of these roles and the notion that they are the special province of women, who should be responsible for the tasks they include. “[We] women have been brainwashed more than even we can imagine. Probably too many years of seeing television women in ecstasy over their shiny waxed floors or breaking down over dirty shirt collars. Men have no such conditioning. They recognize the essential fact of housework right from the very beginning, which is that it stinks” (Mainardi, 1972, p. 283).
It is difficult to think of any other occupational role which excites such extremes of feeling and comment. Many other jobs in the society rank low in pay and status, and sometimes bitter disputes arise over the conditions associated with the work, but no one gets emotional about the job itself. The matter of who is going to do it and how rarely becomes a political issue. But the role of housewife is not like any other occupational role; its physical and psychological environment, its working conditions, constraints, requirements, and rewards are totally different from those that characterize the occupations both women and men perform outside the home.
In the first place, the society does not provide formalized training or instruction to prepare persons to do the tasks that the role normally requires. Women may become housewives overnight, simply by getting married. There are no particular requirements for the job, and whether one comes to it with many skills or none is irrelevant. It is assumed that one either knows how to run a household or that one will learn “naturally.” In one study when the women were asked what training they had received before marriage that was helpful to them in their housewife role, a fifth answered “none.” The most frequently mentioned sources of help were their mothers and a school course. A majority of the respondents felt that women were not adequately trained to be housewives, and women with more education were even more likely to see the role as requiring more skill than they had when they entered it (Lopata, 1971).
Second, the specific tasks performed by women in the home are carried out under conditions which require diffusion of attention and effort. Many events may be competing simultaneously for some action on her part. The phone rings, a pot boils over, the baby wakes up, the dog wants to go out, the three-year-old falls down, the second-grader bursts in from school—experiencing all these events alt the same time, each demanding her attention, is in the norma,! course for a housewife. Furthermore, the role requirements are highly repetitive and allow for very little respite or privacy. She is “on call” for whatever needs to be done, twenty-four hours a day.
A third characteristic which differentiates this role from other occupations is that there are no standards or tests of performance, no objective, externally imposed measure of how well the role is performed. And unlike any other job that one can think of, the rewards have no direct relationship to the quality of the performance. A woman who keeps a dirty house and feeds her family hamburgers and soft drinks three times a week does not necessarily lose her job as housewife; on the other hand, her neighbor who maintains a spotless home, cooks gourmet meals, and makes all the children’s clothes herself does not necessarily get more material or affectional rewards for her efforts. The job can be done sloppily or perfectionistically without directly affecting the woman’s tenure in it. Because of its private, personal quality, it is basically invisible to the larger community.
A fourth feature of the housewife role is its ambiguity. No job description for it exists; whereas other occupational roles include specific rights and responsibilities, the housewife role does not. No wage and hour laws apply to it, nor are its duties prescribed. A woman with grown children and a full-time maid has as much right to the title as has a woman with five children under ten and no outside help. Furthermore, from a list of all possible household tasks a woman may actually perform none, several, or all of them. She may have much help or none, many tools or few. She may do her work at any time of the day or night. She structures the job to her own situation. No union protects her or interferes with her highly individual style of performance. Also, a woman calls herself or is called by others a housewife only if she is not otherwise employed. If she works in a bank or a hospital, her response to the question, “What do you do?” is “I am a banker,” or “I am a nurse,” not “I am a housewife.” This is true even if she performs exactly the same jobs at home that her unemployed sister does. It seems to be tacitly understood that one is designated “housewife” only if one is not something else. All other work-related roles have priority as descriptors of the person.
Perhaps related to this phenomenon is the often-noted low status and devaluation of the role of housewife. The apologetic “just a housewife” suggests that nothing such a person does in that role is of any importance, that it cannot compare in status with a “real job.” The housewife’s status depends not on what she does but rather on who she is. Elsie Smith has a certain status in the community because she is the wife of Harold Smith, high-school principal. Her status is set by the status of her husband, who has that status because of what he does. One recalls Terman’s comment that a good many of the gifted girls in his sample made their most notable achievement in their choice of a husband (see Chapter 6).
Finally, let us note that the role of housewife differs from other occupational roles in that the personal qualities of the woman are not related to her admission to the role category. While the role of, for example, engineer, requires a certain level of intelligence, aptitude, and interest, the role of housewife is unspecialized in this regard. Housewives are not different from women in general. No particular personality, temperament, intellectual level, or set of interests is specified as critical to performance of the role. One does not have to be “suited” to it, either by training or by temperament.
Ina study of almost six hundred Chicago-area women, the social roles of wife, housewife, and mother were analyzed (Lopata, 1971). This work offers an empirically based description of these traditional roles of women in contemporary society derived from extensive field investigation of both suburban and urban women, employed and non-employed. Although women are increasing their involvement in economic, political, and educational roles, the women in this study were emphatic in giving the home roles of women the status of greatest importance. In fact, when asked “What are the most important roles of a woman, in order of importance?” most referred only to the roles of mother, wife, and housewife. Only onefifth even mentioned roles connected with work, or with social, community, or religious organizations. Asked to rank in importance thirteen possible roles of women, the subjects gave the lowest four places to artist (self-expression), career woman, worker, and member of the community. Factors which were important in this rejection of non-familial roles were the respondents’ stage in the life cycle, and their educational and economic level. Mothers with young children stressed family roles, as did the poor and less educated. Women who worked were more tolerant of expanded roles for women in general, and women in the higher social classes were more likely to view extrafamilial involvement as important. But basically, the respondents’ attitudes were traditional and restrictive, limiting women to homebased roles and devaluing all others.
There was considerable variation when housewives were asked what entrance into marriage had meant for them. Some saw it as primarily a change in the pattern of life: “Marriage has been the biggest change—women have a much more distinct change in their lives than men do” (p. 83). Women who had married quite young thought that marriage had resulted in a change in themselves: “I went into marriage spoiled and opinionated, and I had a great adjustment to make to a mate. I have learned to be more tolerant, patient, and to expect less of myself and others” (p. 83). Interestingly, some women related marital status to personal independence, others to an unaccustomed dependency. These two quite different perceptions are illustrated in their comments:
Since I have been married, I’ve had to adjust and make a few changes. You have to learn to share. It’s different from when you’re home with your brother and sister. You have to learn to give as well as take; to learn to be more independent. I don’t depend on my folks as much as I used to (p. 84).
Life has gone from independence to dependence. Before marriage I did what I wanted. Now, I am dependent on my husband. In the future, I will become more and more dependent as the kids grow up and move away (p. 84).
Likewise, some women felt freer after marriage; others before. The former saw it as an opportunity for independent action; the latter, as a giving up of personal control over oneself and the assumption of a burden of responsibility.
These varied views of the difference marriage makes for women are not at all contradictory; rather, they reflect individual personalities and background, as well as the way the woman feels about her current situation. For example, a young woman whose parents had been oppressive in their concern and protection of her might see marriage as a declaration of independence, as an escape from the status of dependent girlhood to the elevation of equality with her own mother. For another, the move from dependence to independence might be economic. Economic dependence on a husband is not necessarily the same as economic dependence on a father. From dependence on the latter’s largesse or lack of it, she might move to a situation where the paycheck is handed to her and she is the arbiter of how it should be spent in the best interests of the new family unit. When marriage is viewed as movement in the other direction, from independence to dependence, again the meaning of the terms for the individual must be considered. A young woman may first experience strong emotional dependence when she moves away from her family and friends to a strange city, and has only her husband to meet her needs for reassurance and personal contact. One who has had her own job and apartment, and freedom to come and go as she pleased, might feel keenly deprived of these after the honeymoon is over.
When the Chicago-area women were asked, “What are the roles, in order of importance, of the man of the family?” there was impressive agreement among suburban, urban, and working women: his main role is provider for the family, followed by father and husband. In fact, the role of man as provider was mentioned more often than the role of woman as mother, indicating a greater consensus among the women in their view of the role of the male.
The women in this study saw the role of the family man today as very different from that of his counterpart three generations ago. The changes, they thought, were focused on a shift in his relation to the entire family. Older, less educated respondents emphasized his loss of power; he is no longer “lord and master.” A second group saw the relational change as more than a dethroning of the patriarch, rather involving a redistribution of authority toward a more democratic alignment. The more educated women spoke of changes in the quality of the relationships, using such phrases as “more understanding,” and “more interested in the family.” Across all variables of age, housing, and residence, however, the higher the education of the woman, the more positive she was in describing the changed role of the man in the family.
While the tradition of the male as provider and the female as domestic manager and worker is less rigid in many families today than in the past, it is still common to observe that many household jobs have sex labels. For example, the man of the house may wash dishes, do the laundry, and run the vacuum cleaner, but he does not usually do the family ironing or sewing. Furthermore, it is usual to view the husband’s participation in these kinds of activities as “helping” his wife, a linguistic convention which plainly reveals whose job it really is. In the same study, women were asked specific questions about the kind of help they received with household tasks. Approximately two out of three husbands helped at least part of the time with such tasks as family finances, care of children, and shopping. However, only about one in three ever helped with such housework as cooking, cleaning, and laundry.
The higher the income, the more likely the husband was to have sole responsibility for managing the household finances; the wife usually received an allowance for those expenditures that were her responsibility. In very low-income homes, where most of the money went for necessities such as food and rent, the woman usually had charge of its allocation. While most fathers with young children helped with their care at least some of the time, we do not know how many were sharing a parental responsibility and how many were helping the mother with “her” children.
The role of mother
Occurring usually after a woman has assumed the roles of wife and housewife, the role of mother is seen by most women as the most important in the life of the adult female. The responsibility for the care and socialization of the young and the feeling of importance deriving from that responsibility are major sources of satisfaction and self-esteem for many women, at least while the children are young. But this is only one part of the montage of feelings about motherhood that can range from despair to ecstasy. The desire to have children and an interest in rearing them is by no means universal among women. Some are deciding to forego the experience altogether, a decision which would have been considered selfish if not actually sinful a few decades ago. More common is the decision drastically to limit the number of children borne. Although the role of mother dominates much less of the life span of women today, its assumption, especially for the first time, is a major life-changing event.
It is only within the past decade that women’s emotional experience of mothering has received attention in psychological research. Instead, researchers have looked at motherhood from an instrumental (masculine) perspective: how mothers’ behavior affects offspring, and what mothers should do to produce healthy, adjusted children. When the focus is changed from mothers’ effects on children to motherhood as woman’s experience and identity, then the questions asked in research change (Gerson el al., 1984). Here we are more interested in the effects on women of the role of mother, recognizing that the two issues are closely related.
As we saw in Chapter 1, the romanticization of the mother role was a feature of popular American culture during the late nineteenth century, and vestiges of it still survive in Mother’s Day celebrations. The early feminists were not ready to attack the mother role, nor to abandon it themselves, but they were well aware of the restrictions it imposed on their own activities. Susan B. Anthony, who was childless, was open in her disapproval of the large families of her feminist friends, as in this excerpt from a letter she wrote to Antoinette Brown in 1858:
A note from Lucy last night tells me that you have another daughter. Well, so be it. I rejoice that you are past the trial hour.
Now, Nettie, not another baby is my peremptory command, two will solve the problem whether a woman can be anything more than a wife and mother better than a half dozen or ten even (Rossi, 1973, p. 383; italics original).
Charlotte Perkins Gilman, writing in 1898, saw clearly the irony in the contrast between the adulation of the mother role and the oppression of women:
An extra-terrestial sociologist studying human life and hearing for the first time of our so-called “maternal sacrifice” as a means of benefitting the species, might be touched and impressed by the idea. “How beautiful!” he would say. “How exquisitely pathetic and tender! One half of humanity surrendering all other human interests and activities to concentrate its time, strength, and devotion upon the functions of maternity! To bear and rear the majestic race to which they can never fully belong! To live vicariously forever, through their sons, their daughters being only another vicarious link! What a supreme and magnificent martyrdom!” (Rossi, 1973, pp. 589–590).
The childbearing histories of most women, however, were less effected by feminist ideology than by medical technology and environmental concern with an emerging belief that it was more acceptable to have few children than many. Even so, as late as 1962, a Gallup survey of the American woman found that childbirth was ‘the most thrilling event” in the lives of half his sample. One woman explained, “You’ve done something that’s recognized as a good thing to do and you’re the center of attention” (Rossi, 1964, p. 152).
Although today’s young women will have fewer children and will spend less of their lives mothering, their role of mother will continue to be the most important focus of their lives when their children are young. The reasons for this are not innately determined by a “maternal instinct,” but result from certain conditions of contemporary society. The first of these is that the care of the infant and young child is relegated almost entirely to the mother. While there are many exceptions, it is still normative for the father to be away at work during the day while the mother cares for young children who are not yet in school. Thus most of her waking hours are spent with her children, for whom she has the ultimate responsibility. The present mores still favor the mother as primary caretaker, even in the absence of clear evidence that such an arrangement is necessary or even desirable for the well-being of the children (Hoffman, 1974).
The centrality of motherhood to woman’s identity has been called the “motherhood mandate” (Russo, 1979). According to the mandate, a woman should have at least two children and raise them “well.” This obligation comes first, even if she is active outside the home. “A ‘good’ mother must be physically present to serve her infant’s every need. As the child enters school, a mother may pursue other activities—but only those permitting her to be instantly available should her child ‘need’ her” (Russo, 1979, p. 8).
Another reason for the salience of the mother role for young women today is the central role of children in the family. With fewer children, and more leisure and affluence, parents can afford to view each one as unique and precious, to consider him or her as an individual who has a “right” to gratification of needs in the best possible environment. Parallel with this development and contributing to it has been the burgeoning of information and guidance contributed by the medical and behavioral sciences, advising mothers on every aspect of child care and impressing upon them the importance of their role in personality development and in the growth of healthy children. Studies by Bowlby (1960), Spitz (1946), Harlow (1967), and others were interpreted by writers for the lay public as proof of the damage that could be caused by inadequate or improper mothering, and this was translated into a popular belief that the child was best cared for by its own mother all the time. The notion that a mother of young children who does anything else on a regular basis other than care for them is guilty of neglect continues to be so influential that every counselor and clinician is familiar with the guilt and selfcastigation felt and experienced by the mother who goes back to work or school while her children are still young.
Since the mother has most of the responsibility for care of the children, and since the children are very important, it follows that their physical and emotional well-being are often attributed to her interaction with them. If children have problems, it is almost always the mother who is blamed for them, on account of the enormous influence she is believed to have over them. Such prevailing views about child development have a very sobering effect upon the behavior of young mothers and inevitably upon their extrafamilial aspirations.
When asked about the consequences of becoming a mother, women defined several major areas which could be identified as directly resulting from the event of motherhood (Lopata, 1971). One of these was a redefinition of one’s identity, meaning an abandonment of one’s own interests into a necessary service of the interests of the dependent one, the infant:
When you are married and have small children, you have a lot of things you would like to do but can’t; you don’t have time and facilities. If I could, if I had peace one-two hours a day, I would continue voice, buy a piano, study. Sometimes 1 feel lost in the shuffle, confused; not the make-a-meal self, but as if 1 lost identity ... (p. 192).
Another consequence was described as a more positive change in the self in the direction of greater maturity and ability, and a growth away from selfishness and childishness. These women saw themselves as becoming more responsible, as acquiring traits associated with adulthood as they had to adapt to the needs of others and learn to tolerate frustration.
A third consequence was expressed in terms of a constriction of one’s personal world, of being “tied down” by the responsibilities and demands of young children. Future changes anticipated by the women envisioned more freedom to do things they wanted to do, and to have more time, both for themselves and to be with their husbands: “More tied down now, hope to have more freedom later ... my life is not my own. The demands of the children take time and I have less time for myself.... 1 wish I would get out more” (p. 195). For some of the women, special circumstances entered into their perception of the changes effected by motherhood: having a retarded child, for example, or taking on the rearing of a grandchild at the same time that one or more of her own were young.
Another consequence was the extra labor required for the care of children, leading to changes in other social roles, such as housewife: “When I first married, I was exacting about the house, exact time and spotless; as I had children, I realized that this is not the most important thing; picking on children—vicious circle ... I learned not to be exacting” (p. 197).
Attitudes toward having children have undergone dramatic changes in recent times in our society. In the 1950s couples who chose to remain childless met with disapproval. Bv the 1970s this negative moral judgment had disappeared. Individualism and selfrealization were the dominant values, and many young women viewed having children as incompatible with their newly won freedoms. At the least, children could be postponed until one had reached one’s educational and career goals. In the 1980s motherhood again became salient as the careerists of the 1970s began to reach the age of thirty and the realization that there were biological limits on the timing of pregnancy and motherhood. The rate of first births to women past thirty began to climb. The salience of motherhood was rediscovered in parenthood, and new studies began to appear.
One of these surveyed patterns of work and relationships of three hundred women between the ages of thirty-five and fifty-five. Of concern were the questions, What makes a woman feel good about herself as a member of society who is in control of her life (Mastery)? and What makes a woman find pleasure and enjoyment in her life (Pleasure)? A critical finding of the study was that whether a woman did or did not have children had no significant impact on her wellbeing, on her sense of either Mastery or Pleasure.
This is especially interesting since the women in the study grew up in a pronatalist era, so that one would expect the childless women to experience negative consequences. But this was not the case. “I thought at twenty-five that I’d be miserable at forty if I didn’t have children,” says one woman. “I’m happy to discover it isn’t so at all” (Baruch et al., 1983 p. 81).
The study found that the rewards of motherhood were associated with two different mothering styles. The first was called “autonomous” and included the following:
-
Liking the kind of people your children are
-
Feeling proud of how they turned out
-
Enjoying doing things with them
-
Seeing them mature and change
These mothers focused on the children as individuals separate from themselves, whose individuality was a source of pleasure. These mothers were more likely to have a Erm sense of their own identity and to be able to nurture their children without living through them.
The second style was called “coupled,” reflecting the importance of the child to the mother’s own sense of identity. It included these rewards:
-
Children give meaning to your life.
-
Children provide a sense of being needed.
-
Being the best caretaker for a child gives you a sense of being special and irreplaceable.
The more a mother endorsed the autonomous rewards of being a parent, the higher she was in Mastery and Pleasure. By contrast, the more coupled she felt to her child, the lower she was in Mastery. The authors noted the risk for women of depending too much on children for one’s self-esteem and sense of value. The more autonomous mother can equally enjoy her children without being overinvolved with them and making them responsible for her feelings of worth (Baruch et al., 1983).
These mothers, like those in the earlier Lopata study (1971), reported on problems they had in the mother role. The unending demands of young children, not being able to control older children, arguments and conflicts with them, and lack of appreciation from children-—such concerns caused some to question themselves, out of fear that they were being bad mothers. While conflict with children caused the sense of Mastery to drop more in employed mothers than in at-home mothers, there was no difference between the two groups in the balance between how positive and how negative they felt about being mothers (Baruch et al., 1983).
Satisfactions and problems, joy and pain. Motherhood is supposed to bring woman her greatest fulfillment, yet little is said about its darker side. No one has more poignantly captured the ambivalence felt by many women for our oldest role than poet Adrienne Rich in her 1976 book Of Woman Bom. In an entry from her journal, written when her sons were young, she said:
My children cause me the most exquisite suffering of which I have any experience. It is the suffering of ambivalence: the murderous alternation between bitter resentment and raw-edged nerves, and blissful gratification and tenderness. Sometimes I seem to myself, in my feelings toward these tiny guiltless beings, a monster of selfishness and intolerance.... And yet at other times I am melted with the sense of their helpless, charming and quite irresistible beauty.... I love them. But it’s in the enormity and inevitability of this love that the sufferings lie (Rich, 1976, p. 22).
While in the long run children are a great source of satisfaction to many parents, their arrival and their presence in the household can impose serious strains on the marriage of their parents. A national survey conducted by the University of Michigan’s Institute For Social Research[42] found that young married persons without children were happier than were those with children. Eighty-eight percent of the childless wives and 73 percent of the childless husbands between the ages of eighteen and twenty-nine said that they were “generally happy with life as a whole,” compared with 65 percent of the husbands and wives with children under six. Contentment dropped and stress increased when the couples had their first child. As the children grew older, marital happiness increased and continued to increase after children had left home. Studies on marital satisfaction over the life span reveal a U-shaped relationship between satisfaction and time period, with satisfaction scores being lowest when children are young (see Fig. 10.1).
Similarly, a study of 2,480 married couples in an urban California sample found that rates of marital satisfaction and physical wellbeing were highest for childless couples, followed by parents whose children had left home. The most problems, both psychological and physical were reported by couples with children at home, regardless of the duration of the marriage and the wife’s age and employment status (Renne, 1976).
The blame for this situation should not fall altogether on the fact of parenthood, however. During this period, other conditions contribute to difficulties of adjustment, and the advent of one or more children may exacerbate stress from other causes: economic strains, in-laws, and clashes of cultural backgrounds, personalities, and expectations as two relatively immature and inexperienced persons learn to live together.
Today, theoretical and empirically based discussions of woman’s traditional roles have implications far beyond the academic arena. They stir up or accompany clouds of controversy that prove the importance of the issues involved. At a conference on the older woman in America, for example, a psychology professor stated that sex roles are based on parenthood, which mediates different role directions for males and females: the provision by males of physical security, and by females of emotional security for the young. Questioning and experimenting with familial roles, and a quest for self-fulfillment, must take second place to the emotional development of young children. The post-child period of freedom is time enough for more open discovery of the self, for psychological release, for liberation. In total disagreement a social worker replied that waiting for post-child freedom is not tenable to today’s woman; forty or fifty is too late to make changes in the self-image or to begin to develop in new ways. Roles are not an immutable function of biology; rather, women are socialized to be as they are, and few are allowed to develop capabilities beyond those ascribed to them by role stereotypes (Uits, 1974).
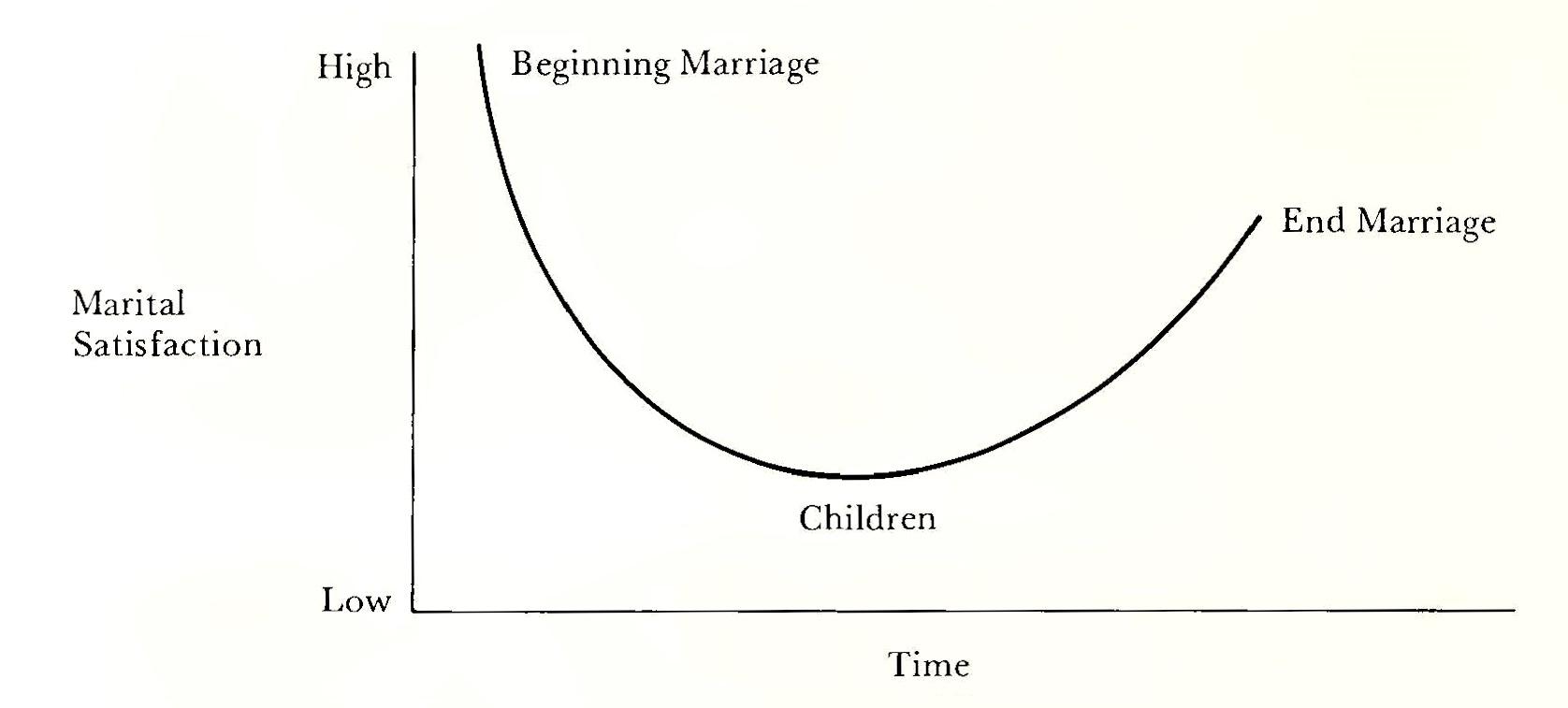
And so the argument continues. More than thirty years ago, the behaviorist B. F. Skinner, in Walden II, proposed the complete emancipation of women from family roles in a new kind of community in which the role of mother, while still performed by the woman, would have “no more connection with her daily work than the role of father with his work in the office or factory or held... As for housework, “[T]he intelligent woman sees through it at once, no matter how hard she wants to believe. She knows very well that someone else could make the beds and get the meals and wash the clothes, and her family wouldn’t know the difference....” But in Walden II, the place of women has been radically changed: “Some women feel momentarily insecure for that reason. But their new position is more dignified, more enjoyable, and more healthful, and the whole question of security eventually vanishes” (pp. 121—22). We may be in transition to Walden II, but we are not yet there.
New Ways to Live
Tradition dies hard, and it is safe to say that a majority of adult women will continue to have as a significant part of their personal history a participation in the roles we have just described. But running through the recent history of human relationships and institutions is the bright thread of revolution, and marriage and motherhood are no exceptions. Marriage and the monogamous nuclear family have been the subject of bitter attack by feminists who see them as major vehicles for the oppression of women. Furthermore, the viability of the traditional marriage relationship as a setting within which individuals can freely grow into their full potential has been seriously questioned, especially by younger, better educated people. Is marriage still a desirable goal? Is marriage ever compatible with freedom and equality? How can marital roles be shared? Not only are these questions being answered, but the answers are empirical, coming out of active experimentation with a variety of life styles reflecting more or less faithfully the ideology of individualism, with its values of personal freedom, self-expression, self-direction, and exploitation of the growth possibilities in a variety of relationships.
The ultimate demise of the patriarchal type of nuclear family symbolized by the phrase “man and wife,” in which the man was the “head of the household” and the wife was subservient and economically dependent, was evident by the middle of this century because of “the ESE factor” (O’Neill and O’Neill, 1972). This factor consists of three components: educational, sexual, and economic freedom for women. While none of these freedoms had emerged fully at midcentury, nor yet, for that matter, the precursors were identifiable in the technological modifications of home life and in woman’s performance outside the home during and after World War II. Education broadened her interests to the world outside the home, opening the door to the possibilities of work and career; birth-control technology largely liberated her from biological imperatives and gave her a measure of control over her own body processes; and economic freedom, achieved through access to education and jobs, meant that she need no longer settle for old dependency roles. Not only has the ESE factor moved women closer to the goal of equality, but it is “the single most important force affecting change in today’s marriage styles” (O’Neill and O’Neill, 1972, p. 195). The realization of these freedoms for women has the potential to make new life styles possible and to fundamentally alter the traditional marriage relationship. Among alternatives to traditional marriage which have already appeared and are being practiced by women and men are the single life, cohabiting without marriage, and communal and other group forms of living together.
The proportion of women remaining single until they are between twenty and twenty-four years old has increased by one-third since 1960. The number of unmarried women and men living together quadrupled between 1970 and 1985.[43] Statistics on marriage have fluctuated in the past, as a response to war, economic conditions, and changes in life styles, but these recent changes reflect a complex set of circumstances that are new in American life, important among which are changes in the role of women.
“Better dead than unwed” once described the unhappy future in store for a single woman, and not without reason in a time when marriage provided the only path to security that the average women could hope for. The socialization process which left little doubt that marriage was the only acceptable outcome for women was reinforced by the veritable lack of alternative ways of spending one’s life productively. When attractive alternatives are available, women are much more likely to delay marriage or to stay single (Bernard, 1971b). Marriage rates are higher among women who are unemployed, and the higher the level of the job and the income, the lower the rate of marriage. As more women develop the values of autonomy and independence, the feasibility of a single life style should improve. Other factors that promote the delay or rejection of marriage are the climate of acceptability which has evolved with the now widespread practice of single persons living together, and the emergence of a singles identity, an awareness by the single person that one is a member of an identifiable group with a legitimate life style (Moran, 1972).
Living the life of a single woman in contemporary society or living with a man in a relationship free of the traditional bonds of marriage does not necessarily convey liberation from sex roles, however. Role assignment on the basis of sex can be a feature of the most sexually liberated social or living arrangement. For example, females in “singles” society found that it catered to men, who still had the option of doing most of the pursuing and choosing from among eligible women (Moran, 1972). College educated couples living together and both working often retain vestiges of the old roles when it comes to housework. Terry and Chick were such a couple. “Like any young housewife, she does most of the cooking, shopping, and laundry. Chick fixes their car....” I seldom identify with movements,’ says Chick, and Women’s Lib is no exception.... [M]any of the premises are unfounded and incongruous’ ” (Coffin, 1972, pp. 316–17).
Even though one marriage in two now ends in divorce, marriage is still thought of as conveying status on a woman and providing economic and emotional security. Does marriage have anything other than these advantages to offer women? It is possible to have emotionally and sexually satisfying relationships without marriage. In an increasingly permissive society it is even possible to have children outside marriage either by having one’s own or by adoption. As the number of independent and adventurous women increases, and as role models for the single life become more visible, more may opt for a life that is free of the explicit and implicit commitments marriage has always meant.
Open marriage
Open marriage is a relationship of intimacy based on equal freedom and identity of both partners (O’Neill and O’Neill, 1972). Involving a departure from rigid conformity to the established husband-wife roles, its realization is dependent upon the equality of women and men, and therefore it may be viewed as a logical consequence of the change in the status relations of the sexes caused by the appearance of the ESE factor. Freed of power inequities in the relationship, the couple is able to implement other values which expand on the concept of equality. A woman may have full equality with a man in their society, yet not have an open marriage, but she cannot have an open marriage without equality. Since equality of women with men is only now possible for the first time in history, open marriage is also only recently possible.
The open marriage model has two purposes: first to provide insights on the closed, or traditional, marriage patterns, which presented few options for choice or change; and second, to provide guidelines for developing an intimate marital relationship within which both partners can grow, each supporting the other.
The patterns of traditional marriage include certain expectations, ideals, and beliefs which are impossible fully to realize. These include the ideas that one mate belongs to the other, that one will always “be true,” that the ultimate goal of marriage is to have a child, that each plays a different part as a function of biological sex, and that one’s spouse can fill all one’s needs, economic, physical, intellectual, and emotional. The values in such a relationship of exclusivity, possessiveness, endurance, and security, give it a static quality which inhibits growth and spontaneity, and stifles creativity.
Open marriage, by contrast, includes the expectations that both partners will change; that each will accept responsibility for self and grant it to the other; that one’s mate cannot fill all one’s needs; that the partners will be different persons, not because one is a husband and one is a wife; that children are not needed as proof of love for each other; that liking and loving will grow out of the mutual respect that the open relationship allows. These expectations reflect the values of individual freedom, flexibility, personal growth, and “undependence” within a dynamic, responsive relationship. Theoretically, the model represents the application of the concept of the self-actualizing environment to marriage (Maslow, 1954). This concept encourages growth to the fullest of human potential. Hence, a couple can go beyond the more traditional relationship, whose form and role requirements can be restrictive to such growth.[44]
The achievement of an open marriage depends upon using guidelines which interact with each other in ways that are mutually augmenting. As a basis for a style of interpersonal relationship between the sexes (although equally applicable to other relationships as well), these guidelines reflect values that are clearly contemporary:
-
equality: the respect for the equal status of the other, in contrast to the status differences inherent in traditional man-woman relations;
-
role flexibility: the sharing or exchange of role-associated tasks, both household and economic;
-
open companionship: each partner having the freedom to relate to others, male or female, outside their own marital unit (this is seen as an auxiliary facilitator of growth, not a replacement for the primary relationship of the marriage);
-
identity: the development of the individual through the realization of potential and the growth toward autonomy;
-
privacy: each having personal time and space to be alone when she or he desires it. This is in contrast to the “togetherness” mystique fostered by earlier values;
-
open and honest communication: discussion that is expressive of one’s real feelings, free of defensiveness and the kinds of minor deceptions that are learned in the process of growing up;
-
living for now: relating to the mate within the present emotional and intellectual climate. Reflection on past glories or calamities, or fixation on future materialistic goals will diminish the personal self which exists only in the present.
-
trust: an outgrowth of the practice of the other guidelines based on respect for the integrity of the other.
Open marriage is still marriage conceptualized within the framework of a primary relationship between two persons implicitly (though not necessarily) male and female, who have a personal commitment to each other which may or may not be legal as well. The factors of sex of the participants and of legality are irrelevant as far as the application of the principles is concerned, but the intention of the developers of the model is to present and to encourage new kinds of behavior in a marital relationship, to bring marriage out of an obsolete form into one compatible with contemporary egalitarian and individualistic values. Thus it would modernize, not abandon or abolish, the old institution. Its success depends upon the capacity of the persons involved to free themselves from the stereotypes which almost everyone growing up in our society so far has learned, and actually to implement the values which underlie such a marriage.
Proponents of open marriage point out that the separation of roles into “his” work and “her” work makes little sense in today’s world. Assigning the total responsibility for the provider and managerial role to the male places a heavy burden of stress on him which not all men are capable of handling and deprives him and the children of each other. The assumption that the wife will have the main domestic responsibility places many women in a role which underutilizes their abilities and restricts their development. They recommend role flexibility, whereby each person can share in both occupational and parent roles, working out an agreement compatible to both. Some couples might find a reversal of roles to their liking, with the man staying at home and the woman working. Or they might exchange chores, she balancing the checkbook, he doing the laundry. The basic idea is that both housework and wage earning must be done, that paid work is not necessarily more valuable than unpaid work, and that couples can work out an equitable agreement which recognizes the talents, wishes, and needs of both.
Clearly the young, less fettered by the past, are more likely to be able to do this—and so are those in increasing numbers who have been through the old route and know its traps. It is hard to imagine any significant acceptance of such a model with all its implications by couples who have been married for two or three decades and who have made their adjustments to their marriage and to each other. Not necessarily unhappy, they may feel no need for change at all, and indeed might be quite threatened by such ideas as these. For the male, such change would include giving up a position of power, dominance and authority, and the right to exclusive possession of his wife; for the female, the loss of her dependency status with its guarantee of protection and material security (for as long as the marriage works!). It would require a dissolution of role limitations and the cultivation of undeveloped aspects of personality. Attempts at such change can provoke high levels of anxiety which some persons cannot or will not tolerate. But it may be for many an attractive alternative to a lifestyle with which traditionally there has been very little competition.
While open marriage offered a theoretical model for marriage in the 1970s, a study of the patterns of women’s lives indicated that some of its elements have become incorporated as positive values for contemporary marriages. “Today the marriages that women describe as highly rewarding are ones that are more like partnerships between loving friends than they are like teams of oxen yoked in gender-harnessed roles” (Baruch et al., 1983, p. 61). In these good marriages, the women saw their husbands as supportive of their interests and activities, men who saw their wives as “someone special” and someone who could empathize with their problems. Too, their husbands were willing to share in child care and housework, a far cry from the Victorian ideal marriage, in which women were supposed to be submissive handmaidens to their husbands.
A critical factor in effecting the change to today’s model for marriage, with its different expectations of the partners, is the economic situation. Women’s paychecks have become very important to the comfort and even to the survival of a majority of American households. The increase in employment of married women has been accompanied by stress for many households. It is simply not possible for a woman to function in the traditional housewife role and work full-time outside the home. Many women resent coming home to another full-time job of caring for husband, house, and children. Not only help is needed, but emotional support as well, in the form of recognition and appreciation. In successful marriages, men have been able to give up some of their prerogatives, such as exemption from the mundane tasks of housework and child care, and to participate in the accomplishment of these as their wives participate in the role of provider (Baruch et al., 1983).
Alternatives to marriage
Recent years have seen a proliferation of alternatives to marriage. The most robust of these seems to be the delay or rejection of marriage by staying single, living with another person in a quasi-marital relationship (without the legal involvement), and certain forms of group commitments or communal arrangements with a common ethos and common goals. What each of these will mean for women remains to be seen. It is plain, however, that the trend is for increasing freedom and flexibility of choice of life style on an individual basis.
The single life. Deferral of marriage or rejection of marriage altogether is becoming increasingly common, especially among more educated, middle-class women. Obviously there is a strong connection between the decision, to live one’s life alone and economic independence. The more resources a woman has, through education and employment, the more feasible it is for her to contemplate a life of being dependent only upon herself, or at least until such a time that she feels ready to make a free choice about sharing her life with someone else. It seems likely that deferral of marriage will be attractive to more women than the rejection of marriage altogether. The decision to delay marriage until one reaches the late twenties or thirties has several advantages. One can complete one’s formal education, become established in a career, and taste the joys of accomplishment and independence. Maturity and a sense of one’s identity are more likely to come with these experiences. Too, the restrictions on freedom imposed by marriage and motherhood may seem less onerous, or insignificant even, to one who has freely chosen them.
The decision to remain single forever does not seem to be competitive with marriage as a preferred way of life for most women. It was not uncommon in the nineteenth century for affluent women to eschew marriage entirely, and through the ages women of all classes have escaped marriage by joining religious orders. Complete freedom of choice for large numbers of women, however, is only recently feasible, and the meaning of this is still unknown. Adult women who are single cite both positives and negatives for their situation. They are free to do as they please without having to defer to another person’s wishes. They are spared the burden of raising children. They can spend their money as they choose and have more of it for themselves. They can design their lives as they wish and come and go freely. On the other hand, they speak of loneliness, of the restricted social life of the single woman, and of the prospect of growing old without a family of one’s own. Too, some miss the pleasures of sharing life events with an important other, of the mutual planning and achievement of family life. Even so, the single life appears to be conducive to mental health. A large sample study of depression and marital status found that single women heading their own households had significantly lower scores for depression than did married, divorced, or widowed women (Radloff, 1980).
When Grace Baruch and her colleagues (1985) looked at the never-married women in their study of life patterns of women aged thirty-five to fifty-five, they found that work played a crucial role in these women’s lives. That is, for the single woman, the type of job she had was strongly related to how she felt about herself. The single woman in a high-prestige job was likely to have high well-being, but the woman who had neither marriage nor a satisfying job was likely to be low in a sense of mastery, of being in control of her life, as well as in a sense of pleasure, finding life generally enjoyable. This is not difficult to understand, since the fewer roles a person has in life, the more central to her psychic well-being are the ones that she does have. Too, the issue of preference emerged as significant. The women who said they preferred being single were high in wellbeing, whereas those who wished they were married were low in both mastery and pleasure.
Another difference that emerged was that single women saw themselves as more assertive and independent than did the married women, and they valued achievement and personal growth more. By contrast, the married women valued interpersonal relationships more. The rewards of being single were reflected by the never-married women’s endorsement of such items as:
-
Not being accountable to anyone
-
Being independent
-
The lifestyle suits you
-
Being able to do things spontaneously
-
Not having too heavy responsibilities
By contrast, the women who scored low in well-being were those who felt stigmatized by being single, who has little sense of autonomy or control owing to being in low-level jobs that gave them little satisfaction. One said, “I find that a big stigma in my life, being single. You have the feeling of never having been chosen and it makes you feel you’re worthless” (p. 219). This woman was in an unrewarding job that she disliked, and she had few sources of support.
A major theme among the concerns of single women was related to need for others. These women endorsed such items:
-
Not having a permanent relationship
-
Difficulties meeting men
-
Sexual relations a problem
Single women do not usually have “built-in” companionship in the form of mates and children. Thus these women had to exert more effort to develop friendships and to ward off feelings of isolation. Even so, many of the women in the study felt good about themselves, having learned that walking “single file” does not doom one to be lonely and unhappy, but that it can in fact lead to the full and rewarding life that is the goal of most (Baruch et al., 1985).
Living together. Most people have some basic needs that can only be met within the context of close relationships with others. Needs for intimacy, for trust, and for sharing are served by living with another caring person. It is now commonplace for men and women to live together without the legal commitment of marriage. Such arrangements offer many of the advantages of marriage, such as companionship and sexual intimacy, without the implication of union and permanency. Compared to marriage, these arrangements are easier to dissolve, though the emotional trauma of parting may be just as severe. There is no prototype for a “living together” relationship. It may last weeks, months, or years and may culminate in marriage. In fact, one of the most commonly observed situations is the couple who are living together in anticipation of marriage at some future time—when one or both finishes school, when careers stabilize, when they want to have a child. Once an option for the adventurous young, especially on or around college campuses, “living together” is now an alternative to marriage for all ages and among all segments of the population. For a woman, living with a man in a nonmarital relationship means trading the possible security of the traditional marriage for looser ties and lesser commitment, suggesting greater freedom and equality. But here again, variation is the rule; roles and couples’ ways of relating to each other seem to be as diverse as those found in marriages.
Group marriages and communes. Among alternatives to traditional marriage are those in which several adults of both sexes live together with a quasi-marital bond of commitment. Group marriage involves at least three individuals, each of whom is “married” to at least two other members of the group. A study of sixteen such groups revealed that the members were motivated by personal growth opportunities and by interest in having a variety of sexual partners. Some interesting findings emerged with regard to roles and gender differences. Sex roles were much less differentiated than in the average nuclear family. Men took care of children and did some of the housework, and women were involved in careers and education. Individuals tended to specialize in certain tasks; one woman kept the books, another was the correspondent, while someone else organized the child care. But the residual work that no one wanted to do usually fell to the person who was least assertive or had the highest need for order—both more likely to be women (Constantine and Constantine, 1974).
Communes and communal living arrangements began to appear in the mid-1960s and have been widely observed and studied. Such experiments in collective living have a long history in American society. More than two hundred were founded in the nineteenth century alone (Muncy, 1973). Families and tribes have always been the most common interest groups, and the renewal of interest in communal living may be the desire to return to an extended family or tribal grouping (Ramey, 1974). The purpose of communes may be economic, political-revolutionary, religious, or for sexual liberation or personal psychological development. A few espouse the principles of sexual equality and attempt the obliteration of roles based on sex, though in general they vary widely with regard to sex role differentiation. As in other forms of living arrangements, much depends upon whether or not children are involved, and the extent to which women are economically productive. In general, the literature on communal living has not suggested any radical departure for women from their traditional roles of housework and child care.
The option of some for innovation in personal relationships should be viewed in the total context of our society. Marriage and conventional expectations for it are still very popular, even if one in two do not work out. But very powerful social, political, economic, and technological forces are producing at the very least a new alignment within the old format, and it seems unlikely that things will ever be the same again. In summary, these forces interact with each other and affect women, men, and marriage:
-
Technology has freed women from household drudgery and unwanted pregnancies, thus reducing in importance the old roles of housewife and mother.
-
Liberalization of divorce and abortion laws reflects a lifting of old oppressive sanctions which maintained traditional roles.
-
Changing views on sexual morality, with increased emphasis on permissiveness and individualism, and decline of the double standard.
-
The women’s liberation movement with its egalitarian and revolutionary goals is supporting educational and economic equality, and optional independence of women from men and children. The movement has also given women some relief from the onus of staying single or of being homosexual.
The effects of these changes will touch almost everyone as old patterns yield, and in the absence of new repression, a truly pluralistic society emerges.
The Future of Motherhood
But what about motherhood, the oldest role of all, in the brave new world? Some see a continuing erosion of the role as technology removes many of its tasks from the home, and a decline in its importance as women have fewer children and more time for other activities, especially jobs and careers. The new scenario for the role of women as mothers is no minor concern, attended to after important matters such as defense and the balance of trade; rather, it is the heart of the matter, a momentous project relevant to the future of the species. Most women will have children, but institutions and fathers will find they must get more involved in their care as women spend less time in the home. A synthesis will evolve in which the principles of “male” strength and “female” nurturance will be found in both sexes, rather than separately specialized in one or the other. Mothering will be a craft for those who enjoy it most, of either sex. Free of the distorting effects of role specialization, “the individual human will be able to develop the psychic wholeness that is urgently needed” if Western society is to face the dangers that lie ahead (Bernard, 1974, p. 365).
This is indeed a grand vision and one whose realization is far in the future. The reduction in numbers of children that women bear, the diffusion of roles, and the availability of alternatives to mothercare must proceed in parallel before the mother role will be significantly affected. Many women will be interested in such alternatives. At the present time, it appears that the first of the three components is proceeding more rapidly than the others. And the second, role diffusion, cannot occur unless surrogate care releases women from some part of the demands of the role.
The research on day care, communal arrangement, and other types of surrogate mothering cannot be reviewed here. But 90 percent of children under six whose mothers worked were in “informal” kinds of care—by friends, neighbors, and other non-kin who were paid for their services. Those in “formal” day care, such as non-profit centers and commercial facilities, were exposed to a wide variety of quality of care; indeed, quality varied greatly within the various kinds of arrangements, both formal and informal (Emlen and Perry, 1974). And still, the biggest problem of the working mother with young children is, who will take care of them? how much will it cost? if I leave them, will it help them or hurt them? what happens when they are ill? and on and on. The long conditioning of women to feel that they are solely or primarily responsible for their children, even if someone else has them part of the day, is not likely to be extinguished quickly.
Voluntary Childlessness
In contrast to the motherhood mandate is the relatively recent and growing phenomenon of voluntary childlessness. In 1976 the Census Bureau reported that three times as many wives under thirty expected to remain childless in 1975, 4.6 percent, as in 1964, 1.7 percent (Kearney, 1979). In earlier times, the childless married woman was thought to be either barren or selfish. Neither of these was socially acceptable, reflecting again the identification of woman with her biologically ordained destiny. Thus, the woman today who chooses not to have children is flouting one of the oldest traditions of all for her sex.
Why would a woman make such a choice? One study of sixty-one childless couples found that career and income considerations were the most important factors in making the decision not to have children (Silka and Kiesler, 1977). But these may in part be rationalizations for factors in the earlier socialization of some such women. A recent study looked at two different types of voluntary childlessness: women who decided early in life, before marriage (early articulators), that they would not have children and women who decided after they had married and developed a lifestyle that did not include children (postponers). The major differences between the two groups were in family background factors and reference-group support. The early articulators reported more psychological distance between themselves and their parents, less warmth in the family, more stress on achievement, less democratic discipline, and less encouragement by parents of assertive autonomy. Also the early articulators had depended less on reference groups in making their decision. Interestingly, the early articulators and their husbands were more than twice as likely as the postponers to have undergone voluntary sterilizations, which may be taken as a measure of their commitment to their decision (Houseknecht, 1979).
So, while desire for a lifestyle free of the demands and responsibilities that children bring may motivate some to refrain from experiencing the mother role, others may be more influenced by their own experiences of childhood and the meaning to them of family life.
The childless women in the study by Baruch et al. (1985) of women aged thirty-five to fifty-five were childless for several reasons. Some had decided not to have children. Others were not able to conceive, and others just “drifted” past the time for childbearing. Those who were voluntarily childless for the most part were satisfied with their lifestyles. Others seemed resigned, along the lines of “It might have been nice, but ...” Like parenthood, being childless had for these women both rewards and regrets. Rewards included being able to be spontaneous in one’s life choices, freedom to do what one likes, and exemption from the financial and emotional demands that children represent. Also, childless married women thought that the absence of children made their marriages more special: “I see a lot more of my husband—there’s no interference. I’m not taking the kids off to piano lessons and he’s not taking kids off to football games, so that when we’re free at the same times we’re always together. I would rather do things with him than with anyone else I know ...” (p. 100).
For these women the major regret was a feeling of missing something in life, of being deprived of a special experience and of a “real” family. As the authors pointed out, such concerns may stem in part from an unrealistically rosy picture of how wonderful things are in a “real” family. Just as unmarried women may idealize the bliss of married life, so childless women may harbor romantic visions of a family life that includes children (Baruch el al., 1985).
Conservative Adaptations
Between the old stasis of the Kinde, Kiiche, and Kirche assignment and the dynamic visions of women’s liberation, open marriage, and complete sexual equality are more typical models, with elements of both, which account for the way millions of American women live today. The emergence of women into roles of economic productivity outside the home has forced adaptations of women, men, and the family. These are marked by the residuals of old human problems and a generation of new ones. In some ways they are very traditional, while in others they are different from anything we have had before. But some of the differences are superficial, are more apparent than real, and represent only a slight shift in women’s positions in the world of men.
Typically, when women work they are grafting onto their lives a new role in addition to the old ones. Since this would seem to add to the complexity of their lives and make great demands on their time and energy, the reasons why they do so must be rather compelling. Also, for the individual woman, her absence from home and her status as economic contributor both would seem to effect a substantial change in the way housework and child care get done, and in her relationship with her husband. At a deeper level of analysis, one would expect her power to increase to the extent that she attains economic equality with men in general and with her mate in particular. However, the research on motivation for working, how it effects other roles, and the relationship between economic productivity and power suggest that, while we may be on the right road, we still have a long way to go.
Why women work
In 1985, more than half of all adult women were working, and six out of ten of these were married.[45] Since the employment of a married woman outside the home must have some effect upon her domestic roles and upon her marital relationship, it is relevant to consider why so many contemporary women are taking outside jobsi Some reasons are money, aspects of the housewife-mother role, and personality factors (Hoffman, 1974).
Mundane as it may seem, the major reason that a woman works is to meet economic need. If she is the head of a household, or if her husband is unemployed or has a very low income, she may work because she must, simply to provide necessities for the family. Or she may work to reach and to maintain a higher standard of living for her family by supplementing her husband’s paycheck with her own. More subtly, a paycheck is tangible evidence of the value of one’s skills. It is connected in our society with such attributes as. achievement, personal worth, and self-esteem. For many women returning to the labor market after years of domesticity, discovery that someone is willing to pay for the work of their hands and brain is a powerful stimulant to growth of their self-image. For the housewife, bringing home a paycheck could be interpreted as a sign of competence and as a tangible contribution to the family (Riesman, 1953).
Certain attributes of the domestic roles of women act as motivators for working away from home. Basic housework is not very creative, and while it can be done at varying levels of competence, it does not require a high level of skill. While it can be embellished by casting it at a level which includes baking one’s own bread, designing and making clothing, and decorating the home with needlepoint and other domestic art, the incentive for such activity has been reduced by the ready availability of such items in the market. A woman may feel that she would rather spend her time at a job earning money to pay for such goods and services than to supply them herself. The role of mother, important as it is, has elements which send some women in search of a job. The constant companionship of children, the relentless demands, the isolation, the loss of freedom, the physical labor, the repetitive tasks, the noise level—these can cause feelings of despair and frustration in the most dedicated mother. It is not uncommon to hear working mothers of young children rationalize their need to get away by saying, “I’m a better mother when I have time away from the children. I have more patience with them and enjoy them more when I’m home.” Another factor associated with the role is its diminishing importance as children go to school and grow up. The woman may go to work not to get away from the children but because their leaving creates a gap in her life which she feels pressure to fill with something meaningful.
The role of personality factors as motivators toward working is much less clear, inasmuch as the numbers of women who work are so large, and as a group they are so heterogeneous, that one would not expect to find them sharply differentiated by personality from their nonworking sisters. Many women are attracted to work outside the home because of a commitment to a skilled or professional occupation and a need to achieve in it, aside from its economic rewards or its offer of an alternative to staying home all day. A career, for example, is often distinguished from a job by the implication that the woman has a long-term identification with a held of work requiring high-level skills, the performance of which results in feelings of achievement and other personal satisfaction. Several studies have found that working women have a stronger feeling of competence and a less traditional view of sex roles, but it is not clear whether this is a cause or an effect of their working status. Studies of the psychological needs that women cite as reasons for working include status aspirations, the realization of potential, desire to benefit society, high energy level, active orientation toward life, and the need for social contact (Hoffman, 1974). A study of women who were seniors in college found that those who wanted to realize their potential through combining a career with marriage were higher in ego strength than were the more traditionally oriented (Gump, 1972). Again, we do not know whether ego strength mediates the willingness to pursue difficult goals, or whether the decision to do the less usual, to pursue two valued goals, increases ego strength. In any case, ego strength was negatively related to the adoption of the traditional female role.
In addition to money, the housewife-mother role, and personality factors, there is another element: social pressure. In recent years a variety of factors have combined to lift the cultural interdiction against employment for married women whose husbands could support them. One of these is the ideology of feminism, which deplores the economic dependence of women and supports the emergence of the individual woman as a strong, independent, free person who will develop herself to the fullest. Her economic independence from the male through her own achievements will give her choices that her mother never had. The appeal of this line of thinking is strongest to the young and educated, and while it may be considerably attenuated among more conservative groups, one suspects that the college woman who openly states that her only life goal is to be a housewife and mother will be regarded as quaintly archaic or hopelessly reactionary. In fact, a study by the Educational 1’esting Service of college freshmen women found that the percentage who thought that “women’s activities are best confined to the home and family” dropped from 37 in 1970 to 9 in 1973. Asked to make future goal predictions, fewer than one in five of the latter looked forward to being a housewife fifteen years later (Wilson, 1974). Parents of daughters, too, knowing that the rate of marriage failure is high and alimony less certain, are more interested in the education of daughters for future contingencies. The notion that the education of sons is more important is less prevalent today, with almost equal numbers of males and females continuing into higher education.
Whatever the motivation, women are working. The new cultural imperative seems to be that most women will combine marriage with a job or a career. One study found this expectation emerging as a function of age from puberty to young adulthood. A study of junior high, high school, and college women revealed that the youngest group saw marriage as their most important future goal. For the older groups career emerged as an important part of their life pattern, accompanied by increasingly liberal attitudes and desires regarding work for women (Rand and Miller, 1972).
Women’s careers: “Dream vs. Drift”
Men’s constructions of their adult lives are often guided by “the Dream,” a kind of anticipatory vision of what a man will do with his life. Defining the Dream and finding ways to live it comprise an important developmental task, necessary to making the transition to adulthood and serving as a guide or ground plan to how one will live one’s life (Levinson, 1978). Women have traditionally expected that much of their life satisfaction will come through someone else’s Dream, a vicarious sharing of the realization of the Dream of the other. Pamela Daniels (1981), in research on the timing of parenthood, found that many gifted women, not having an early Dream of their own, more or less drifted into their eventual successes and accomplishments. Songwriter Joni Mitchell, for example, asked about her preparation for her success, said: “I never thought that far ahead.... I always wanted to play music and dabbled with it, but I never thought of putting them all together. It never occurred to me” (qtd. in Daniels, 1981, p. 289). Other talented women, who did have an early Dream, found themselves dismissing it, deferring it, or pursuing it and finally claiming it with considerable hardship, owing to the conflicting demands of marriage and motherhood. The phenomenon of drift, however, seems to reflect old taboos against women having Dreams of their own, separate from their connections with others. It is difficult for a young woman, with few role models and mentors, to think in terms of a Dream that encompasses a lifelong commitment to work other than that which is supportive of others. Often her game plan for her life is so contingent upon the answers to the questions “Whom will I marry” and “Who will I be then?” that the making of a Dream seems premature, if not presumptuous. Thus women for whom this is an issue find their lives colored by compromise, accommodations, and postponement, often, of the Dream. But, as Daniels (1981) points out, a good Dream can help one negotiate the role conflicts that come up all the time, can see one through the frustrations and interruptions, so that even a period of drift may be used in creative ways.
Role adaptations
The traditional family has always exemplified in its structure and function the concept of the division of labor: the man is the provider; the woman manages the household and cares for the children. This division of labor is no longer clearly defined, as a majority of women are now in the work force. But while this change seems firmly established, it appears that only one side of the division has given way, resulting in a marked asymmetry in the work roles and work loads of men and women in industrialized countries (Newland, 1980). One reason for this is the difference in pay and prestige attached to men’s work compared to women’s work at home, leading women to seek access to the work force and to public life. There is no corresponding demand by men, however, for equal participation in housework and child care. Another reason is that governments can open up work opportunities to women by requiring equal opportunity and nondiscrimination, but governments have no jurisdiction over who does the housework (Newland, 1980).
A result of this imbalance is that married employed women carry a disproportionate share of the couple’s total work load. A United Nations’ review of progress for women based on data from eighty-six countries concluded that in all cases the amount of leisure time of employed women was less than that of employed men. Though employed women spend less time at housework than do nonemployed women, the total number of hours they spend working is greater than the total of either men or nonemployed women, by as much as ten to fifteen hours per week (Newland, 1980).
These are generalizations. What actually happens in families when women go to work outside the home? Are role prescriptions modified? Do they ever vanish altogether and if so, under what conditions? When mother brings home a paycheck, does father pitch in with the housework? The research in this area yields two major conclusions: first, the employed married woman does less housework than she did when she was not working, and her husband does more; and second, the home and children continue to be viewed by both as primarily her responsibility.
Some variations were introduced into these basic conclusions by the variables of ages of children and wife’s commitment to work. Husbands did more housework when children were small, presumably because there was more to do. Though older children might be expected to take on some of the chores, prevailing child-rearing beliefs promoted to some extent an indulgent attitude toward offspring, at least as they were interpreted by many parents who reported concern that children not be overburdened with household tasks (Roy, 1963). Wives whose work commitment was low, who were working primarily out of economic need, received more help from husbands and children than did wives with high commitment, who would work whether they needed the money or not. Regarding this last finding, there are probably both economic and psychological factors at work. One is more likely to find commitment to work among educated professional women who can afford household help, thus reducing the need for the husband’s contribution. And, poignantly, the woman who works to satisfy her personal needs may feel sufficiently guilty that she cannot burden her family with tasks which she would be doing if she had stayed at home.
Though some husbands pitch in with the dishes and laundry, housework and child care continue to be seen as the woman’s responsibility. This prediction for sex roles of the future was made more than three decades ago.
Even if, and it seems possible, it should come about that the average married woman had some kind of job, it seems most unlikely that this relative balance would be upset; that either roles would be reversed, or through qualitative differentiation in these respects, completely erased (Parson and Bales, 1955, p. 15).
Considerable research attention has focused on the dual-career couple, families in which both the husband and the wife are engaged in full-time professional work for which they have a long-term commitment, over and above economic necessity. An early study of such couples concentrated on a sample of highly educated professional women, a group expected to be among the most liberated of women, and to have a most nearly egalitarian marriage. The data permitted the fifty-three couples to be described in terms of four types of marriages: traditional, neotraditional, egalitarian, and matriarchal.
In the traditional families, the wife’s career was regarded by both her and her husband as equivalent to a hobby, with the family’s status and income deriving from the husband. The wife’s income was not used for family needs. Her principal role was wife-mother-homemaker. Though hired domestic help performed most of the routine chores, she alone was responsible for all other feminine role tasks, such as child care, entertaining, cooking, and so on.
The neotraditional families differed from the traditional in that the wife’s income was needed to maintain the standard of living, and her career was given some importance when major family decisions had to be made, such as moving to another city. Though more egalitarian in the division of labor (the husband “helped out”), both considered the wife to be in charge of the home and children. When a woman pediatrician, married to a pathologist, was asked if her husband helped around the house, she said:
He helps a lot. I don’t ask him to clean up the livingroom or to wash the diapers—I have a maid to clean. It’s the little things that are most important. If I am tired, he will take the baby ... and he is not at all demanding. If I am busy, he doesn’t mind having a TV dinner for supper (Poloma and Garland, 1971, p. 750).
Let the speaker be male, and substitute “she” for “he”. The resulting incongruity will clearly demonstrate whose responsibility the baby and the dinner are.
Only one couple was truly egalitarian in sharing both the provider and child-care-housework roles. The other five families were classified as matriarchal because the wives earned more than their husbands. Even so, the men did not share significantly in the work and responsibility of the household.
During the past decade, the incidence of dual-career families has increased greatly, not only because of the unprecedented entry of women into the work force but also because of the rising percentage of women among the professions and other prestigious careers. In these families, wives are more nearly equal with their husbands in education level, job prestige, and income than are working wives in general.
In-depth interviews of ten couples, in which both partners had continuous career involvement with minimal interruption of the wife’s career to have children, revealed that all the couples experienced work overload problems because neither was at home to perform the usual domestic duties and to take care of the children. The most common solution was to hire domestic help, which relieved the housework overload but was not as helpful in easing the parents’ concerns about child care. Responsibility for common household chores tended to be variously distributed: preparation of meals, food shopping, hiring of help, and care of children—including emergencies and school holidays—were generally taken care of by the wives; husbands took care of the cars and shared in disciplining the children, maintenance chores, financial management, and making special household purchases. Domestic help did other routine tasks. These couples tended to have little leisure time or social life. Even so, the wives felt that they had gained in self-esteem and had experienced important intellectual and psychological benefits from their work. Children, too, were reported to be independent, resourceful, and self-confident, showing none of the “maternal” deprivation predicted by traditional ideology (St.John-Parsons, 1978).
Frequently professional women interrupt their careers to have and care for children before returning to their work. One study looked at the differences in family involvement of couples in which both had worked continuously, and couples in which the husband had worked continuously and the wife part-time. Couples with similar employment histories shared the family work more evenly in the areas of maintaining relations with the community—friends, relatives, colleagues, and so forth—and such household chores as cooking, cleaning, and shopping. In the area of child care, however, all wives did more than their husbands. The author suggests that women have absorbed the message that working mothers are bad mothers; thus, their guilt feelings about leaving their children cause them to compensate by taking on child-care tasks when they are home. Since men have no such conditioning, they would be less motivated to share equally the nurturing role in the family (Weingarten, 1978).
Psychologist couples themselves came under scrutiny in one study on the effects of family size on domestic and job satisfaction and productivity (Bryson et al., 1978). Predictably, the larger the family, the more problems the couples expressed concerning allocation of time—for family, for profession, for home, and for avocations. As for satisfaction with advancement in their careers, a curious sex difference emerged: as family size increased, husbands expressed more satisfaction, wives less. As domestic demands increased with more children, they were unequally distributed with more of the burden falling on the wife. “... it is surprising to find that even in couples where both husband and wife are professionally trained (and presumably in a field where they would be relatively more accepting of the concept of sexual equality) the evidence suggests that traditional sex roles still appear to be the basis for allocating responsibility for child care” (Bryson et al., 1978, p. 76).
Contemporary feminist scholars have placed strong emphasis on their theoretical view of family inequality, specifically the division of family labor resulting in role overload for employed women. A recent analysis of two very large national surveys revealed some interesting trends in husbands’ and wives’ relative participation in household tasks and child care (Pieck, 1985).
There appears to be a long-term trend toward increased male participation in family work, both for younger men and for older men with employed wives. Between 1965 and 1981 the time spent in family work of both younger (aged twenty-five to forty-four) and older (aged forty-five to sixty-four) men increased by 2.3 hours per week. This increase was accompanied by a decrease in women’s family time by 14.1 hours per week for younger women and 7.6 hours per week for older women. These shifts mean that men’s contribution to total family work load has increased from 20 percent in 1965 to 30 percent in 1981. Thus men and women seem to be moving toward convergence in their family time, though there is still a twentypoint gap between where we are now and equality. Interestingly, the increase in men’s family time is occurring at a time when broad social trends are decreasing adults’ time spent in housework and child care. Fewer children, thus less housework, have served to decrease women’s time in home-related work, while men’s increased involvement goes against this trend. It is suggested that our society is undergoing a value shift toward greater family involvement by husbands. This is no doubt related to value changes that support wives’ (and mothers’) employment, as well as to changes in the perception of fatherhood and fathers’ participation in child care (Pieck, 1985).
Finally, however, we are left with the fact that employed women still carry a disproportionate share of the total work involved in family maintenance. What are the factors that hold men back from doing their full share? In Pieck’s (1985) analysis four major social processes are seen as accountable for men’s low family participation:
-
Motivation: wanting to participate is effected by such variables as husband’s experience in his family of origin, attitudes of wife and peers, media images, and so on.
-
Supports: it helps if significant others give positive reinforcement for his participation, along with advice and help, such that the family role becomes self-reinforcing.
-
Skills: some men would be more highly motivated to do family work if they knew how. Learning the specific skills makes family participation more rewarding and gives a man more self-confidence in the role.
-
Absence of structural barriers: some men are constrained by institutional barriers, such as inflexible or very demanding job schedules. Also significant is the fact that the greatest time and effort are demanded in the early stages of career development, just when family requirements are also at their peak. Too, husbands usually earn more than wives do, and if they both put in equal time at work and at home, the net effect may be a reduction in family income. Thus the husband-wife wage ratio can act as a powerful structural disincentive to husbands’ participation at home (Pieck, 1985).
Several years ago, anthropologist Margaret Mead delivered an address on gender roles in various societies. At the end, a member of the audience asked if she thought women would ever achieve equality with men. The response was immediate. “It depends,” she said, “on who takes care of the children.” If that is the case, these studies show that equality, even for highly trained professional women, is still an elusive goal.
The power shift
The totality of human interaction can never be understood without including the pervasive role of power Qacobson, 1972). Marriage, being the most common and intimate of all human interactions, is a relationship in which roles are invested with greater or lesser power, one determinant of which is economic. While the concept of power is variously defined, or not defined, in the research it generally is held to mean the ability of one person (in the case of a marriage) to influence or control the behavior of the other, or to make more of the important decisions. In marriage, such decisions include, for example, what job the spouse should take, where the family will spend vacation, what kind of car they will buy, whether the children go to public or private school, and what kind of food is eaten.
Considering the distribution of power in the family, two facts emerge as salient. First, in most families, the male is the primary provider of economic resources, and second, most important family decisions involve money. Thus it follows that in most families the male exercises more power than the female does. Although the matter of who supports the family is not the only determinant of power, most of the research supports the conclusion of male dominance, in spite of popular belief to the contrary (Gillespie, 1975).
What happens to this unbalanced situation when the wife is employed? In some cases, she gains power in areas where she had none and loses in areas where she was dominant. In other cases, nothing is different. For example, if her income is critical to the family’s well-being or desired standard of living, she gains power in the making of decisions about how money will be spent. On the other hand, if her husband or someone else participates actively in the care of the children, she may lose power in the decisions regarding them. And in the cases of the upper-class professional women where their income was not needed, the fact of their working made very little difference in the power structure of the marriage (Poloma, 1971). This so-called modern family type was not basically different from the traditional model.
An interesting class difference has been observed in the power wielded by working wives. Lower-class wives gain more power when they are employed than middle-class wives do (Bahr, 1974), in spite of the fact that middle-class husbands espouse a more egalitarian philosophy than do their lower-class counterparts (Gillespie, 1975). While the first finding is readily explainable by the assumption that the wife’s income is more important to less affluent people, the contrast between deed and word across classes is something of an anomaly. It may be that the lower-class male is ideologically more concerned about presenting a traditionally masculine image but is more willing to concede material power when it is realistic to do so, whereas the educated male adopts the more sophisticated strategy of verbally supporting an egalitarian arrangement while tacitly expecting the traditional perquisites of his sex.
We have seen how social changes are effecting shifts in women’s lives from the precedents set by tradition to adaptations that often permit greater freedom and flexibility. The most important change for women is their movement out of the home and into the work place and a more public life. More than broadening their lives and helping them to take better care of themselves, this change adds choices to women’s lives where once there were none, except in unusual instances. It is not that women in great numbers are switching from a life of domesticity to a life of employment and economic independence, but rather that women now can choose among many possible ways of living their lives, taking what they want from the old and the new to meet their individual needs and desires.
Black Women: The Minority Experience
As the psychology of women emerged as a discipline in the 1970s, most of the issues it raised and its published content were based on observations of white, mostly middle-class women and the sociocultural context of their behavior. The psychology of women developed as part of women’s studies, the academic arm of the women’s movement, whose constituency was mostly white, middle-class women. Except for scattered references, studies of the lives and experiences of black women hardly appeared in writings on the psychology of women.[46]
But the importance of attention to black women identified as such is that one cannot assume that the experiences, interests, and concerns of black and white women have much in common with each other. The editor of an anthology of black women’s writing asked, “How relevant are the truths, the experiences, the findings of White women to Black women? I don’t know that our priorities are the same, that our concerns and methods are the same” (Cade, 1970, p. 9).
While both black women and white women have suffered from discrimination and oppression, the status of black women has been lower than that of white women in the society because of racism. Being black and female has subjected black women to both racial and sexual inequality. Shirley Chisholm, the first black woman ever to be elected to the House of Representatives, was speaking of herself as a black woman when she said, “It is a disadvantage because America as a nation is both racist and anti-feminist. Racism and antifeminism are two of the prime traditions of this country.” To challenge these traditions, she said, is to invite punitive sanctions, whose sole purpose is to protect the sanctity of the traditions (in Lerner, 1973 p. 353).
Black women have tended to see racism as a more potent cause of their subordination than sexism. Thus, when the women’s movement arose in the 1960s, the same decade in which the civil rights movement began, black women viewed it with some mistrust, feeling that it was exclusively concerned with sexism and that they needed to spend their energies on the common cause that they had with black men, the cause of fighting for social, political, and economic equality with whites. They saw that white women at least were accorded deference in their roles of helpmate, mother, and sex object, and that many if not most white women at the time were economically supported by men. Black women were denied these roles. Deference was not accorded to them because of the stigma of race. Too, their important economic role as providers for their families, even in menial and low-paying jobs, gave them a degree of power in their society, power that was often resented by black men, who were unable to get work (Lewis, 1983). Alice Walker, Pulitzer Prize—winning black author, noted this hostility when she wrote, “Black women are called matriarchs, called castrators of the men, and all kinds of things by black men ... [when] [t]hey thought they were just providing for their families, that they were just surviving” (Walker, 1972, pp. 601–2).
Despite the perceived greater evil of racism, black women have organized to combat sexism as well. The National Black Feminist Organization, at its first meeting in December 1973, stressed that such feminist concerns as day care, abortion, and maternity leave were of even greater significance to black women than to white women because of their greater economic disadvantage. It has been proposed, however, that even if increasing numbers of black women become involved in opposition to sexism and racism, their organizations might be limited to blacks and strongly racially oriented. “The concern with racism would preclude too exclusive a concern with sexism” (Lewis, 1983, p. 191).
Thus the psychology of black women is set in a context of historic and institutionalized racial oppression. As with any minority group, black women have suffered from being identified as an outgroup, as the Other, and from the fact of their difference being used to deny full participation as free citizens in the society. Joyce Ladner (1972) wrote of the psychological cost of such oppression: “Every Black person can probably recall the time when he first became painfully aware of the lifelong restrictions that would be placed on him because of his color” (p. 80). One would expect such treatment to result in low self-esteem and feelings of self-hatred. Yet this has not been confirmed in the literature. Ladner’s study of black urban girls found that the great majority of them were proud of their race and would not change it. There was no evidence of low self-esteem, nor did they experience feelings of inadequacy because of their race. None desired to be white. As one fifteen-year-old put it: “I feel that I’m just as good as the next person. I feel that a white person or someone of any other race, if they’re as good as I am, well, I feel that I’m even better.... I don’t think there should be any setback just because I’m a Negro”(p. 88).
Once again it is important to note the commonalities between the experiences of being black and being female. Although women outnumber men in the society, both women and blacks have minority group status. Both have experienced discrimination in educational and occupational opportunities. Both have been relegated to “special” roles in the domestic and service sectors that white men did not want, roles that thus were stigmatized because of their association with women and blacks. Both have been labeled as being childlike and immature, between child and adult male. Both have been stereotyped as devious and unreliable, irrational and irresponsible. Both have been held to be mentally inferior to white males. And both, curiously enough, have been believed to be happy in their roles, the contented housewife and the singing fieldhand. Politically, the commonality continues. It was through involvement in the nineteenth-century antislavery movement that white women became aware of their own oppression and launched the first feminist movement, whose aim was to raise the consciousness of women to the fact of their political powerlessness and to win for women the right to vote (accorded to black males in 1870). Again in the 1960s the black civil rights movement gave impetus to women to look at their continuing exclusion from the opportunities and rights that men took for granted and to begin to demand their fair share. So the status of both women and blacks, and especially of black women, has risen from roots of oppression. And perhaps that is the basic reason that a psychology of women had to come into being.
In this section, we shall look at research on black women and their families, their socialization, their education, and their orientation to achievement. Comparisons to and relations with black men will be discussed in each of these contexts.
The family
There is no single type of family pattern that is typical among blacks any more than there is among whites. Rather, diversity is the rule. In this section we look at some data on family organization and household patterns and examine some myths about black families in American society.
Potentially, the event of marriage signals the birth of a new family. For the past twenty years, Americans have been postponing the age of first marriage, with blacks marrying later than whites. For example, among black females in the twenty to twenty-four-year-old age group the percentage never married went from 36 percent in 1960 to 69 percent in 1980. In the same two decades, the percentage of black women over the age of fourteen who were married declined from 60 percent to 49 percent. These changes reflect the increased numbers of blacks continuing their educations, economic hardships attendant upon the recessions of the 1970s, and lifestyle changes, including living together without marriage, that characterized Americans in general (Blackwell, 1985).
Household patterns of black families are more heterogeneous than they are for American society as a whole. They may consist of the basic husband-wife unit, the nuclear family of parents and their children, or the attenuated nuclear family, in which one of the spouses is absent. These primary types may be elaborated into extended families that include relatives, or two or more families living together, or unrelated persons joining a family unit. According to the 1980 Census data, over half (55.5 percent) of all black families consisted of a married couple, with or without children or others living in the house. Forty percent of black families were headed by women, and the rest by men, most of whom did not have their children living with them.
Black children are only about half as likely to live with both parents as white children are. Over half of all black children live with their mothers only, or with their grandmothers or other female relatives. Two-parent families tend to have higher incomes than single-parent families, most of whom are headed by women. The high incidence of female-headed families among blacks is a major factor in the number of black children living at or below the poverty level. For example, the U.S. Bureau of the Census (1980) reported that only 11 percent of children living with both parents were in poverty, compared to one-half of children living in homes with the father absent.
Black families have stereotypically been described as matriarchal, that is, with power and decision-making authority vested in a strong woman head. This belief, to be discussed in more detail later, has been challenged by research that indicated that the most common authority pattern is actually egalitarian in two-parent homes. In such homes, too, roles are more flexible than in traditional families, with men more likely to do housework and women more likely to take on the provider role. Such adaptations have been necessary to enable families to survive the kinds of crises that are more likely to threaten poor families with few resources (Blackwell, 1985). Supportive of this less hierarchical pattern is a study comparing whites’ and blacks’ ideas of the “Ideal Woman.” Blacks saw the ideal woman as more assertive, achieving, and independent than whites did, and black males and females were closer in their perceptions than white males and females were (Crovitz and Steinmann, 1980).
Controversial issues of illegitimacy, divorce, and the “black matriarchy” stereotype, all related to perceptions of the stability of the black family, attract the contemporary attention of both researchers and government policy planners. Though it is possible to discuss these only briefly, each is important to the experience of growing up black and female in America.
Although the illegitimacy rate, defined as the number of illegitimate births per one thousand unmarried women, is much higher for blacks than it is for whites, the rate for black women has been declining over the past two decades, while the rate for white women has risen. Even so, in 1982 more than half of all births to black women in the United States were to unmarried women (Blackwell, 1985). Research has indicated that pregnancy rates for unmarried women are highest among young women from poor and disrupted families. For example, high levels of permarital pregnancy among black teenagers in Chicago were associated with poverty, ghetto residency, female-headed households, and large family size (Hogan et al., 1985). Black women are less likely than white women to terminate illegitimate pregnancies by abortion and are more likely to keep out-of-wedlock babies and to incorporate them into the family. Black families may be less moved to condemn and reject the unwed mother and her child and less concerned about the status of the child as legitimate or illegitimate (Blackwell, 1985). Even so, teenage mothers are a particularly vulnerable group, at risk for social and economic reasons as well as for health-related concerns.
According to data from the U.S. Census of 1980, the divorce rate among blacks is more than twice as high as it is for the general population. This rate has risen sharply over the past two decades, as it has for Americans in general owing to changes in atntudes toward marriage and divorce and the greater ease in recent years with which divorces are granted. The particular economic and social stresses experienced by blacks further exacerbate the situation, as poverty, unemployment, and other aspects of the disadvantaged status of many black people contribute to disruption of family ties.
The large number of female-headed black households, first brought to national attention with the publication of The Negro Family: The Case for National Action by Daniel Moynihan (1965), gave rise to the notion of a black “matriarchy,” a society in which family power is lodged in women rather than in men (or shared by both). It was Moynihan’s thesis that family structures that were headed by women contributed to the poverty, illegitimacy, and delinquency that existed in many black communities. In particular, such power vested in women in the family had the effect of robbing the black male of his manhood, of stripping him of authority, of turning him into a shadow figure in the family, or of literally driving him away. This myth of black matriarchy has been challenged by several scholars of the black family (Ladner, 1972; Powell, 1979; Staples, 1970). It has been held to be injurious to black women and black men alike. According to the myth, the black woman is almost superhuman, brave, strong, capable of taking care of all the needs of her family without the help and support of a man. This facile view ignores the bitter necessity for many black women of struggling alone to care for their children, with no other option available to them. It also carries the assumption that the inability of many black males to function effectively in the society is because of their psychological impotence at the hands of black women, rather than because of historic social events and conditions (Ladner, 1972). The myth was able to gain credence because of the large number of woman-headed families in black communities, such that women in decision-making roles in families were more evident than they were in other American families. In a woman-headed household, it is obviously a woman who will have the power. The myth ignores the facts that a majority of black families have both parents present and that in these families authority is most likely to be shared:
... in many Black homes where the husband and wife are present, women appear to be carrying the major responsibility for the family unit and the man seems to be a shadow in the background. However, his shadow does not mean that he is non-assertive. Oftentimes he makes decisions in the household that are entrusted to his wife for implementation. In still other families, the wife does indeed make most of the decisions but with the tacit, sometimes explicit, and always understood permission of the man. His is the ultimate authority and he can exercise it when he wishes or feels impelled to do so (Ladner, 1972).
Socioeconomic factors play a major role in the integration of the male in black families and in black family stability in general. Studies of black and other American families show that socioeconomic level is an important correlate of male status in the family, particularly in the middle class. Stable employment gives men authority and respect in the family, and middle-class black males enjoy a status in their families that is comparable to that of other men in the society (Powell, 1979).
While black women have indeed shown strength and resilience, it has not been at the expense of men. “The strength and the coping capacities evident in the biographies of Afro-American women, who in spite of the racism, sexism, poverty, and undeserved culpability managed to overcome such adversities, have been unfairly maligned” (Powell, 1979).
Finally, attention has been called to some unique strengths of black families. These include (1) strong kinship bonds, such that relatives, children, elders, and subfamilies may be incorporated into the family structure; (2) the strong likelihood for black children born to unwed mothers to be kept in the family rather than given up for adoption and the absence of stigma attached to such children; (3) a strong work orientation among black people; and (4) high flexibility of black families in roles in the home and the greater probability of an egalitarian authority structure (Hill, 1981).
Socialization
Poet and novelist Alice Walker (1983) wrote of an Easter Sunday morning when she was about six years old, all dressed up for a church service at which she was to recite a speech. “When I rise to give my speech 1 do so on a great wave of love and pride and expectation. People in the church stop rustling their new crinolines. They seem to hold their breath. I can tell they admire my dress, but it is my spirit, bordering on sassiness (womanishness), they secretly applaud.
“That girl’s a little mess,’ they whisper to each other, pleased” (p. 385).
Born in Georgia, the youngest of eight children, Walker grew up in a rural farm family. Her mother labored beside her father in the fields. Her mother also made all the family’s clothes, canned vegetables in the summer, and made quilts in the winter, with never any time to herself. Walker went to school, and when she graduated from high school at the top of her class, her classmates took up a collection and gave her seventy-five dollars to start her college education.
Growing up female does not have the same meaning for all black girls any more than for girls in general. One can only generalize and describe a few examples, especially since research on black girls and women is not plentiful, and behavioral scientists have learned that, given the pluralistic nature of our society, generalizations that may be valid for people socialized in the mainstream cultural traditions may not be valid for others whose experiences and traditions are different. A noteworthy contribution to understanding of the socialization of black girls is Joyce Ladner’s Tomorrow’s Tomorrow. The Black Woman (1972), a study of low-income black girls living in an urban housing project. In this community, the major agents of socialization for girls were their immediate and extended families and their peer groups. The girls spent much time with grandmothers, aunts, and other relatives, who often cared for them while their parents were at work. Some were “given” to grandparents who brought them up as their own. Many lived normally in a three-generation household.
Between the ages of five and twelve, peers became important, often more important than the family in influencing values and behavior. Although the girls in this age range were involved in play, school, and other activities not unique to them, they also were engaged in sharpening their roles as women. Ladner perceived that while other girls might be playing with dolls and engaging in other rituals of childhood, many of the girls in the project did not have the luxury of a conventional childhood. Parents were not able to provide them with the material setting for the middle-class child’s experience of her early years, and they often could not protect them from the harshness of their environment, with its poverty and potential for violence. Most of the children in the study could relate directly to some form of violence, and one had been raped at the age of eight. This “absence of childhood,” Ladner found, was present in many young girls in the project. At the same time, she found that they developed a great amount of strength and adaptability that enabled them to cope with their world.
What aspirations did these girls have for the future? Though there was no single route to becoming a women, several trends emerged. They tended to identify with role models they knew well, as mothers or older sisters. Sometimes they looked to others whom they identified as successful, such as singers or actresses. They saw themselves as relating to men, though with ambivalence. Many had boyfriends, and they talked of marrying a wealthy man who would take care of them. At the same time, the women they knew best were very hardworking, and many had no man to help them financially. They saw the necessity of being strong. Some wanted to further their education as a way of entering the middle-class world of material prosperity.
These girls are influenced by a set of traditions, a common value system and a set of beliefs that, although varying from group to group, are still shared to some extent by all of them. Their aspirations for being the hard-working backbone of the family, for children, for an education and for a kind of spiritual quality of empathy—the ability to understand and develop the necessary resources to fight oppression and make healthy adaptations to what are sometimes overwhelming circumstances—are common features (Ladner, 1972, p. 175).
Psychological studies of gender-role development and self-concept of black girls and women are not plentiful. As noted above, gender roles among black people are more egalitarian, carrying the expectations that both males and females will be economically productive and that both will participate in household chores. One would think that such socialization would lead to less traditional attitudes among black women. The research reveals, however, that while black college women anticipate careers and lifelong employment, their attitudes toward women’s role in the tasks of home and child care are quite traditional. In fact, their plans for future work and family roles are not different from those of white college women (Smith, 1982). One study pointed out that the expectations for work, while the same for black and white women, might come from different motivations. The young black women described their work commitment as motivated from a sense of responsibility for family support. Young white women were more likely to credit their work intentions to a need for self-fullfilment (Gump and Rivers, 1975).
Interesting Endings on the self-concept of black girls and women have begun to appear. While historic factors of minority group status and discrimination might have affected black self-concept in the past, such does not seem to be the case for black females of today. A national study on the self-image of girls aged nine to seventeen found that black girls rated themselves higher than white girls did on all the following dimensions: being quick to learn, being good in sports, being well-dressed, being good-looking, having the teacher like you, and having many friends (Prendergast, el al., 1974). Black female adolescents in another study likewise reported positive feelings about themselves. Their feelings were affected somewhat by whether they were in black or white situations. They felt they were “being-me” more often in the black community and “not-being-me” more often in white situations. Interestingly, however, “not-being-me” did not involve a devaluation of the self; rather, their dislike was of the situation (Sterling, 1975).
Education
The earlier literature on the educational careers of black girls and women suggested what one writer called “the farmer’s daughter effect”: “Similar to farm parents, the Negro parents seem to have made the assumption that daughters will be more successful than sons in attending school, acquiring occupational training, obtaining a job equal to their education, and generally improving themselves” (Bock, 1969, p. 19). Indeed, studies of black communities prior to school desegregation found that black females had higher literacy rates and more years of schooling than black males had. Their aspirations were higher and were linked to jobs available to blacks at the time. Black men, for example, might aspire to own a farm or to work at a skilled trade, whereas black females could use a college degree to teach in the segregated black schools. For black men, higher education did not open up job opportunities. Thus black women were more likely to graduate from high school and college than black men were (Lewis, 1983).
In the years since desegregation, the research reveals that some changes have occurred. A review of the literature on the educational achievement of black females indicated that black females continue to have higher scholastic achievement than black males at the high school level. At that level, they also have higher educational aspirations, with more of them voicing expectations of pursuing undergraduate and graduate degrees. The situation changes with regard to college enrollment, however. In 1970, 28.7 percent of black men and 24.1 percent of black women high school graduates were enrolled in college. By 1981 the figures were 28.2 and 27.8 (Blackwell, 1985).
Even in the 1960s, when black women were somewhat more likely than black men to be enrolled in college (6.1 percent and 5.2 percent respectively), black men were more likely to obtain graduate and professional degrees. One study of black institutions found that 91 percent of such degrees in medicine, dentistry, law, veterinary medicine, and theology went to men (Jackson, 1973). Other surveys of black doctorates from all institutions indicate that black women receive about one in five of these degrees (Lewis, 1983). Thus, while black females have higher educational achievement and higher apirations than males at the high school level, the picture changes in college, as it does with white females, with fewer of them continuing their educations past the undergraduate level.
Thus the “double jeopardy” of being black and female puts black women at the bottom of the educational achievement ladder. The lingering effects of racism mean that she is less likely than her white sister to pursue high-level educational goals, while her gender puts her at a disadvantage compared to her black brother.
Achievement
The stereotype of the striving, independent, dominant black woman seems to reflect her behavior more in the domain of home than in the world of work. It is true that black women seem to have less conflict in combining the dual roles of family responsibilities and work, since, as we have seen, black women have traditionally worked outside the home out of economic necessity. Still, research on career aspirations of black college women reflects the constraints of genderrole concerns, with most preparing for such occupations as school teaching, nursing, and social work (Murray and Mednick, 1977). Aspiring to careers, they turn, as many other women do, to traditional women’s work that involves caring for other.
The motive to achieve as usually defined, “competition with a standard of excellence,” may be less important for black women (women in general?) than it is for others. Their career choices may be more reflective of feelings of responsibility than of an intrinsic need to achieve (Gump and Rivers, 1975). This interpretation is supported by the fact that, as noted earlier, a substantial proportion of black women are heads of households and thus might be more interested in achieving economic security in a stable job situation. The sense of responsibility as motivation for career choice is also reflected in the tradition that links professional work to service in the black community. Careers in education and social service fields are seen as serving the needs of black people: “This linkage has involved both individual and collective strategies. Black women’s uplift organizations and national professional organizations have constantly, since the end of the nineteenth century, tried to wed black women’s professional aspirations to black community needs” (Gilkes, 1982).
The continued tracking of black women into traditional female occupations, however, has been partly responsible for their status as lowest paid workers. Black women are more likely than white women to be employed, but they earn less at lower status jobs. They also earn less than black men and are notably absent from those professions that are typically male-dominated. Clearly, if the employment and economic situations of black females are going to improve, more need to look to jobs and careers in fields that are less traditional for women (Burlew, 1982).
Important differences have been found between black women preparing for traditional and nontraditional careers. The backgrounds, attitudes, and career expectations of black female undergraduates pursuing traditional (teaching, social work, and nursing) and nontraditional (sciences, engineering, law, business) careers were investigated at a large urban university. Their backgrounds differed in two respects. First, the mothers of the nontraditionals were better educated and were more likely to have worked in nontraditional Helds themselves than were the mothers of the traditionals. Thus their mothers provided role models for achievement in areas less typical for women. Second, the nontraditionals were more likely to have had early work experience, perhaps giving them an opportunity to experience the rewards that are associated with various jobs. The nontraditional were also more confident in their ability to complete nontraditional educational programs and had less traditional ideas about appropriate roles for women than did the traditionals. They also thought that their chances for marriage would not be impaired owing to their career choices. Poignantly, however, they believed that they would have few female friends because of their choice of “the road less traveled” (Burlew, 1982).
Minority women are greatly underrepresented in the scientific professions. In 1975 the American Association for the Advancement of Science brought together minority women in science, engineering, medicine, and dentistry to discuss their common bonds of race, sex, and career choices. It was noted that programs designed to bring more women into science-oriented careers actually focus on white women, while programs targeting minorities are dominated by males. Therefore, it is of special interest to discern the common features in the backgrounds of those women who managed to overcome the double burden of sexism and racism to enter those professions dominated by white males.
Most of the participants had several early life experiences in common:
-
Most had learned to read at an early age.
-
All described a strong sense of self beginning in childhood.
-
Many remembered the encouragement of a particular teacher or friend.
-
They were rarely ambivalent about school and the value of education.
-
They had always been aware of their sex and ethnic status.
-
All had experienced poverty and racism as children and adolescents.
The women talked also about their academic experiences. They felt that their high school preparation had not been adequate and that role models were few throughout their academic careers. Their science professors had displayed condescending attitudes toward them, with the tacit expectations that female minority students would not do well. They also had felt socially isolated from other females and from men of all groups. In addition, they felt pressures to marry, to choose more traditional careers, and/or to return to their own communities (Powell, 1979).
Women preparing for or engaging in atypical careers have always suffered from feelings of alienation and lack of other women as role models. As one black woman prelaw student wrote, “I’m doing this for me, but also for my little sisters, and for their cousins, and lor all the little girls in the community. When I get down, I just think about them” (personal communication, 1985).
11. Lesbian identity
Since even many lesbians gave credence to the images originally promulgated by men which saw them as sick, confused, violent, and hopeless, love between women lived in disrepute through much of this century....
—Lillian Faderman. Surpassing the love of men, 1981
I came to realize my attractions—social, emotional, professional, intellectual, sexual—were toward women.... I guess I’d known that for a long time, going back to childhood, when I had urges to be with some of the teachers, wanted to know everything about them, their secrets, the way they did things. I had much less curiosity about men. Looking back to when I was sixteen or seventeen, I can see I had some crushes on some women players and didn’t know it. I just liked, being with them. By the time I was eighteen 1 knew I always had these feelings.
—Martina Navratilova, Martina, 1985
In an earlier edition of this book lesbians were defined as women whose sexual preference is for other women. Most writers on the subject at that time would probably have agreed with that simple definition. Today, however, as lesbianism has emerged as an issue with social, political, and historical dimensions, defining it only in terms of sexuality is too simplistic and narrow. In fact the very matter of its meaning is a controversial issue in the feminist/lesbian literature.
Who is the lesbian? Is she any women who is sexually attracted to other women? Does the act of having sex with another woman identify her as lesbian? If she has sex with men as well as with women, is she a lesbian? Suppose that her life is asexual, but she is strongly identified with women, lives and works with women, and supports and loves women, independent of men—is she a lesbian? Suppose a woman has intimate relationships with other women over years of her life, then enters into a conventional marriage with a man. or vice versa—is she a lesbian? Is lesbian a political identity for those women who renounce patriarchy and its compulsory heterosexuality in favor oh a woman-centered world with strongly held feminist goals? All these questions are being asked, and since misunderstandings about lesbians and lesbianism are common, it is important to attend to the record of contemporary understanding of who and what they are.
Blanche Cook (1979), in an essay on lesbianism and cultural tradition, offered a definition of lesbian that does not depend on sexuality: “Women who love women, who choose women to nurture and support and to create a living environment in which to work creatively and independently, are lesbians” (p. 738). Even if two women do not have physical contact, she argued, if they choose and love each other, they are lesbians. Saying that the issue would be an absurdity if the pair were male and female, she used the example of a famous American general and his female aide, who were unquestionably in love with each other, though they never “consummated’ their love in the conventional sense. But their love would be defined as heterosexual. Therefore, Cook reasoned, love between women, even though nonphysical, can be defined as lesbian.
Feminist poet and author Adrienne Rich (1980), in her classic “Compulsory Heterosexuality and Lesbian Existence,” preferred the terms lesbian existence and lesbian continuum to lesbianism, because of the latter’s clinical, limiting connotations (this would hearken back to the earlier definition of lesbian in terms of sexuality only and to its association with pathology).
Lesbian existence suggests the historical presence of lesbians, who are identified as women bonded primarily to women, sexually and emotionally independent of men. Thus lesbian existence rejects the society’s compulsory requirement of heterosexuality. It is both an affirmation of women’s right to choose each other over men and an act of resistance to patriarchy, which gives only men the right of access to women.
Rich’s concept of lesbian continuum is meant to include a range “of woman-identified experience; not simply the fact that a woman has had or consciously desired genital sexual experience with another woman.” We can expand it to “embrace many more forms of primary intensity between and among women, including the sharing of a rich inner life, the bonding against male tyranny, the giving and receiving of practical and political support; if we can also hear in it such associations as marriage resistance ... we begin to grasp breadths of female history and psychology which have lain out of reach as a consequence of limited, mostly clinical, definitions of ‘lesbianism’ ” (pp. 648—49). Thus the essential criteria for placing women along the lesbian continuum are women bonding with women and resistance to male domination.
Critical of the meaning given to lesbianism by Cook and Rich, Ann Ferguson (1981) wrote that their problem is that they are not connected with history, that they assume that lesbianism can be defined universally across cultures, classes, and races. Instead, she said, sexual identity must be self-conscious, that is, the person must take on the lesbian identity as a chosen commitment or choice. Further, the self-conscious lesbian identity must have relevance in the culture. That is, during the person’s historical period there must be a community of others who likewise identify themselves as lesbians. Since the cultural category of lesbian did not appear until the twentieth century, it is not correct to identify someone as lesbian before then, though women in earlier times who today would be called (and would call themselves) lesbians would be described as sexually deviant. Taking into account these considerations, Ferguson offered her own definition of the lesbian woman: “a lesbian is a woman who has sexual and erotic-emotional ties primarily with women or who sees herself as centrally involved with a community of self-identified lesbians whose sexual and erotic-emotional ties are primarily with women; and who is herself a self-identified lesbian” (p. 166). This contemporary definition of lesbian includes both bisexual and celibate women as lesbians if they so identify themselves and have their primary emotional identification with a community of lesbians.
It has been argued that Ferguson’s definition of lesbian is too exclusive, even elitist, since it leaves out women who lived before the term lesbian came into use, and it is particular to a selected group of women who live in the subcultures of advanced capitalistic societies (Zita, 1981). This points up the problematic nature of definition. In part, the problem lies in who is doing the defining. There are at least two perspectives on lesbianism. One is the perspective of the “normal” society, which has the authority to define lesbians as deviant. The other is the perspective of the lesbian subculture, which is more positive, as exemplified by those definitions we have looked at here, and which sees the normal perspective as pathological (Addelson, 1981).
Implicit in all the concern for careful definition of lesbianism is the necessity of detaching it from male homosexuality. The inclusion of lesbians as female versions of male homosexuals deprives lesbians of a political identity, thus once again erasing female reality:
To separate those women stigmatized as “homosexual” or “gay” from the complex continuum of female resistance to enslavement, and attach them to a male pattern, is to falsify our history. Part of the history of lesbian existence is, obviously, to be found where lesbians, lacking a coherent female community, have shared a kind of social life and common cause with homosexual men. But this has to be seen against the differences: women’s lack of economic and cultural privilege relative to men; qualitative differences in female and male relationships, for example, the prevalence of anonymous sex and the justification of pederasty among male homosexuals; the pronounced ageism in male homosexual standards of sexual attractiveness, etc. In defining and describing lesbian existence I would hope to move toward a dissociation of lesbian from male homosexual values and allegiances. I perceive the lesbian experience as being, like motherhood, a profoundly female experience, with particular oppressions, meanings, and potentialities we cannot comprehend as long as we simply bracket it with other sexually stigmatized existences (Rich, 1980, pp. 649—50).
How to define lesbian existence? And why does the task capture the attention of historian, poet, and philosopher, who, while they differ in the subtleties of their definitions, never doubt the task’s importance? Ever since the word lesbian began to be used in the early years of this century to describe sexual passion between women, it has had a pejorative meaning associated with deviance and pathology, as did its earlier counterpart, sapphist.[47] Questions drive the need to define: “How to cleanse the word lesbian, how to dislodge its negative and evaluative meaning, how to expand the scope of the term, whom to include, whom to exclude, and why ...” (Zita, 1981, p. 173).
Defining lesbian is in itself a political act. Lesbians have always been an at-risk group, as part of a sexually stigmatized minority; thus trust in accepting other women as lesbians is a major issue: “Lesbian community is a place where lesbians can relax ... where the women you meet share common interests, and experiences, and desires.... It is the place where we feel at home—a radical kinship in the making. Is it any wonder that the definition of lesbian is vital to our survival as lesbians?” (Zita, 1981, p. 175).
Still unsettled, then, is the final, consensual definition of lesbian. Components of a definition seem to include: (1) a woman whose primary bonds, emotional, social, and probably erotic, though not necessarily, are with other women; (2) a women who identifies herself as lesbian, though she may not do this publicly for reasons related to children, job, friends, and so on; (3) a woman who may (or may not) be part of a lesbian subculture, or community, or simply a group of lesbian-identified women. These components are not definitive and include ambiguities. A definition that is wholly satisfying to all concerned may never appear. But the intensity of caring about the issue has created informed discussion that at least provokes more thought about it than ever before.
Lesbianism in History and Culture
The world lesbian comes from Lesbos, the Greek island home of Sappho, a poet of the seventh century B.C. who wrote love lyrics to some of her young female students. Sappho had a kind of academy to which came aristocratic young women to learn the composition of poetry and music and the cultivation of grace through dance. Men were banned from her colony, which was dedicated to the cult of Aphrodite, the Greek goddess of love and beauty. In her time, Sappho gained renown as a poet, even though it was generally known that her love lyrics celebrated the joys and sorrows of women who loved other women. Later, in the Roman and Christian eras, her lesbianism became the focus of comments about her, and her works were largely destroyed. When bits of her work were recovered and translated in the early nineteenth century, scholars recognized her brilliance and her poetic genius. Since they could not reconcile this with the unacceptability of her sexuality, they proceeded to “purify” her by denying that her poems were written to women, saying that they were written to male lovers and were not even erotic. It is only in recent years, as attitudes have changed somewhat toward homosexuality, that the reality of Sappho’s erotic love for women, addressed explicitly in her poems, has been recognized and brought, once again, “out of the closet” (Klaich, 1979).
Compared to male homosexuality, commentary on erotic relations between women is extremely sparse in the religious, legal, and other secular literature of the Western world until the seventeenth century. The Bible, for example, makes only one mention of this aspect of female sexuality, in Paul’s epistle to the Romans, speaking of pagans who denied the one God: “For this cause God gave them up unto vile affections; for even their women did change the natural use into that which is against nature” (Romans 1:26). While this language is obscure, later interpreters have taken it to refer to sexual relations between women. Judith Brown (1986) in her book Immodest Acts, the story of a lesbian nun in renaissance Italy, looks at church and lay attention to lesbianism during medieval and early modern times in Europe. Two observations emerge as especially salient: first, an awareness of the existence of sexual attraction between women, at least at some level of consciousness, and second, a neglect of the subject that must have been motivated by a profound unwillingness to believe that such things could happen, resulting in its rendition as trivial and unimportant compared to phallocentric sexuality.
Awareness of the possibility of female homosexuality is revealed in the writings of St. Thomas Aquinas, the famed thirteenth-century theologian, who included it among his categories of vice against nature. About the same time, efforts were made to curb lesbian sexuality in convents. French nuns were prohibited from sleeping together. Dormitories were lighted all night, and nuns were prohibited from entering each other’s cells. Brown’s story of the actual inquests into and punishment of the behavior of the nun Benedetta in the seventeenth century is a vivid example of both the ignorance of ecclesiastical authorities and their horror of the acts of which she was accused.
Yet compared to the attention given to male homosexuality by both church and state, lesbian sexuality remained in a shadowy and ambiguous realm. Most early civil laws, which made male “buggery” punishable by death, did not mention women.[48] Great medieval writers, such as Dante and Boccaccio, spoke of sexual misdeeds, including male sodomy, but said nothing of similar female behavior. The few authors who did write about women loving women, however, make it clear why such behavior was so generally ignored: it was seen as a frivolous substitute for real sex (i.e., with a man), a kind of warming-up exercise. Brantôme, a sixteenth-century French court commentator, noted that the fashion of women having sexual relations with each other was becoming quite common, but, he said, it was nothing but an appt enticeship: “... because after they are heated up and well on their way with one another, their heat does not diminish unless they bathe in a livelier and more active current.... Because in the end, as I have heard many ladies tell, there is nothing like a man; and what they get from other women is nothing but enticements to go and satisfy themselves with men” (in Brown, 1986, p. 11). It is probable too that the inferior status of women generalized to their sexual behavior. In a phallocentric society, the sexual activities of creatures who did not have penises and did not emit seed-bearing semen were in general not taken very seriously.
For these reasons penalties for lesbian acts were often more lenient than were those for male homosexuality. Early religious penitcntials prescribed much briefer penances for women who had sex with other women than for male homosexuals. Later, after the Protestant Reformation brought greater concern for legislating moral conduct, penalties became more harsh, and the death penalty began to be prescribed for women as well as for men. In the city of Treviso, “If ... a woman commits this vice or sin against nature, she shall be fastened naked to a stake in the Street of Locusts and shall remain there all day and night under a reliable guard, and the following day shall be burned outside the city” (in Brown, 1986, p. 14). Even so, some writers made attempts to fit the punishment to the seriousness of the crime. The ultimate punishment, death, would be reserved for those woman who used an instrument in their relations with another woman, i.e., those who behaved like men. If a woman only made overtures to another woman, or behaved corruptly by “rubbing,” the punishment might be lighter (Brown, 1986).
After the sixteenth century, lesbian lovemaking entered the French and English erotic literature, where it continued to be seen as a prelude to heterosexual lovemaking and as hardly constituting a threat to male dominance in sexuality. In fact, its purpose was the sexual arousal of men, appealing to male fantasies of stepping in and exhibiting their own superior potency.
The exception to the benign treatment of lesbian behavior during this era was the transvestite, the woman who wore male dress and often passed as a man, even marrying another woman, thus completely rejecting the female role. Death by execution was often the punishment for such intrusion into the masculine sphere (Faderman, 1981).
The most notable American case of a woman impersonating a man was that of Deborah Sampson, an eighteenth-century Massachusetts woman who was excommunicated from her church for dressing in men’s clothes and enlisting in the revolutionary army. Her true sex was discovered when she was hospitalized with a serious wound, and she was discharged from the service. She continued to wear male dress, work on a farm, and have love affairs with women. Eventually she married a farmer and had three children. Perhaps she saw that as an indigent, uneducated woman her future prospects outside marriage were grim. She was eventually decorated as a war hero and awarded a soldier’s pension (Mann, 1972).
The phenomenon of female transvestism in the seventeenth and eighteenth centuries is an interesting one. Given the sanctions against women assuming the male role, even in so innocuous a matter as dress, the motivation to do so must have been very strong. Some were homosexuals, believing that they had to emulate men in order to have relations with women. Some may have been sexually ambiguous, like the adrenogenital girls studied by John Money (see Ch. 4). One writer has suggested that they were the first feminists:
Mute as they were, without a formulate ideology to express their convictions, they saw the role of women to be dull and limiting. They craved to expand it—-and the only way to alter that role in their day was to become a man. Only in convincing male guise could they claim for themselves the privileges open to men of their class (Faderman, 1981, p. 61).
A temptation indeed for those few who were willing to risk all for what they saw as freedom from the oppressed state of being female.
“Romantic friendship”: bonding in a female world
Women’s love relationships with each other were a strong and stable feature of conventional eighteenth- and nineteenth-century life in America and England. The bonding of women in intimate, sometimes lifelong friendships was recognized and socially acceptable. Without the implicit or explicit sexual connotations of lesbianism (a word not in use at the time, whose meaning was perhaps not even dreamed of by conventional women), such relationships were nonetheless expressed in passionate, loverlike, even erotic letters, poems, and memoirs. Married or single, women lived in a social world that was strictly segregated by gender. Daughters were trained by mothers for life in the female world, wherein women were bound by the common events of their lives, such as pregnancy and childbirth. Supportive networks of friends and kin sustained and nurtured female bonding. By contrast, relations with men were severely restricted. Intimacy of any kind between young women and men was not permitted, and even after marriage the worlds of wife and husband were so different that it was commonplace and accepted for women to meet their needs for devoted caring and intimacy with each other.
The nature of women’s love relationships with each other has been described and analyzed by feminist scholars such as Carroll Smith-Rosenberg (1975) and Lillian Faderman (1981). Called variously “romantic friendship,” “kindred spirits,” or “Boston marriage,” such relations existed among both married and nonmarried women. They often expressed strong desire to live together, to be together always, away from the world of men. But few could realize such a dream in a time when alliance with a male meant the only economic security for which most women could hope. Yet the literature is filled with accounts of months-long visits of women with the specially beloved friend, of trips taken together, even of one moving into the home of a married friend. These relationships, intense as they were, were apparently non-threatening to the traditional value system, since they were not interpreted as sexual and were, in fact, an accepted part of the female world.
The prototype of romantic friendship is the story of Sarah Ponsonby and Eleanor Butler, daughters of upper-class Irish families, who ran away together in 1778. Pursued and caught by their families, they ran away again, thereby convincing everyone of their intentions. They were finally given small stipends to live on and managed to buy a cottage in Llangollen Vale in Wales, thus becoming known as the “Ladies of Llangollen.” For over fifty years they lived there together, inseparable, their devotion to each other recorded in journals in the most endearing terms (Faderman, 1981). Far from being castigated, they were admired and respected by many literary figures of the day, even having their romantic friendship recorded in verse by William Wordsworth. They won such approval because they were seen as chaste, morally pure women who eschewed frivolity and lived quietly in a charming cottage in the country, where they spent their time reading and gardening. Highly conservative in their behavior and orthodox in their moral and political views, they offered no offense to a society that did not suspect the “ladies” of being anything other than what they seemed: romantic friends.
In a now classic analysis of relations between women in nineteenth-century America, based on thousands of letters and diaries written by women, Smith-Rosenberg (1975) brings poignantly to light the existence of characteristic, unselfconscious, and deeply felt commitments that women typically made with other women. An example is revealed in the correspondence between Molly and Helena, two young women who met in 1868 while both were students in New York. Over the years their friendship deepened into a bond that lasted throughout their lives, though both married. The letters are filled with ardor and the sentiments of love. In an early thank-you note, Molly write: “Imagine yourself kissed a dozen times my darling. Perhaps it is well for you that we are far apart. You might find my thanks so expressed rather overpowering ...” (p. 7). Later, when they were having a crisis, apparently because of Molly’s decision not to live with Helena because of parental constraints, Molly wrote: “I wanted so to put my arms around my girl of all the girls in the world and tell her ... I love her as wives do love their husbands, as friends who have taken each other for life—and believe in her as I believe in my God ...” (p. 7).
Both Faderman and Smith-Rosenberg believe that such relationships, though expressed in the language of love and longing that we today associate with physical as well as emotional passion, were not sexual in the sense of physical erotic or genital contact. Their significance is that such female love existed in a particular historical context and that it was both socially acceptable and compatible with heterosexual marriage.
What was the fate of romantic friendship? In some environments, such attachments continued to appear well into the twentieth century. The founding of girls’ boarding schools and colleges beginning in the eighteenth century provided a setting wherein middle- and upper-class girls often formed close relations with each other. The intense fixation of one girl on another, an older student or an idealized teacher, variously called the “crush,” “flame,” or “rave,” was common in all-female schools and was recognized as a positive part of female development, as well as a challenge to discipline and selfcontrol: “Girls were advised that, if their emotional attachment did not improve their work, play, and ‘general power of helping others,’ it should be ‘rooted out with unhesitating courage and unwavering will’ ” (Vicinus, 1984, p. 617). So normative were such phenomena among girls and young women in schools and academies that sexologist Havelock Ellis took note of them in “The School-Friendships of Girls” (1936). While there was an unquestionable sexual element in the “flame” relationship, he said, it was not really a perversion, because it occurred too frequently, and it usually ceased when the girl left school and entered social life.
Social acceptance of intense emotional relationships among women, married and unmarried, younger and older, thus continued into the early twentieth century. At the same time, however, other social forces were generating another discourse that eventually made such friendships suspect if not dangerous. One was the increasing visibility of women in public life, in education and in the professions, and in the suffrage movement and other reform movements of the era. As the boundaries that separated man’s world from woman’s place began to become more diffuse, institutions that promoted the strength and bonding of women came to be viewed as threats to the social order, particularly to the institutions of marriage and the family. Women’s schools and political organizations became targets for conservative critics, and romantic friendships and schoolgirl crushes alike began to be seen as abnormal (Vicinus, 1984).
The ultimate demise of romantic friendship as normative among women was probably effected by the appearance of the early sexologists, such as Freud, Ellis, and Krafft-Ebing (see Ch. 7). Interest in describing and classifying sexual behavior was strong, particularly that which was nonnormative by the standards of the times. Thus women who engaged in “male” behavior, such as dressing in men’s clothing, agitating for women’s rights, or falling in love with other women, came to be labeled variants or deviants. It was around this time, in the World War I era and the years following, that the terms sapphist and lesbian came into general as well as clinical use to describe women who stepped out of the feminine role and, in particular, whose affectional orientation was toward other women.
While the labeling by the sexologists of such behavior as abnormal clearly had a stigmatizing and chilling effect on women’s affectional relations with each other, it has been pointed out that such attention made a positive contribution as well. Their vocabulary provided a language of sexuality where none had existed before, making it possible to see the commonalities among the experiences described by women and making more explicit the connections between their strongly felt and expressed emotions and their sexuality, however suppressed (Vicinus, 1984). Though not to be realized until later, the potential was there for increased understanding of the self and for the development of a collective consciousness that, more than anything else, could lead to liberation.
The cultural tradition
The development of a lesbian cultural tradition began in the post-World War I years with the publication in 1928 of Radclyffe Hall’s The Well of Loneliness and Virginia Woolf’s Orlando. The heroine of The Well was Stephen Gordon, daughter of an aristocratic English family, who wore mannish clothing, rode horses, and early on realized that women attracted her much more than men did. Hall, herself a lesbian, presents Stephen as the prototype of the masculine butch who is attracted to feminine women. The story is highly sentimental and ends tragically (perhaps the only way it could at the time). The Well was banned in England as obscene, though it has no explicit sexual content. Translated into many languages, for decades it was the lesbian novel, and its heroine Stephen embodied for many the lesbian identity. It became a target of feminist criticism because of the inference of abnormality in the portrayal of Stephen as an “invert” and because of its debilitating, joyless image of its lesbian characters and of lesbianism in general.
Virginia Woolf is best known to feminists as the author of A Room of One’s Own (1931), in which she discusses the reasons why there are so few women writers compared to men. In it she sets forth her famous dictum that, in order to be a writer, a woman must have a room of her own and enough money to be independent: in other words, privacy and freedom, rare conditions indeed for women of her day. Woolf’s novel Orlando (1928) is a fantastic tale of an androgynous character who changes from male to female over a centuries-long existence. Orlando represents the development of the ancient, aristocratic family of Vita Sackville-West, a poet and novelist with whom Woolf carried on a long and passionate relationship. The literary circle in which Woolf lived, the Bloomsbury Group, was noted for its liberal views and behavior, in contrast to the Victorian moral attitudes of the day, and several of them came to the public defense of Radclyffe Hall when her book was threatened with state censorship (Cook, 1979). Even so, Woolf’s nephew and most important biographer, Quentin Bell (1975), described her as “sexless” and dismissed her friendship with Sackville-West as unimportant and free of emotional involvement. Recent publication of Woolf’s letters to Sackville-West, however, tell a different story, and recent analysis leaves little doubt that they did in fact lead what they called a “Sapphic” life for many years (Gilbert and Gubar, 1985). Woolf’s work is certainly infused with a woman-centered consciousness that is far more enlightened and sophisticated than is Hall’s twisted and dismal tale. After her death little attention was paid to her work, and she fell into oblivion until her rediscovery by feminist writers and critics in the 1970s:
She understood that the freedom—personal, economic, and political— to which we aspire connects our work with passion to all our human relations. We were told, on the other hand, that she was a mad, virginal Victorian spinster-wife, precious and elitist. And so we were denied access to the most eloquent creator of a woman-loving socialist-feminist vision of the early twentieth century (Cook, 1979, p. 730).
In the unsupportive, often hostile climate of the time, there were, however, oases of acceptance, support, and pleasure for women fortunate enough to enter them. One was the Paris literary salon of Natalie Barney, which began around 1906 and flourished for some sixty years. Here were held literary and musical events as well as dinner parties, some attended by men as well as women, some for women only. Guests over the years included Colette, Gertrude Stein and her lover Alice B. Toklas, Radclyffe Hall, Edna St. Vincent Millay, Ezra Pound, Isodora Duncan, and William Carlos Williams, to name only a few of the illustrious who sought her out. Though well-known male artists and writers attended her salons, Barney’s circle functioned as a support group for intellectual lesbians in an environment where they could be themselves, free of concern of society and its moralisms.
After the First World War, Barney created what she called an Academie de femmes, whose purpose was to bring together French, British, and American women writers to salons devoted to literature by women. Barney’s major interest was in furthering the careers of women in literature, and her interest extended to financial and emotional support for those who needed it (Faderman, 1981).
But “history tends to bury what it seeks to reject,” as Blanche Cook (1979) observed in her paper on lesbianism and the cultural tradition, and for most of this century, lesbian tradition, culture, and literature have been hidden from view, absent from the public record. Once again, it was not until feminist scholars began their work in the 1970s that those obscured voices could begin to inform the present.
Anyone interested in lesbian history and culture today finds a wealth of resources. The Lesbian Herstory Archives in New York is both a library of published works and a clearinghouse for such material as letters, diaries, and other unpublished material. Recent books have explored historical, political, and sexual theory, and feminist journals such as Signs, Chrysalis, and Sinister Wisdom publish lesbian feminist writing. A good example of contemporary lesbian writing is Our Right to Love: A Lesbian Resource Book (Vida, 1978).
Most significant in revealing the rich lode of lesbian writing is the Arno Press reprint series edited by Jonathan Katz. This series includes fifty-four books and the entire run of The Ladder, the journal of the Daughters of Bilitis, a lesbian social and activist group formed in 1955. The series includes anthologies and bibliographies, as well as archival material such as Government v. Homosexuals, with the infamous McCarthy hearings of the 1950s. Also in the series are biographies and memoirs of the 1920s and 1930s, and paperback novels of the popular genre of the 1950s. Another collection of documents from lesbian and gay history is Katz’s (1976) Gay American History: Lesbians and Gay Men in the USA.
Thus the historical and cultural record is being discovered and restored and can no longer be buried or denied. It also cannot be denied that mainstream society still regards lesbianism not as a parameter of personal and social identity but as a sexual anomaly to be denied or glossed over, as happened with Sappho and Virginia Woolf, when it conflicts with cherished values. The continuity of stigmatization flows not only from religious and legal judgments of past centuries but from later medical and scientific judgments as well. Though residuals of these persist in society’s perceptions and evaluations, the word lesbian no longer carries, as it once did, the scientific imprint of pathology.
Lesbianism and the Medical Model
While homosexuality had historically been dealt with by religious and civil authorities as both a sinful and a criminal offense, it began to capture the attention of medical science early in the century. As noted earlier, lesbian sexuality had not attracted the attention of either religion or the law to the extent that male homosexuality had, and early medical attention to the subject was no exception. Women were a subordinate and inferior class, and this evaluation extended to their private acts as well.[49] Women’s sexual needs were not seen as either as important or as urgent as men’s were, and their sexual behavior was less a matter of concern or comment. When authoritative opinion, be it religious, legal, or medical, did focus on relations between women, it related specifically to sexual behavior and did not partake of the larger dimensions of definition discussed earlier. In other words, the lesbian was identified by her sexual behavior, extracted from the other elements of her identity.
A particular confluence of events that brought more attention to lesbianism than ever before occurred in the early years of the century. One was the appearance of the New Woman. The other was the developing interest of psychiatry in sexual behavior, especially that of a “deviant” nature.
The struggle for women’s suffrage, women’s participation in social and political movements such as the temperance campaign and labor unionization, World War I with its utilization of women in military and industrial roles, and increasing educational and economic opportunities for women contributed to the appearance of the New Woman in the early decades of this century. New Women were epitomized by those who cast off old familial roles, entered public life, and insisted upon independence and freedom from traditional definitions of womanhood. Among them were such women as birth-control pioneer Margaret Sanger, political radical Crystal Eastman, and lesbian writers such as Gertrude Stein, Natalie Barney, and Radclyffe Hall. Women who identified themselves with the New Woman prototype were not necessarily lesbians, and probably most were not. They were demanding access to the kinds of freedoms that men had, such as professional opportunities and political power, and even such mundane symbolic perquisites as the right to smoke and drink in public. Some, such as Hall, abandoned feminine attire and adopted male clothing.
Such transgression of the gender roles so basic to Victorian society aroused great concern in some quarters. If women rejected the feminine role, what other role was there for them? If they insisted upon behaving like men they were deviant by definition. And if some of them went even further, refusing marriage and choosing women to share their most personal lives, they were clearly abnormal.
Psychiatrist Richard von Krafft-Ebing (1906) was one of the first to connect elements of “masculinity” in women, such as feminist ideas and male dress, with lesbianism. He described four types of lesbians. The first and least deviant was the outwardly feminine woman who was attracted by mannish women. The second type preferred to dress in male clothing, a female counterpart to the effeminate male. The third was a true “invert,” the woman fully assuming the masculine role. The final and most extreme type, said Krafft-Ebing, had female genitals, but everything else about her—thought, action, and apperance was masculine. Krafft-Ebing believed that lesbians suffered from a congenital form of inversion of sexual desire, usually manifesting itself in childhood and characterized by gender reversal, i.e., the insistence upon taking on the male role to a lesser or greater degree.
Krafft-Ebing reported on a number of lesbians whom he had studied and “treated.” Since the normal destiny of women was marriage, and women were essentially asexual and passive, the lesbian, who violated all these tenets, was not a “real” woman. He attempted to “cure” some of his patients by using hypnosis to stop them from masturbating and to encourage heterosexual feelings. He later came to believe that heterosexual women could be seduced into lesbianism, often by learning about masturbation. He concluded that any woman was suspect who wore her hair short, had masculine interests, or advertised in the newspaper for a lady companion.
Havelock Ellis (1936), sexual radical though he was for his time, also espoused the doctrine of the congenital invert as explanation for women’s sexual attraction to women. He even saw romantic friendship between women as rudimentary forms of lesbianism, thus classifying them also as abnormal. For Ellis, the “active invert” felt more comfortable in the masculine role, by actions, occupations, and dress, owing to an “organic instinct.” Lesbian couples who copied the heterosexual model, wherein one took the masculine role, the other the feminine, posed a problem. Who was the feminine invert? Ellis (1895) decided that she was one of the class of women who differ from the normal in that they are not repelled by advances from other women. They have good figures and are always “womanly,” the “pick of the women whom the average man would pass by.” As a class, he said, they seemed to possess a genuine, though not exactly sexual, preference for women over men.
In 1920 Freud published the case of an eighteen-year-old female patient, “The Psychogenesis of a Case of Homosexuality in a Woman,” in which he noted that homosexuality in women had been neglected by psychoanalytic research. His report of this single case did little to remedy the situation, but it is indicative of his thinking about the issue. In an earlier paper, “The Sexual Aberrations,” he had stressed masculinity in lesbians who sought feminine partners, and in the case of his young patient, he likewise found “masculine traits” in this “beautiful and well developed girl“: “acuteness of comprehension,” “lucid objectivity,” and the preference for being “lover rather than beloved.” He remarked that the girl was not in any way ill, but had been brought by her parents who were seeking a cure for her “nervous and unruly” behavior. As a child she had been full of high spirits, always ready for romping and fighting and competitive with an older brother. She was in fact, Freud wrote, “a feminist; she felt it to be unjust that girls should not enjoy the same freedom as boys, and rebelled against the lot of women in general.”
What had brought about this condition? The “psychogenesis” of her case had two elements. First, she had wanted a baby by her father, but he had given one to her mother instead, causing her in her frustration to turn away from men altogether. Second, she envied the penis of her older brother and, denied this, she compensated by developing a “masculinity complex“ which accounted for her expressions of feminist ideas and envy of the status of men.
Interestingly, this young woman had never had sexual relations with a woman. She spoke of the “purity” of her love, which had been expressed with kisses and embraces and fantasies of living with her beloved. In other words, her behavior was like that of the romantic friendships of an earlier era, before such relationships came into the purview of science.
In any case, Freud’s interest in lesbianism seems more intellectual and analytic than that of his colleagues, such as Krafft-Ebing, who did not hide their moralistic horror at the spectacle of such perversion. His interest was more in trying to explain its psychic origins in the early psychosexual development of the child. He said more than once that he did not believe that adult homosexuality could be cured, and, further, he observed in “The Sexual Aberrations” that “inversion” is often found in people who show no deviation from the normal, whose mental capacities are not disturbed.
Throughout the first half of the century, with few exceptions, the medical literature on lesbianism had two basic features; first, assumptions that lesbianism is an abnormal condition, an illness or mental disorder; second, theories of causation. A sample of the latter includes: fear of the opposite sex and of the penis; the desire to possess the mother; heterosexual trauma (including rape); seduction in adolescence by an older woman; tomboy behavior; masturbation, resulting in clitoral fixation; living in all-female groups; and physical factors, such as genetic and endocrine factors (Rosen, 1974). The great majority of such studies were written by men, commenting upon women who were medical patients or undergoing analysis or other psychotherapy.
Thus the belief that lesbianism represents personality pathology, that is it deviant behavior and needs to be corrected if the woman is ever to be normal, has been the prevalent view of the mental health community until recent times. The homosexual, female or male, was almost by defmiton emotionally disturbed, frustrated, and unhappy. Even if such symptoms occurred, however, they could have been partly understood as effects of the social stigma, persecution, and discrimination that in the past have driven those who loved others of their sex into concealment and secrecy, often alienating them from society and family.
“Once We Were Sick and Now We Are Well”: The Shift in Perspective
Even in the midst of the early pathology-oriented studies that carried the message “lesbians are sick,” however, there were a few unattended voices that did not concur. A 1929 nationwide study of the sex lives of “normal” women found that about 25 percent had had sexual experiences with other women at some time in their lives. These women were healthier, better educated, and more likely to have been gainfully employed than were the women who had never had such experiences (Davis, 1929). Similarily, a gynecologist who collected data on his patients’ sexual experiences observed of those who reported having had sexual experiences with women: “Good health and steady occupation is the rule; appearance, dress, and social status are without idiosyncrasy and above the average” (Dickinson and Beam, 1934, p. 203). Such studies did little to dispel the prevailing climate of belief in the morbidity of lesbianism, and it was not until Kinsey et al. (1953) that the message that homosexuality was a normal variant of sexual behavior received widespread notice. During the 1960s and 1970s, numerous studies using nonclinical subjects found no significant differences in mental health or adjustment between lesbians and heterosexual women. Responding to this new research, and to pressure from lesbians and gay men who did not regard themselves as abnormal, the American Psychiatric Association in 1973 decide to remove homosexuality from its status as a mental disorder.
“Once we were sick and now we are well”: Susan Krieger (1982), in her review of social science literature on lesbian identity and community, used this simple statement to describe the shift in the lesbian paradigm from pre- to post-Kinsey research. An important component of the shift is the professional identity of the researchers, reflected in their methodology. Earlier writers who focused on pathology were almost all male physicians or analysts, who often drew conclusions from one or a handful of cases. More recent researchers are much more likely to be women, some of them lesbian-identified, using the more sophisticated methods of contemporary social science. In addition to conventional studies that compare groups of lesbians to groups of heterosexual women on certain variables, today’s researchers use participant-observation, in-depth interviewing, and survey methods. The focus of the research and the questions it asks have changed, too. No longer concerned with the issue of assumed pathology, researchers have moved beyond the identification of the lesbian with her sexuality to a broader concept of lesbianism as a lifestyle choice, linked with a sense of personal identity (Krieger, 1982). Thus much of the recent research looks at lesbians in their social context: influences to which they attribute their lesbianism, relationships in couples and in communities, the formation of lesbian identity in an alienating environment.
An example of a contemporary study is Susan Krieger’s The Mirror Dance: Identity in a Women’s Community (1983). Based on a year of participant-observation and interviews in a midwestern women’s community of mostly lesbians, it tells in the women’s own words of their identification with the community, of their social and personal relationships, of their connections with the outside world of work, family, and straight society, and of their feelings about privacy. Some examples from these areas:
Identification: It didn’t seem to be just any women in the larger community who happened to be lesbian, Bronwyn believed. It was a particular group of women who were lesbians and a few who were not, a group of women whose lives touched, who came in contact socially and emotionally (p. 8).
The community, felt Harriet, was made up of people who found solidarity and comfort in participating. She did think you had to consciously join it, but she didn’t think there were any rules about being in it. It was basically an open association, except for the one requirement: that you had to be supportive of women who were trying to build healthy relationships with other women (p. 16).
Relationships: The problem of time alone versus time with people was, thought Gloria, the most controversial theme in relationships in the community, not a problem only she and Leslie had. The problem was that one person would want to be more private, havfe more time alone; the other would want to be more public, more social. She thought it began because opposites attracted. They complemented each other. They brought out things in each other that were appreciated. Then the two people had this conflict (p. 75).
She was impressed with their efforts, said Kathryn, their intense, persistent efforts at loving, at friendships, their efforts not to lost people. Even when you were breaking up, they knew, you were still on the same side of the fence. These relationships were hard, she felt. The community tried to use everything it possibly could to solve the problems.... The main problems were the lack of differentiation and the fusion which led to some of the crazy-making, and the intense disappointment when the relationships broke up or weren’t as different‘or as perfect as people expected they would be (pp. VO- SO).
The outside world: She didn’t tell people at her jobs that she was a lesbian, said Mitzi, She tried to say everything but that. Sometimes she wanted to talk about it with the women, though, so she used other words. She just never said she was a lesbian or used the label because she was worried she would lose her job—cleaning houses. People would be scared for her to come into the house.... If you said you were a lesbian, people got worried about the word and forgot what you were telling them ... (p. 146).
Her family knew, said Connie. They found out. They got hold of one of her letters once. It happened to be the most explicit letter she had ever received. She was living at home in a small town near Queens Crossing and working and going to school. Somehow her parents thought she would straighten up. Then when she moved here to take a job, they thought it was all over. Little did they know she was moving to a bigger lesbian community (p. 156).
Privacy: There were certain things you learned only after you got more familiar with people, felt Ruby. Like when she had been staying with Natalie and Jo this spring, she had learned how to tell about times when they wanted to be alone together. During those times she tried to be careful about their space. For example, if she needed to go into the bathroom and they were in (here talking (because the bathroom in their house was a place where one person took a bath and one or more people talked to them), she needed to ask permission first; whereas if they had just come home from work and were talking in the bathroom, she wouldn’t have to do that (pp. 164–65).
It was something some people seemed to need more than others, said Leslie. She had always been a person who had to have it and at certain times especially. She might write in her journal then, or listen to music, or spend lime on photography. During that time she was thinking and calming down and refueling (pp. 165—66).
The history of research on lesbians has some commonalities with the history of research on women in general, on blacks and other minorities. First, they do not appear in the social science literature; when they begin to appear, they are found deviant and exotic; then they begin to be defended; finally, when perceived as ordinary, they begin to be included with other partly understood phenomena (Krieger, 1982). Lesbians are not yet perceived as ordinary. They are however being defended, and research about them is beginning to edge its way into the mainstream literature of science.
Contemporary Issues
The liberation of sexual attitudes from old prejudices and misconceptions has resulted in increasing acceptance of homosexuality in both sexes. Kinsey found that one-tenth of his sample expressed tolerance for homosexuality, whereas in the Playboy survey of the 1970s (see Ch. 7), one-half of the respondents thought that homosexuality should be legal and agreed with the statement “There is some homosexuality in all of us.” The gay liberation movement, whose goal is to free its consituents from social, legal, and economic sanctions against them and their lifestyles so that they may receive the same treatment accorded to others members of the society, has encouraged many lesbians and gay men to identify themselves. Members of the lesbian contingent of the feminist movement see themselves as subject to dual discrimination, both as women and as lesbians. This group believes that women will never have true freedom and equality until they are independent of men, sexually as well as in every other way.
In view of the changing social climate, one might expect the incidence of homosexuality to increase. But this does not appear to be the case. While the data are less than completely reliable, Kinsey (1953) and Hunt (1974) found remarkably similar incidences in their samples. About one in five single women and one in ten married women eventually have some homosexual experience. It is difficult to make any definitive statement about the incidence of homosexuality since, as Kinsey pointed out, people cannot be placed in two discrete categories, heterosexual and homosexual. Homosexual experiences in childhood are quite common, and among girls in the thirteen-to-nineteen age range, about 6 percent have one or more homosexual experiences (Sorenson, 1973). The incidence of exclusive homosexuality among women is estimated to be between 0.5 and 1 percent of the adult female population. Among younger groups, the incidence is higher, perhaps 2 percent, with 15 percent having occasional lesbian relationships (Wolfe, 1980).
Part of the problem with estimating incidence, too, is related to the issues of definition discussed earlier. The words, homosexual and lesbian do not have the same connotations; the former relates specifically to sexual behavior, while the latter, as we have seen, has much broader and as yet not clearly defined implications. Restricting the discussion to sexuality for the moment, some individuals may have only a few homosexual experiences in an otherwise heterosexual life. Others may be bisexual, interested equally in sexual activity with partners of both sexes. Some engage in homosexual behavior only under conditions of separation from the opposite sex, as in prisión or other sexually segregated situations. Thus, except for persons who are exclusively homosexual, the question of who is and who is not has no meaningful answer.
As we have seen earlier, much of the older literature was concerned with the search for causes for what was seen as abnormal behavior. Since no one asks, What causes heterosexuality? the question, What causes lesbianism? implies that it is deviant, even though it is widely recognized that homosexuality is not a discrete behavioral entity, like vegetarianism. Even so, behavioral scientists continue to be curious as to why a minority of the population pursue a sexual perference and even a whole way of life that is guaranteed to be problematic for them, often causing them to be rejected by family and society, generating pain and suffering for many.
Among those interested in the development of sexual preference have been researchers of the Alfred C. Kinsey Institute for Sex Research at Indiana University, who studied the family relationships, gender conformity, and other growing-up experiences of both homosexual and heterosexual women and men in the San Francisco area (Bell et al., 1981). They found that sexual preference is likely to be determined by adolescence, in the form of sexual feelings that may occur several years before overt homosexual activity appears. Both the female and the male homosexuals tended to find early heterosexual experiences ungratifying, again reinforcing the importance of preadult feelings in the development of homosexual preferences. A strong link was found among both the women and the men in the study between gender nonconformity in childhood and adolescence and the development of homosexuality. However, a substantial number of the respondents who became homosexual did not display gender nonconformity; thus such behavior is childhood does not inevitably lead to future homosexuality. Further, gender nonconformity was more important as a precursor of homosexuality for the males than for the females.
Identification with opposite-sex or with same-sex parent was not connected to sexual orientation, though poor relationships with fathers seemed to be more salient than whatever relationships the subjects had with their mothers. The authors conclude: “What we seem to have identified is a pattern of feelings and reactions within the child that cannot be traced back to a single social or psychological root” (p. 192). Given so complex a variable as sexual preference, we learn once again that it is a mistake to search for the single cause, attractive though that might be, and to accept that peoples’ preference, social, emotional, sexual, for others of their sex, is the result of complex interactions of influences from sources both internal and external to the person.
Raising a related issue that impinges upon the political implications of lesbianism, poet and author Adrienne Rich (1980) examined the nature of lesbianism and what she calls “compulsory heterosexuality.” Instead of asking, Why are some women lesbians? she asked, Why are most women heterosexuals? She sees heterosexuality as a beachhead of male dominance, embedded in the assumption that most women have an innate sexual preference for men. Male power, she argues, has enforced compulsory heterosexuality on women, convincing them that marriage and a sexual orientation toward men are inevitable, even if they are unsatisfying and oppressive. The implication here is that such writers consider lesbianism in light of female and male power issues and not as an isolated phenomenon with “causes” and “treatments.”
Dimensions of Lesbian Experience
The question, Who are lesbians and how do they live? is no more easily answered than is the question, Who are nonlesbians and how do they live? As Del Martin and Phyllis Lyon point out in their classic 1972 book Lesbian!Woman, lesbians exist in all races, socioeconomic levels, occupations, and geographic area. They live in apartments, houses, and institutions, in cities, villages, and on farms.
Lesbian women do not fit any stereotype of personality or appearance. Some adopt masculine or feminine roles similar to the traditional male and female roles in martial relationships. The “butch,” or “dyke,” for example, may wear male clothes and take a protective stance toward the “femme,” who appears more conventionally feminine in dress and mannerisms. The adoption of such roles is more common among older lesbians; it is an imitation of traditional marriage and is much less frequently seen among younger lesbians today. In fact, according to a large-scale study of American couples that included lesbians and gay men, today’s lesbians are trying to reject both female and male behavioral stereotypes. Neither partner wants to be the dependent one or the sole provider. Both usually work and try to contribute equally to the relationship, including sharing housework. Money can be a problem, because even with two wage-earners, lesbian couples’ income level was lower than that of heterosexual or gay male couples. An interesting point was that leisure-time activities could potentially create more of a bond for lesbian couples than for heterosexual couples because same-sex couples are more likely to enjoy the same kinds of activities (Blumstein and Schwartz, 1983).
The sexuality of lesbians has been the aspect of their existence that has most intrigued norihomosexual people. The sexual activities of lesbians may include all the kinds of sexual behaviors observed in any human group: kissing, caressing, mutual masturbation, oral-genital stimulation, and breast stimulation are most common. The use of an artifical phallus, or dildo, is rare. The lesbians in one study mentioned mutual masturbation and giving and receiving cunnilingus as their most frequently used and most preferred sexual techniques (Bell and Weinberg, 1978).
The popular view equates the lesbian with her sexual orientation, suggesting that lesbians are obsessed with sexual concerns and activities. But a comparison of lesbian couples with heterosexual married and cohabiting couples and with gay male couples found that the lesbian couples had sex less frequently than any of the other couple models (Blumstein and Schwartz, 1983). A study of fifteen hundred homosexuals in the San Francisco Bay area found that, for most of them, sex was not the predominant concern of their lives. Lesbians are more likely than gay men to desire relatively permanent, sexually exclusive, and emotionally close relationships (Peplau et al., 1978). This seems to reflect culturally based norms for love and personal relationships, by which girls and young women learn to value close, secure, and caring bonds with others, as well as fidelity and commitment. Since girls who become lesbians are socialized within the same value systems as are their heterosexual sisters, it follows that social prescriptions for women’s orientation toward love and love relationships would equally influence them.
By contrast, there is evidence that some lesbians value independence, strength, and intelligence and choose personal autonomy over traditional feminine values. Their concern for autonomy and independence suggests a desire for separate interests and friends outside a primary love relationship. One study found both these orientations in a sample of 127 lesbian women. While most of them reported that their relationships with their partners were close and satisfying, one group endorsed attachment values of togetherness and security, and the other endorsed autonomy themes of equality, greater valuing of work and education, and a deemphasis on sexual exclusivity. The latter group appeared to have been more influenced by feminist ideology and were more likely to be lesbian activists. But attachment and autonomy values in a primary relationship are not mutually exclusive and can interact with each other. It is possible to be oriented toward both ideals, as were some women in the study (Peplau, et al., 1978).
The growth of research interest in lesbianism and the interpretations of its meaning by feminist scholars in psychology, anthropology, history, and literature are beginning to bring lesbianism out of the shadows of obscurity and defamation. This movement, born out of feminism and gay activism, offers the promise of bringing us to a greater appreciation of the cultural and sexual diversity that has always been observable among earth’s people.
12. Psyche and society: women in conflict
[T]here is no sharp line between those who act out their conflicts directly and in forms unacceptable to society and all others who struggle with them at some time in their lives, but do not act in this particular way. It is We one studies when one studies any pari of the human race, never They.
—Gisela Konopka, The Adolescent Girl in Conflict, 1966
While women are not unique from men in the kinds and intensity of the conflicts they experience in contemporary society, the incidence and patterns of these conflicts, the reactions they evoke, and the ways they are dealt with are sufficiently different to justify special consideration. Some of the problems women have result from the violation of social norms and standards of behavior. Others are the direct outcome of the victimization and exploitation of women that have historically characterized our society as well as others. Still others reflect intrapsychic distress and interpersonal conflict.
In the language of social psychology, norms are ways of behaving that are typical for a group, and that reflect its attitudes about what is right and wrong, good and bad. Normative behavior is behavior that is within the limits defined as normal, that is, limits that include the behaviors displayed by most of the group. Thus it is normative in our society for children to go to school; for parents to care for their own children; for all persons to respect the property rights of others; and for men and women to marry each other and to have only one spouse at a time. Norms are essentially reflections of value judgments that are tacitly agreed upon by the influential members of the society and that establish, among other things, the guidelines for the socialization of children. All human societies have norms that regulate the behavior of their members; violations are more or less severely punished, depending upon the importance of the norm: one who wears inappropriate clothes to a public event may be stared at, while one who wears no clothes at all may be put in jail. Such judgments about behavior vary greatly from one society to another and even between groups in a single society. But they all have one element in common, and that is that they are perceived as necessary for the survival of the group and for the growth to maturity of the individual.
This chapter deals with women whose behavior violates such important norms that they are a threat to the social order and must be segregated and confined; with women who are victims of rape, battering, and sexual harassment; with pornography; and with women whose behavior causes them to be seen as mentally disturbed and in need of treatment to restore them to normal and to alleviate their psychological discomfort and the concern that others have for them. The observable gender differences that abound in these areas, as in others we have looked at, are outcomes of a complex interaction of historical precedents, individual histories, sociocultural pressures, socialization practices, and biological factors. Although one of these elements may contribute more than the others to a particular case, it is a mistake to look for the single cause as some observers do. It is no more enlightening, for example, to say that a certain woman is suicidal because her father died when she was ten, or because an oppressive society defines her “place,” than it is to credit her symptoms to demonic possession. No one, male or female, is exempt from pressures from all these sources and more, and individual variations in morally and socially sanctioned behavior result from the many possible combinations of social and environmental influences impinging upon the unique and vulnerable individual.
Early Life Adaptation of Girls
Culture and biology combine to favor the psychosocial adaptation of girls in our society during at least the lirst decade of life. Those behavioral and learning problems that are commonly manifested by children and the relative incidence of these in the two sexes are shown in Table 12.1.
The manifestation of behavior that is troublesome either to the child, to her or his parents, or to society, behavior that is regarded as pathological or that brings the child into conflict with laws and mores, is unquestionably less frequent among young girls than boys. The research on sex differences reviewed in Chapter 5 indicates that several factors interact to produce this effect.
Table 12.1 Sex ratio of problematic behavior in children{9}
| Problem | Male/female |
| Hyperactivity | 5:1–9:1{10} |
| Elimination | |
| Enuresis | 2:1 |
| Encopresis | 6:1 |
| Asthma | 2:1 |
| Speech disorders | 3:1 |
| Reading problems | 3:1–5:1{11} |
| Delinquency | 3:1 |
| Drug abuse | 2:1 |
| Mental retardation | >1:1 |
| Infantile autism | 4:1 |
| Childhood psychoses | 2:1–9:1{12} |
| Outpatient admission to mental health facility | 1.7:1 |
-
The additional genetic material on the second X chromosome conveys some protection to females against non-lethal sex-linked disorders that add stress to the life of the affected individual.
-
The lower incidence in girls of congenital neurological abnormalities is reflected in lower rates of mental retardation, learning disabilities, hyperactivity, poor impulse control, and personality disorganization. Schizophrenic children often shows signs of neurological impairment, such as deficiencies in motor coordination, muscle tone, gait and balance, and the capacity to integrate sensory stimuli. When schizophrenic children are grouped on the basis of whether or not they have these signs, the ratio of boys to girls is higher in the group that has such signs, suggesting that neurological impairment is more often involved in childhood psychosis in boys than in girls (Goldfarb, 1970).
-
The advanced developmental maturity of girls compared to boys facilitates their early learning and socialization, giving them an advantage in developing coping and interpersonal skills. The reinforcement that girls receive for these skills may promote the salience for them of affiliative behavior, reducing the probability that they will alienate significant people by hostile and aggressive behaviors.
-
The “feminine” tone of the early childhood environment, in which girls are cared for and later taught by same-sex models, facilitates the adoption of socially approved roles and reduces the potential for conflict with authority.
-
The cluster of aggressiveness-competitiveness-resistiveness differentiates girls from boys, who have a lower threshold for the evocation of such behaviors. Since a major thrust of socialization practices is control of aggressive and antisocial behavior, girls adapt more easily to the adult expectations of such control. If we assume that the sex difference in aggression among young humans has a biological determinant[50] as the research clearly indicates, and that more boys than girls will display a higher rate of such behavior, then it follows that the agents of socialization, parents and other adults, will direct more stringent efforts toward curbing their unacceptable responses, applying nonphysical and physical punishments. In 1974, Maccoby and Jacklin reported that fathers were more punishing of aggression in their sons than in their daughters. Thus boys, more frequently subject to methods of aversive control, experience more conflict with authority figures and are more likely to develop attitudes of hostility and resistiveness toward even legitimate authority. Such a snowballing effect can occur when the biological and developmental differences between the sexes in early life are not understood, and when inappropriate or ineffective methods are used by adults in their attempts to modify behavior and bring it into line with whatever their idiosyncratic and prevailing cultural criteria are. To the extent that girls behave differently from boys, they elicit a different kind and level of response from adults, and this also has a cumulative effect, mediating in general a more positive adaptation of young girls to the norms of a demanding society.
These factors taken together should be thought of as an etiological basis for the childhood sex differences in problem behavior. Together, they predict a higher incidence for boys than for girls of such behavior. The persistence of problem behavior into later life is dependent not only on its historical antecedents but also on society’s reactions and its attempts to deal with it.
A distinction is made between the kinds of judgments concerning the behavior of young children in our society and those that are imposed on the behavior of older children and adults. Atypical behaviors that give rise to concern in parents of young children are usually classihed as behavior disorders, learning disorders, or the more serious childhood psychoses. When young children exhibit antisocial behavior, such as stealing or assault on an infant sibling, they are not labeled delinquents or felons, because they are not considered to be responsible for their behavior. Instead, they are considered to be emotionally disturbed and in need of treatment. Older individuals who violate the property or person of others are more likely to be held responsible for their behavior and to be incarcerated and punished. Disturbances and problems that adolescents and adults have that do not violate a law, such as emotional distress and occupational and marital discomforts, are presumed to be mental illnesses or problems of adjustment amenable to treatment by trained personnel in appropriate facilities. Thus an important dichotomy develops in the classification of behavior problems of older children and adults, some behaviors being classified as delinquent or criminal and others as due to mental or emotional disorders. This developmentally emergent dichotomy does not exist for young children. That it is altogether a social artifact is obvious. But it has important effects for the research findings on later sex differences in atypical behavior: among adults, more males than females go to jail; more females than males go to psychiatrists.
Delinquency and Crime
Nowhere in ail the documentation of sex differences does one find more striking examples than in the literature on delinquency and crime. In fact, the differences between males and females in patterns of delinquent behavior, rates of arrest and imprisonment, treatment by the criminal-justice system, and behavior in correctional institutions are so important that attempts to understand delinquency and criminality have had to deal separately with them. Such behavior by men and women cannot be explained by a single model; thus the female offender joins the list of exceptions to theories built upon observations of males.
Delinquency in girls
Although there exists a very large body of theory and research on delinquency, most of it deals with boys. Studies of delinquency in girls and attempts to explain it have been few. Earlier writers simply ignored it, as if it didn’t exist. For example, in 1954, Talcott Parsons explained delinquency in boys as a rebellion against the female-oriented Western family and their difficulty in making an appropriate male identification. The girl had a more favorable opportunity for healthy maturing, since her mother was readily available to model for the functions of wife and mother. While this may be true, it clearly glosses over the occurrence of delinquency in girls. Another study of adolescent behavior blamed delinquency on the long postponement of adult roles (Block and Niederhoffer, 1958). Again, it was presented entirely in relation to the boy and his frustration at being barred for so long from the roles of worker and father. Whether or not a parallel situation exists for girls was not considered.
More recently, another theory of the adolescent girl in conflict was presented. It includes four concepts: the unique pubertal biology of girls, the nature of their identifications, the changing cultural position of women, and the “faceless” adult authority with resulting loneliness (Konopka, 1966).
Puberty with its dramatic body changes ushers in the role of sexuality and the possibility of pregnancy. Thus sex has a more pervasive meaning for girls than for boys and acquires intensive romantic connotations as a love offering, a weapon, or an outlet for frustration and rebellion. Parental role models for identification may be absent, inadequate, or so punitive and rejecting that constant conflicts make the development of an emotionally mature sense of self impossible. Changes in the cultural roles of women have led to raised expectations for education and vocational opportunities which may not be available in fact, and increased awareness of double standards in sex roles create resentment and hostility against a society that provides more freedom and access to its goods to boys.
These three conditions apply to all girls but lead to delinquency only under special circumstances. They are potent sources of problems, their resolution dependent on factors in the life of the individual. The girl who seeks love through sexual acting out, who flees from harsh conditions and from physical and emotional trauma, and who sees no way out of her situation comes into conflict with society and its values. She distrusts authority at home, in school, and on the street as inimical, and this distrust grows to include all adults and even peers. The resulting behavior leads to rejection, school failure, and feelings of worthlessness, which in themselves increase frustration and rebelliousness generating further conflict with society (Konopka, 1966).
Many crimes for which girls are taken into custody are individualistic, such as truancy and running away. Group delinquent behavior, as manifested in urban male gangs, is much less prominent in female delinquency. All girl gangs are most likely to be auxiliary to boys’ gangs, as were the Vice Queens studied by Fishman (1966). Girls’ gangs are loosely organized and rarely take on group activities of their own. While members of girls’ gangs may participate in the delinquent acts of boys’ gangs, such as fighting and drinking, such behavior is not common and does not provide status to the girls. Status derives from male affiliation and is centered around sexual activity. Studies show that girls in gangs have only about one-tenth the illegal involvement of male groups. Their group violations tend to include shoplifting, truancy, drinking, and drug usage, rather than violent personal crimes. Female delinquency is most likely to appear in mixed-sex peer groups with male members as instigators or role models. The higher the male-female ratio, the higher the rate of delinquent behavior by the females (Weisheit, 1984).
An interesting study of black youth of whom 40 percent were affiliated with gangs found that of 182 reported delinquent acts only 4 had been partially planned by girls. Delinquent boys were asked what would have happened if a female had been involved in the act for which they were in custody. Sixty-eight percent said the planned act would have been postponed or cancelled; 24 percent said the female would have been ignored; and only 8 percent would have included the female in the act. It appeared that females were rarely involved in the delinquent acts of the male gangs and that the presence of females might even have had a suppressing effect on the delinquent behavior of the male gangs (Bowker et al., 1980).
Juvenile delinquency offers a fertile field for the study of both sex differences in behavior and the double standard of treatment of offenders. On the record, boys are significantly more delinquent than girls. Most studies report a male-female arrest ratio of about five to one. Recent FBI Uniform Crime Reports (1980–85) indicate that females account for about 19 percent of underage eighteen arrestees charged with economic and property crimes and about 12 percent of those charged with violent personal crimes. It appears that the large majority of female juvenile offenders are arrested for “status” violations, that is, for behavior that is not illegal for adults, such as truancy, promiscuity, running away, or being incorrigible, offenses with which boys are rarely charged. For example, a study of juvenile institutions in one eastern state found that 31 percent of the girls and none of the boys were incarcerated because of their sexual behavior (Rogers, 1972).
Thus the criminal justice system is more likely to punish girls for offenses that violate sexual mores and parental authority. On the other hand, girls are dealt with more leniently when they commit “real” crimes. The paternalistic attitude of society toward girls mediates the view that their sexual and gender-role transgressions call for protective and punitive measures, while traditional attitudes of chivalry result in their actual crimes being dealt with less harshly than boys’. For example, one study revealed that 45 percent of girls charged with status or gender-role violations were detained before trial, compared to 24 percent of those charged with misdemeanors and 35 percent of those charged with felonies (Chesney-Lind, 1974).
Women and crime
Considering that women constitute more than half the population, they are remarkably underrepresented in crime statistics. Several theories have been advanced to account for this. Cesare Lombroso, a nineteenth-century Italian criminologist, believed that criminals were born with certain physical characteristics that distinguished them from other persons and predisposed them to lives of crime. But he found that his theory did not fit women criminals, who did not differ from moral women with regard to physical anomalies. He attempted to explain this on the basis of women’s biology and their social roles. Women showed fewer physical stigmata because they were less deviant from their norms on biological characteristics, and because of a selection factor whereby men choose women who had fewer physical anomalies. They committed fewer crimes because of their sedentary social roles and because of a less active cerebral cortex, which when irritated led to hysteria and sexual problems rather than to crime (Lombroso and Ferrero, 1916). Thus he decided that most female criminals, unlike males, were not born criminals but were led into crime by lovers and husbands. Occasionally, however, a born female criminal would appear who was more diabolical than the male.
Otto Pollack in his classic book The Criminality of Women, published in 1950, presented the thesis that the criminality of women is vastly underreported because it is masked in their conventional roles of mother, domestic servant, nurse, shopper, and so on. For example, women have much more opportunity to commit crimes of abuse against children that often go unreported. They can conceal theft in their roles of servant or shopper. In addition, because of women’s less active role in society, they are more often instigators of crime committed by men than perpetrators. Thus the real incidence of female crime is not known because of its devious nature, and because of women’s protected role.
More recent writers have looked to the socialization of women and to their sex roles for explanations of the degree and kind of their criminal behavior (Payak, 1963; Ward et al., 1969). The feminine model that guides the socialization of women includes the attenuation of aggressive drives and the development of a moral stance that precludes overt acting out against others. Males are often rewarded by peers for resisting authority and engaging in illegal acts, whereas females are not ordinarily encouraged in such behavior. Also, the restricted sphere in which women have traditionally lived in middie-class society has provided them with less opportunity to engage in criminal behavior.
Today female crime is less rare. The ratio of male to female arrests in the United States was five to one in 1984, compared to seven to one in 1968. Even so, the sex ratio was relatively unchanged in the five years from 1979 to 1984. In 1984, for example, the percentage female of total arrests was 16.7, up only 1 percent compared to 1979’s 15.7.[51] As the data in Table 12.2 show, the percentage of female arrests increased considerably more in some crime categories than in others. While female arrests for violent crimes and for property crimes increased only 0.5 and 1.6 percent respectively, arrests for other offenses, such as embezzlement, rose more dramatically. Others have noted that most of the increase in female crime in the past decade is accounted for by increases in economic and other nonviolent crimes (Leonard, 1982).
The increase in female crime has been attributed to a variety of factors, including increased drug use, general letdown of social inhibitions, and changes in the status of women leading to increased willingness of law-enforcement officials to arrest them. One can hypothesize that as society becomes more open to women their opportunities to commit visible crimes increase, and concomitantly, as society becomes less protective of women and less patriarchal in its attitudes toward them their infractions of the law will be dealt with more stringently.
Table 12.2 Percentage of females among arrestees, 1979 and 1984{13}
| Offense category | 1979 | 1984 |
| Violent crimes | 10.2 | 10.7 |
| Murder and nonnegligent manslaughter | 13.7 | 13.3 |
| Forcible rape | 0.8 | 0.9 |
| Robbery | 7.4 | 7.2 |
| Aggravated assault | 12.4 | 13.4 |
| Property crimes | 21.8 | 23.4 |
| Burglary | 6.3 | 7.4 |
| Larceny-—theft | 30.3 | 30.2 |
| Motor vehicle theft | 8.9 | 9.2 |
| Arson | 11.3 | 12.2 |
| Other selected offenses | ||
| Forgery and counterfeiting | 30.9 | 33.7 |
| Embezzlement | 25.3 | 36.9 |
| Prostitution | 67.5 | 69.9 |
| Against family and children | 9.9 | 13.9 |
| Driving under the influence | 8.7 | 11.6 |
Inevitably, some observers have wanted to make a connection between the increase in female crime and the women’s liberation movement, arguing that the rising tide of female assertiveness has broadened women’s scope from their “traditional” crimes of prostitution and shoplifting to more serious and sophisticated crimes (Adler, 1975). Others argue that it is specious and misleading to blame the women’s movement for the increased participation of women in crime (Feinman, 1979; Leonard, 1982). These writers point out that incarcerated women tend to be poor, black, and young, hardly the constituency of the women’s movement. Far from emancipated, they are mostly victims of denied social, educational, and economic opportunities.
One study attempted to investigate a possible association between criminality and a feminist orientation by comparing attitudes of women prison inmates with those of college women. The inmates saw women as weak, emotional, and less capable than men. They thought women should be submissive and faithful to their husbands, and should not drink, curse, or smoke. The college women, on the other hand, had much more assertive and egalitarian attitudes toward women’s roles. All but two of the inmates were negative toward women’s liberation and feminist goals, while all the college women were positive (Leventhal, 1977).
Most women criminals are outside the mainstream of the women’s movement, which has attracted mostly middle-class, educated women. As Balkan and Berger (1979) point out, the movement has not addressed the circumstances of lower-class women, from whose numbers come most female offenders. The women’s movement, they say, needs to view sexual oppression in its relationship to class position. It is not a coincidence that most women in prison come from the most socially and economically oppressed classes of society.
Women in Prison
Today the federal government and most states have penal institutions for women that are separate from those for men. The ratio of male to female prisoners in these institutions in 1984 was about twenty-two to one. Though women are still only a small proportion of incarcerated persons, the number of women in prison climbed by 133 percent in the decade 1974—84, compared to an increase for men of 86 percent. A survey of state prison inmates conducted by the U.S. Census Bureau revealed that a typical woman in prison was in her twenties, never married, had at least one child, had less than a high school education, and was about equally likely to be white or black (46 to 52 percent). About a third had no prior convictions, and more than half were serving terms of five years or more. A majority were imprisoned more than one hundred miles from their homes (John, 1984).
Distance from home and the isolated settings of many prisons create problems for prisoners and their families. Alderson, the nation’s only all-woman federal prison, is in the hills of southern West Virginia, three hundred miles from the District of Columbia, where many of the women lived. “We’re the forgotten women,” said one inmate. “We’re just dropped here in these mountains and that’s it” (Preston, 1984, p. 6).
Women’s behavior when imprisoned sometimes reflects the same gender-role stereotyping that occurs in the outside world. According to one counselor at Alderson, who had come there from a male institution, “Men [inmates] are always on the phone to their lawyers, they’re always working on their cases. Women don’t call their lawyers, they call their kids or they call their man. It’s probably some man who got them in here in the first place, but they want to call him anyway” (Preston, 1984, p. 7). The woman warden of the prison agreed that hardly any of the women were “masterminds” at crime. Most, she said, come as codefendants.
The consequences of imprisonment include certain common experiences for both men and women: loss of freedom and autonomy, deprivation of goods and services, separation from family and here-to-sexual contacts, and removal from home and community to a sometimes alien and often harsh and lonely setting. For women, the disruption of family life and of significant relationships has the effect of undermining or removing their most salient social roles of wife, lover, mother, sister, daughter, and so on, roles to which their identities are tied and within which their affectional and security needs are met. To compensate, women in prison evolve an informal culture which duplicates the interactions of primary social relationships in the outside world and represents a transfer of social roles and statuses into the prison, providing a system whereby women can continue to participate in the familiar rituals of courtship, marriage, and the family (Giallombardo, 1974; 1966; Heffernan, 1972). Such social systems are found both in institutions for delinquent girls and in prisons for adult women with remarkable similarities that suggest their relevance to common needs and problems and reflect the outside social structure. The system is a network of nuclear families and other configurations linked to each other by the overlapping membership of some individuals.
Western, a correctional school for girls, is an example of an institution where an informal social system developed. It is called “chick business,” which means all the behavior related to the homosexual alliances and kinship ties formed by the inmates. Individuals are differentiated by the family roles and the sex roles they occupy, and almost all are part of the system of family groups in the institution. A newcomer becomes socialized very rapidly to the inmate culture:
Some girls are going together as soon as they come on the dorm. For others it takes two days or it could take one week or one month. It depends on what crowd you get into. Some get in the crowd real fast— if they know you on the streets, and if you’re friendly and hip (Giallombardo, 1974, p. 224).
Though only a small percentage of the inmates is committed to a homosexual role in the outside world, all but a few adopt a sex role of butch or femme during their stay at Western. The butch is supposed to take the aggressive role in the courtship, and the femme takes the passive role. In all other aspects of the roles, the relationship is patterned after the inmates’ cultural expectation of such roles in the outside world. Marriages are formalized by written documents and by a ceremony performed by a “high priest,” an older butch who is gay outside as well as inside prison.
An analysis of the scope and functions of women’s prison families estimates that between 50 and 70 percent of women in prison engage in some sort of homosexual activity, usually within the context of the family system (Williams and Fish, 1978). Butch-femme liaisons are the norm, and these have a strong economic as well as social and romantic function. The cooperation of two or more women provides the spirit and organization needed to acquire scarce or illicit items. A femme often enters into a relationship with a butch because of “his” contacts and assertive ability to supply her with wanted goods. Homosexuality is not condoned in women’s prisons, and congregation is discouraged both by regulations and by architectural design (Price, 1977).
While dominant-submissive roles in homosexual relationships are common in men’s prisons, the inmate social system does not include marriage and a kinship network (Vedder & King, 1967). The roles of violence and the enforced submission of a weaker inmate to a strong one, both characteristic of male inmate culture, do not emerge in the prisons for women. Such sex differences reflect prevalent values in the outside world. As Giallombardo pointed out, since the cultural orientation of males in our society precludes the adoption of a female role, the family systems of the female prison cannot occur. Even in prison, the confirmed homosexual is considered to have sacrificed his manhood, although the “wolf” who is aggressively homosexual as a temporary expedient is consistent with masculine norms, especially since the absence of sentiment in the relationship divests it of the feminine aura that it tends to have in society.
Rehabilitation and release
Differences exist between male and female prisons in regard to rehabilitation programs and release patterns. While prison life can have negative and dehumanizing consequences for both sexes, evidence indicates that women are discriminated against as recipients of certain kinds of services (Howard and Howard, 1974). First, the training opportunities for women in prison tend to be those which contribute to the operation of the facility, rather than preparation for potential employment. While programs for men are also limited and often unrealistic, they usually include a wider range of choices relevant to later employment. Second, work-release programs, in which the inmate works or goes to school during the day and returns to the prison at night, are less widely available to women, although they have been known to be successful in men’s institutions. Third, educational opportunities for women in prison are meager, especially for non-English-speaking inmates. Where classes did exist, they were conducted in English, and bilingual teachers were rare (Howard and Howard, 1974). Fourth, therapeutic programs \vhose aim is to reorient the offender to function in more socially acceptable ways on the outside, while rare everywhere, are more likely to be found in men’s facilities. Innovative therapeutic programs are first introduced in men’s prisons, and are tried in women’s institutions only after their success has been demonstrated with male prisoners.
Training programs for women in prison tend to be modeled on traditional social attitudes and cultural expectations for women’s roles. “In the nineteenth century it was servant-housekeeper; in the twentieth century, waitress-typist” (Feinman, 1979, p. 93). Companies have been reluctant to bring equipment and instructors into the prisons for the few eligible women, and government agencies are unwilling to allocate money for women’s programs, still apparently believing that women do not work outside the home to support their families. At Alderson most of the women cook or sew in the garment factory, practicing skills that few will use on the outside. A few women have government-sponsored apprenticeships. But the most popular program is the firefighting apprenticeship, a university-certified program that has produced the only all-woman fire department in the country. Only a very few women can participate in this program, however. At Alderson, the woman who is the warden echoed the ideology that underlies the scarcity of resources for inmates’ rehabilitation: . people want to see people punished. If you rob me or burglarize my house, 1 want something to happen to you. I don’t want to walk down the street and see you still there. And that attitude is not changing.... The average person wants to see someone incarcerated” (Preston, 1984, p. 12).
The practice of allowing conjugal visits is being introduced in some state prisons for men only (Hayner, 1972). So far, the conjugal visit is a male prerogative which women in prison do not enjoy. Also, some states allow men, but not women, to go home on furloughs if they are due to be released soon. Such differential treatment might once have been explained as necessary to avoid pregnancy in incarcerated women, but with today’s contraception this is no longer a valid argument. The implication is strong that the sexual needs of women continue to be seen as less urgent, or less important, than are the needs of men in similar circumstances.
Finally, surveys of female offenders indicate that their major concerns are their children and training and employment opportunities (Female Offender Resource Center, 1976). About 80 percent of women in prison have children for whom they are responsible. These children are living with relatives or in foster homes, and sometimes the mothers lose custody of them forever (Price, 1977). Most women in prison lack the skills to make a living wage on the outside, and prison does very little to remedy their handicap. Also, the very fact that they have been in prison makes employment upon their release problematic.
Woman as Victims: Violence and Intimidation
The reasons that women are victims of male aggression consist of complex interactions among biological, sociocultural, economic, psychological, and political influences.
-
Men are physically stronger than women are, and it is highly probable that their greater aggressiveness also has a biological basis (see Chapter 5). In our society, male socialization emphasizes this by providing training in fighting and the use of weapons and forceful intimidation as part of the experience of most small boys.
-
Our society has a long tradition of male dominance over women, and of tolerance of physical punishment and restraint of women by men. The tacit acceptance of male aggression toward women is exemplified in films, pornography, rock music, and other media whose dominant motif is the degradation of women.
-
Economic realities often force women to absorb physical abuse when they are dependent upon their aggressor. A common theme of abused wives, for example, is “If I left, I couldn’t support myself and the children, or “I had no place to go.”
-
At the level of the individual, psychological factors interact with those already mentioned to determine that some men behave in abusive ways toward women while others do not, and that some women are more vulnerable than others.
-
Common to all these is the power differential between women and men. In the interpersonal sense, power is defined as the right or ability to exercise control or to impose one’s will on another. In our society such power is vested mostly in males; and in any violent encounter between the sexes, a woman is more likely to be the victim.
In this section, we look at three kinds of victimization of women: rape, battering, and sexual harassment in work settings. Each of these has a history both of documentation and of theoretical and research attempts to understand them as intra- and interpersonal events. Feminist theorists, however, have focused attention on the nature and meaning of the act itself and have discredited older theories that often held the woman responsible for the wrong done her.
Rape
Rape is the most basic statement of woman’s subjugation by man:
... rape became not only a male prerogative, but man’s basic force against woman, the principal agent of his will and her fear. His forcible entry into her body, despite her physical protestations and struggles, became the vehicle of his victorious conquest over her being, the ultimate test of his superior strength, the triumph of his manhood (Brownmiller, 1980, p. 232).
Rape is variously defined in legal codes and in the research literature.[52] Criminal law distinguishes between forcible rape and statutory rape. Forcible rape includes the elements of vaginal penetration, force or threat of force, and nonconsent of the victim, while statutory rape is sexual relations without use of force with a person below the legal age of consent. The research literature is highly variable in its deflnitions of what constitutes rape. Feminist studies of rape sometimes define it as any sexual intimacy involving force, stressing nonconsent of the woman to the penetration of any bodily orifice by the penis or other objects, such as bottles, sticks, or fingers (Katz and Mazur, 1979).
Males are victims of homosexual rapes in about 5 percent of reported rapes, and children, both male and female, are especially vulnerable to all kinds of sexual abuse (Hursch and Selkin, 1974). Our discussion here, however, will deal with the forcible rape of women by men.
During 1984, according to the Uniform Crime Reports of the Federal Bureau of Investigation, there was an estimated total of 84,233 reported forcible rapes in the United States.[53] This means that an estimated 70 of every 100,000 women in the country were reported rape victims, an increase of 6.7 percent over 1983. Only about one-third of reported rapes result in an arrest. Arrests in 1984 were up 8.1 percent over 1983, and 17.9 percent over 1980.
FBI statistics indicate that rape is the fastest growing of the violent crimes. Even so, the actual incidence is unknown. It is estimated that between 50 and 90 percent of rapes are not reported because of the victims’ fear and embarrassment (Hilberman, 1978).
A major study of rape victimization in twenty-six large American cities provided important information on some characteristics of the crime of forcible rape (McDermott, 1979). Conducted by the Bureau of the Census for the U.S. Department of Justice, survey data consisted of interviews with representative samples of twenty-two thousand persons in each of the cities. The results thus go beyond police reports of rapes and attempted rapes and provide more representative findings on rape and its victims.
The survey data indicated that rates of rape and attempted rape in the cities are higher for young women (compared with older women), black and other minority women (compared with white women), and women who were single, divorced, or separated (compared with married or widowed women). Also, women who worked away from home and had lower family incomes were more likely to be victims than were women who were full-time housewives or women with higher family incomes.
The survey provided descriptive elements of the incident itself. Rape and rape attempts were more likely to occur during evening and nighttime hours, and more took place in public areas, such as streets and parks, than anywhere else. Usually only one offender and one victim were involved. Although weapons were used in less than half the attacks, they were effective means of intimidation; more attacks were completed when the offender was armed. Knives were the most common weapon in both the completed and attempted rapes.
This study provided important information on the controversial issue of the use of self-protective measures by the victim. Women have been variously advised to carry whistles and chemical deterrents such as mace, to scream, struggle, and fight back in any way they can. Others advise women to submit, claiming a lesser probability of injury or death. Among the women victims in the survey, about half had received physical injuries in addition to the rape or attempted rape. These ranged from bruises and cuts to knife wounds and broken bones. The relationship of the use of self-protective measures to the completion or non-completion of the rape, and to the suffering of additional injuries, was highly significant. Among victims who used self-protective measures, only 20 percent of the rapes were completed, compared with 60 percent among those who did not resist. However, the proportion of victims reporting injuries in addition to the rape or attempted rape was much greater among those who tried to defend themselves. Two-thirds of rape victims who used self-protective measures received additional injuries compared to only one-third of those who did not resist. Among attempted rape victims, about half of those who used such measures received other injuries, compared to 29 percent among those who did not resist.
These findings lend themselves to variable interpretations, depending upon how injury is defined. If the victim tries to protect herself, she increases the probability that the rape will not be completed; however, she also increases the probability that she will receive other injuries in addition to the rape or attempted rape. Since the issue is not clear-cut, it is difficult to generalize about what women should do if they are threatened with rape. Certainly women need to learn more and better ways of protecting themselves, such as courses in self-defense and in the martial arts, to give them more power in situations in which they might otherwise be victims.
Theory and research. The focus of ideology and investigation about rape has had an interesting course, ranging from blaming women to intense concern for the psychopathology of the rapist to, finally, interest in and concern for the victim (Albin, 1977).
A common motif in studies of rape has been the culpability of women. Freudian theory promoted the idea of woman’s masochistic potential for suffering, noting that sexual and reproductive events for her often combine pleasure and pain: defloration, menstruation, childbirth. Helene Deutsch, a follower of Freud’s whose work we considered in Chapter 2, thought that masochism was a normal component of the female personality, and that some women whose masochism is beyond that normal limit “are not aware of the fact that they provoke the masochistic situation or bear up with it because of—not in spite of—the suffering it brings them” (Deutsch, 1944, p. 283).
The theme of masochism supported the idea of the “born victim,” she who, because of her unconscious need to suffer, invited sexual assault by taking risks and behaving provocatively. Wives and mothers of rapists, too, have been held responsible for the rapists’ criminal acts. One study of wives of rapists suggested that they were competitive with their husbands and rejecting of their feminine role. In addition, they were unresponsive sexually, the implication being that it was prolonged sexual frustration that drove the men to rape (Palm and Abramhamsen, 1954). Mothers of rapists have been blamed for frustrating their sons’ early needs, for turning them against all women, so that women become objects for the venting of pent-up aggression fused with sexuality (McCaldon, 1967).
Another line of research on rape attempted to explain the rapist, to understand his characteristics and his psychopathology. While in earlier times, he might have been seen as a pervert and a deranged person, psychological studies of rapists during the 1960s tended to report them as the healthiest of all sex offenders, concluding, for example, that though the rapist had committed a crime from the legal point of view, on the basis of his actual sexual behavior he was not in fact a sexual deviant. “The view of rape as neither pervasion, taboo, nor serious crime against women was thus substantiated by research whose underlying assumption was precisely that view” (Albin, 1977).
Other research suggests that it is not possible to classify rapists by diagnostic categories of psychiatric disorders. Nor is it accurate to say that they are normal in the psychiatric sense. It seems that rapists occur across most diagnostic categories, as well as among nonpsychiatric populations. Asserting that their heterogeneity makes it impossible to classify them with any conviction, one study of the psychology of rapists further pointed out that their response to therapy and to rehabilitation is also highly variable. With regard to motive, however, three classes of rapists could be distinguished: those with aggressive aims, those with sexual aims, and those whose aims were a diffusion of sex and aggression. All three groups were found to have had life-long pathological relations with women, such that long prison terms would not make them less dangerous upon release (Cohen et al., 1971). Later we shall look at the feminist response to research which assumes that rape is sexually motivated, a pathological distortion of normal sexual aims toward women.
The rape victim. Studies of rape victims suggest a sequential pattern of responses, which has been called the “Rape trauma syndrome.” Immediately following the rape, the victim experiences an acute crisis reaction with feelings of fear, humiliation, guilt, and degradation. The emotional shock may disrupt normal behavior patterns. She has to cope with immediate concerns about reporting the event to the police and telling her husband or lover and family. She fears the likelihood of pregnancy or venereal disease as well as the possibility of future assault.
Later, attempts at coping lead to a “pseudo-adjustment,” in which she tries to suppress the event—“putting it out of my mind”—or has fantasies of undoing, of how she might have handled it differently. Such defenses are important attempts to protect the ego, the self, from the psychic trauma of the rape.
Gradually she feels the need to integrate the event with her selfconcept and to resolve her feelings about the rape and about her assailant. Depression is common, along with anger toward the rapist and toward herself for somehow having permitted the act to occur. (Sutherland and Scherl, 1970).
The emergence of coping and adaptive responses may take weeks, depending on such factors as the victim’s age, personality, presence of support systems, and others’ reactions. Some victims experience long-term disruptions of life styles, such as moving to another town, or impairment of their performance at work or at school. Some report nightmares, phobias, or sexual dysfunctions (Burgess and Holmstrom, 1985).
As noted before, probably a majority of rapes go unreported. A woman who has been raped is in a double-bind situation. If she chooses to remain silent, she has to deal with her trauma alone, without the support of others. She risks venereal disease and pregnancy, and the rapist will go free. Such “silent” rapes can go unresolved with long-term psychological consequences such as phobic reactions, aversion for sex, and depression (Hilberman, 1978).
If she reports-the rape to the police, she faces interrogation, the necessity to assist in the identification of the rapist, and the possibilities of courtroom exposure and publicity. She will be examined in a hospital for documentation that a rape occurred and treated to prevent venereal disease and pregnancy, as well as for any physical injuries she may have suffered. Not least, she has to face the reactions of family and friends. Will she be blamed for what happened? Will her husband or lover turn away from her? Will her children learn about it from the neighbors?
Emerging concern for the rape victim has resulted in the development of more humane methods for helping her through the postrape experience. There is greater awareness of the potential for harrassment in police interrogation, and some law enforcement agencies now require the presence of a woman officer when a rape victim is being questioned. The presence of a counselor/adovcate as part of the hospital team is now routine in many hospitals. Reports agree on the need for immediate crisis counseling for victims, to help in working through the trauma, to provide emotional support, and to deal with family and friends of the victim (Hilberman, 1978). A nationwide anti-rape movement has appeared, involving both lay persons and professionals, whose goals are to educate the public and to assist victims.
Meantime, however, the crime of rape continues to increase. Women know that no one is exempt and therefore, to some extent, all walk in fear. As one victim put it, at this encounter death is the voyeur. In the final analysis, rape is a woman’s issue.
The feminist interpretation. During the past decade, feminist theorists and researchers have strongly challenged the beliefs that rape is sexually motivated, that the rapist is a sexually deprived man who cannot control his lust. They also question the notion that women themselves precipitate the crime by seductive behavior and dress, by leading men on, the suggestion, in other words, that all women secretly want to be raped. Feminists interpret rape as an act of violence motivated by the needs for power and domination over women. Its sexual aspects are only the means for debasing and humiliating women. Rape occurs in a cultural context wherein women are viewed as inferior, as weaker, as objects to be taken and used at will.
Supporting this analysis of rape as a crime of power and dominance was a study of 133 rapists, most of whom had prior convictions and had demonstrated an escalation of use of force and brutality during their assaults. At the same time, the men were either involved in a consensual sexual relationship or had other sexual outlets. In no case were they deprived of sexual gratification. Their motives were judged to be anger or power or both. The angry rapists appeared to be expressing hatred and revenge against women, while those motivated by power needs achieved gratification and strength by asserting domination over the victim and experiencing her helplessness (Groth and Burgess, 1977).
Feminists have also responded strongly to the doctrine of victim precipitation, the belief that women “ask for it.” According to conventional mores of respectability, any suspicion of misconduct on the part of the woman meant that she got what she deserved; the man was, therefore, absolved of any crime. “The woman is placed in an impossible situation. She is responsible for her actions, his actions, his interpretation of her actions, in short, for everything that could possibly give him an excuse to lose control” (Medea and Thompson, 1974, p. 43). Men, however, are responsible for controlling their own behavior.
To all such arguments of woman’s culpability, feminists stress that rape is a violation of basic human rights. A woman’s body is her own property, and no one should have sexual access to it without her consent no matter what the provocation (Katz and Mazur, 1979).
Battering
The battering of women by the men they live with is one of the most frequent and least understood forms of violence against women. Battering is variously defined in the literature, but usually it means physical abuse that involves deliberate, severe, and repeated physical injury (Moore, 1979). Such abuse is often accompanied by psychological damage inflicted by fear, guilt, and harassment, though physical battering is the key element.
Wife-beating began to capture the attention of researchers and professional service providers in the 1970s, as part of the renaissance of feminism. The feminist “discovery” of violence against women encouraged analysis of the problem from the social context of male supremacy in a patriarchal society, rather than from the genderneutral perspective of earlier family violence researchers (Breines and Gordon, 1983). The battering of women by men has come to be seen not as a quasi-normal, if not trivial, type of family interaction, but as a phenomenon that is profoundly symptomatic of traditional societal relations between males and females.
Battering can occur in a variety of contexts, and not all the victims are married women. Men are sometimes beaten by women, and children are especially vulnerable to all kinds of abuse. Some battered women are not married to their batterers, though battered wives are the subjects of most of the studies. In this section we shall confine our interest to women who are the victims of violence by men with whom they are married or cohabiting.
Incidence. It has been observed that battering is the most underreported crime in America (Moore, 1979). Accurate data are unavailable because agencies and private individuals, such as physicians, who may come into contact with beaten women often do not record or report the event. Victims themselves frequently do not report beatings, even when they have been occurring for months or years (Martin, 1979). Available data include scattered accounts from various communities. For example, in two Michigan counties 35 percent and 42 percent respectively of all assault complaints were wife assault. In 1976 the Brooklyn Legal Services reported that 57 percent of the women filing for divorce had complained of physical abuse for at least four years before filing the suit (Moore, 1979).
A nationwide study of domestic violence revealed that 28 percent of all families in the population had experienced at least one incident of physical assault during 1975. One study estimates that one out of every two women will experience some form of violence in their lives (Walker, 1979). There is other compelling evidence of the pervasiveness of the crime. “Whenever a shelter for battered women is established, whether it be in an urban area or a rural area, it is filled to capacity immediately and there is a long waiting list” (Martin, 1979, p. 39).
The historical setting. Wife-beating has been a feature of marriage throughout most of human history, a vivid testimony to the consequences of the status and power differences between men and women. An important reason for this lies in the origin and history of marriage as an institution. Although the question of the origin of marriage has stimulated several theories, the most influential today is the concept of ubiquitous patriarchy, in which the formal institution of marriage arose from the reciprocal exchange of women among tribal groups (Lévi-Strauss, 1969). The universally observed incest taboo served to promote exogamy, marriage outside one’s own kinship system. The functional value of exogamy was the formation of alliances between groups through the elaboration of kinship systems. These alliances were based on the reciprocal exchange of property, which included women. Thus the giving away of sisters and daughters became an insurance against extinction.
With the advent of civilization, the identification of woman as property—first of her father then of her husband—acquired legal status, and wife-beating became legally sanctioned. English common law, the foundation for the American legal system, gave husbands the right to physically punish their wives. The so-called “rule of thumb” originally referred to the right of the husband to beat his wife with a stick no bigger than the thumb. It was not until the end of the nineteenth century in this country that the courts began deciding that husbands did not have a right to beat their wives. Even so, rulings were often ambiguous, advocating an attitude of noninterference in family disputes.
the husband has no right to chastise his wife, under any circumstances ... [however] if no permanent injury has been inflicted,.nor malice, cruelty, nor dangerous violence shown by the husband, it is better to draw the curtain, shut out the public gaze, and leave the parties to forget and forgive (Calvert, 1975, p. 88–89).
Obviously interpretations of what constitutes malice, cruelty, and dangerous violence can vary widely. This, along with the notions that husbands have certain rights over their wives’ persons and that what happens within domestic walls are private matters, has led to a notable reticence on the part of law enforcement agencies to get involved in these most intimate violent encounters (Martin, 1979).
The fact that a man and a woman are legally united in the bonds of marriage seems to influence whether or not violence will occur. A study of forty violent families who had come to the attention of social agencies or the police found that in only one had physical assault occurred before the vows were exchanged. In two families the wives married, divorced, and remarried the same man, and violence occurred only during the time they were legally married (Gelles, 1974, p. 153). Two possible explanations were advanced for this: one, that marital violence is considered normative in that it is not permissible to hit the same person outside the bounds of marriage; and two, that violence between two persons involved in an intimate relationship is likely only in the context of family life, with its stress and frustrations (Gelles, 1974).
Contemporary factors in battering. In battering as in other phenomena of human behavior, one finds several factors that are determining influences on its occurrence: socio-historical effects, the criminal justice system, and personal-psychological factors.
Historical precedents for man-woman relationships are reflected in today’s attitudes, beliefs, and socialization practices. Traditional attitudes toward women view them as lesser persons in the society, and this is reinforced by the tradition of their dependence on men. Thus, under certain conditions women, along with other powerless groups, are natural scapegoats for the venting of anger and frustration. One study of battered women found that 80 percent were raised with very traditional sex-role expectations. Whereas their husbands had been abused as children, most of the women had not. Rather, they had been treated stereotypically as “daddy’s little girl.” This underlines the importance of traditional role training in determining the power differential between men and women, which sets up the context in which battering can occur. As girls they had learned to be compliant and passive, to submit to punishment in the name of love. When they married men who had learned that violence inflicted by the stronger upon the weaker is an acceptable way of resolving disputes, the stage was set for an abusive relationship (Walker, 1979). In addition, the traditional economic dependence of women upon men further limits a woman’s range of options should her marriage encounter problems. In fact, one study of battered wives in Texas found that their economic dependence dominated all other reasons why they stayed with their abusive husbands. Interviewed in the shelter where they had sought refuge, 85 percent of those whose husbands were their sole source of income planned to return to them, .while 82 percent of those who had other sources of income intended to leave their marriages (Aguirre, 1985).
Regarding battering, the criminal justice system has been generally unresponsive (Paterson, 1979). This is a reflection of societal attitudes that did not view the abuse of wives as a criminal matter: “Police departments across the country have typically viewed domestic violence as a social problem and not as criminal conduct” (Paterson, 1979, p. 82). The attitude of noninterference in domestic violence has given implicit sanction to men who abuse their wives. Police have tended to avoid arrests in domestic-violence cases, and to refer battered wives to social agencies—a curious response to assaults. An additional factor in the noninterference model of handling family disputes may be the observation from FBI data that one-fifth of all policemen killed in the line of duty die as a result of their investigation of a domestic argument.
Profiles of batterers. Who are these individuals who batter women? Are they responding to their own personal histories, personality problems, or learned modes of conflict resolution? Men who batter women are not distinguished by age, educational level, religion, socioeconomic status, psychopathology, or ethnic group. Rather they are representative of men in general, though there are some commonalities in their backgrounds and personalities that are related to their abusive behavior. Most were raised in families where violence was commonplace, where they saw their mothers abused, and where they themselves were physically mistreated. They learned that violence, for punishment, for the imposition of one’s will upon another, for scapegoating, or simply for an outlet for frustration, is an acceptable form of conflict resolution.
An important characteristic of batterers is low self-esteem (Moore, 1979). A husband, socialized to believe in the masculine stereotype, may feel that he is not getting ahead fast enough, that he is not providing adequately for his family. He may feel insignificant at work, impotent in the outside world, a failure. Thus, abuse of those weaker than he becomes a defense against his knowledge of his own powerlessness. In addition, it has been shown that family violence is more frequent when the husband’s educational and occupational levels are lower than those of the wife (Gelles, 1974). This is further evidence indicating the importance of low self-esteem in the abusive man’s profile. A threat to the traditional male’s view of himself as superior in attainment to his wife contributes largely to the phenomenon of wife-beating.
Alcohol has been implicated in about 60 percent of spouse-abuse cases (Moore, 1979). Given the disinhibiting effect of alcohol on behavior, its use can readily be a precipitating factor in a person who is experiencing stress, who has a low tolerance for frustration, and who needs to assert himself as the dominant one.
Thus to the question, Why does battering occur? there is no simple answer. As with most other types of human behavior, the individual act is determined by the confluence of several factors, whose importance is variable from one person to another. Battering of women is a function of intrapersonal, familial, social, legal, and historical situations, influences, and events, and their effects upon vulnerable persons.
Battered women. The battered woman, like her batterer, may be any age and from any educational and socioeconomical level. Less affluent women tend to be overrepresented in the statistics, since more affluent women are likely to have more resources. Affluent women may seek professional help, for example, rather than having to depend on assistance from the police or social agencies. Even so, wife abuse occurs at all levels of the society. An organization that has provided shelter for thousands of battered women reported that their typical client is thirty-six years old, has been married seventeen years, and has four children. She has had little or no job experience and arrives at the shelter with her self-esteem and self-confidence undermined. She is in a state of fear and self-doubt, mistrusting her own decisions (Bell, 1977).
Women with a history of being abused tend to lead very constricted and isolated lives. Often they have withdrawn from friends and family because of their feelings of shame and guilt. Some think the beatings are their fault, that they provoked them by their own behavior. That is, often the woman believes the reasons her husband or boyfriend puts forth in order to rationalize his violent behavior. Thus, if he beats her “because dinner was late,” she may well believe that if dinner had been on time, the incident would not have occurred. Beating victims “have a terrible sense of insecurity. They’re afraid to be alone ... and the empty, passive feeling of these women is reinforced in marriage to a man who keeps telling them that they don’t know anything” (Bell, 1977, p. 22).
The observation that many abused women continue to live with their husbands for many years before actively seeking help or getting out has contributed to the idea that women want or expect to be mistreated, an echo of the old theme of women’s inherent massochism. Otherwise, goes the question, why does she stay? This is not a trivial question, as its answers increase the spectrum of observation to include not only the victim but the social context as well.
There are various reasons why women put up with repeated beatings by their husbands (Bell, 1977).
-
Negative self-image. Such women feel they have nothing to offer to another person. Their self-worth hinges on having a man, and the idea of being alone signifies worthlessness and abandonment. The sense of powerlessness coming from the reality of the situation engenders feelings of hopelessness and inability to see alternatives. They feel trapped in their situations.
-
Belief that their husbands will reform. Some women continue to believe that their husbands are basically kind and good, that they are responding to transient stresses, that they will be “themselves” when times get better. Such women report that they love their husbands—and perhaps, too, they cling to the myth of the family as a place of safety and love. Such defenses deny the reality of their lives and make it possible for them to stay in the hope that things will get better.
-
Economic hardship. As noted above, a typical beating victim has no training or experience in earning a living. Often with dependent children, the woman sees no way to survive economically without her husband. This is probably the most realistic of the reasons women stay in abusive relationships.
-
Need for child support. If a woman charges her husband with abuse, it may impair his earning capacity. A professional man may be hurt by the publicity, a worker by absence from the job, in which case the chances of collecting child support are diminished. Too, many fear their husbands will retaliate for their leaving by Ending a way to avoid making child support payments.
-
Doubt that they can survive alone in a hostile world. As one woman poignantly put it, “... if the person who loves you treats you like that, what is the rest of the world going to do to you?”
-
Finally, a woman may stay in an abusive relationship because of fear of violent retaliation should she leave. She fears that her spouse or boyfriend will subject her to even greater violence for deserting him, or reporting him to the police.
Instead of labeling battered women masochistic collaborators in their own abuse, we need to understand better the social and economic realities of women’s lives, the nature of the institution of marriage, and the society in which it exists.
Coping with women battering: solutions and more problems. Now that battering is recognized as a widespread and serious problem in our society, what can be done about it? Attempts at solving the problem are underway on several fronts, including temporary expedients for the protection of victims, legal courses of action, and preventive measures aimed at education and socialization.
In the past ten years, shelters for battered women have opened their doors all over the country. Typically such shelters take in battered women and their children, providing them with a safe place to stay while their needs are assessed, their alternatives explored through counseling, and their temporary crises resolved through available social service and other resources. In the beginning shelters were operated by volunteers and supported by donations and contributions from the community; now they are being funded by public agencies and by state and local governments. Shelter networks exist, whereby women can be transported from one state to another for their protection.
Shelters are not a panacea however. There are still too few of them to meet the need, and existing ones are usually full. Shelters at best are temporary expedients, to meet the need of the woman and her children for immediate protection, and to help her develop alternative plans for managing her life. Women who come to shelters have multiple problems, both situational and psychological, which they still must face in addition to terminating the abusive relationship. Specifically, with or without the support and services of a shelter, a woman often must seek a new means of support, such as getting on welfare or finding a job, she must And a new residence, and even then her physical safety is not insured, and often she must obtain childcare if her children are still young.
The legal system is changing its approach to the problem of wife-beating and to its victims. In some states, wife-beating is now a felony offense. Numerous civil remedies now exist for alleviating the distress of victims and for providing protection for them. For example, Florida has a domestic violence law which funds existing shelters with increased revenues from marriage license fees. The intent is to match community support for shelters, and to insure continuous operations. Many states have passed bills creating networks of community shelters for abused women and children.
Women in New York and California won class action lawsuits against police departments, after charging them with not being responsive to calls from battered women. As a result, these departments have agreed to make basic changes in their handling of such situations and to treat batterers by the same criteria that apply to other assault cases (Paterson, 1979). In addition, a new breed of police officer, trained to deal with domestic violence, is coming out of college and university training programs (Bell, 1977).
Psychology itself has been instrumental in creating new public policy for dealing with domestic violence. Much of this has developed from cases in which abused women have killed their abusers. In the past, such women have been treated harshly by the courts, who did not see their abuse as a factor, or found innocent on the grounds of insanity. Today such women may plead innocent on the grounds of self-defense. In these instances, psychologists may testify as to the psychology of battering relationships, thereby assisting such women in getting a fair trial by educating jurors and the court about the context of battering and the defendant’s perceived need to use self-defense (Walker, 1984).
The first recorded case wherein a battered woman who killed her husband pleaded that she had acted in self-defense was tried in 1977. A psychologist had evaluated the woman, found that she was indeed a battered wife, and testified to the jury why she had shot and killed her husband:
The members of the jury were allowed to listen to the expert describe the violence in their relationship and explain why Miriam Grieg was psychologically unable to leave the marriage, why she was able to recognize that the violence that night was life-threatening, and how the battering syndrome affected her state of rnind at the time she shot him. They then came to a unanimous decision that Miriam Grieg had killed her husband in self-defense (Walker, 1984, p. 1179).
In the long run, basic solutions will need to rely on education of the public and on changes in the primary ways that men and women relate to each other. Socialization practices still sanction the greater aggressiveness of males, and the notions of male dominance and female submission. Aggression is learned in family and social contexts and can, likewise, be unlearned as the contexts change (Eron, 1980). Traditional marriage has an inherent unequal distribution of power between man and woman, which facilitates an abuse of that power. As marriages become partnerships of equals, and as women become more independent of men, both economically and emotionally, we can hope to see a decrease in the physical abuse of women by their husbands.
Sexual harassment
Like rape and battering, the sexual harassment of women in work, educational, and other settings goes largely unreported. While less violent than the two other offenses, it is clearly an intimidation of women and is both degrading and exploitative. Again, it occurs within the context of a power differential between a man and a woman, wherein important needs of hers can only be met through his influence or approval.
The typical case of sexual harassment occurs between a man of some authority and a woman who is subordinate to him. He suggests, either directly or by innuendo, that she will be rewarded in the job setting if she accepts his sexual advances and that she will be punished if she does not. “Sexual harassment can range from verbal abuse to actual rape. It includes sexual suggestions or jokes, that “friendly” pat on a woman’s behind, an “accidental” brush against her body” (Goldstein, 1980). Surveys show that eight out of ten of all working women have some experience with sexual harassment during their employment careers.
In one case, a young woman employee of a radio station told of repeated episodes of unwanted touching, being chased into the restroom, and physical coercion almost to the point of rape. When asked why she subjected herself to this, she said, . 1 thought in a Hash about my whole career, my credibility vanishing. I knew he was a man of wealth, and I thought that everything I’d worked for would be destroyed....” (Goldstein, 1980, p. 7).
Such cases, only whispered about in the past, are now being publicly aired in the courts. A reason for this is that hiring a woman for a job with the consideration that she will provide sexual services is now illegal under Title VII of the Civil Rights Act of 1964.[54] Also, the Equal Employment Opportunity Commission has ruled that sexual harassment on the job is illegal, making employers and unions responsible for such acts by employees.[55]
Sexual harassment of women by men occurs not only between employer and employee but also between professor and student, and doctor and patient—in any relationship wherein power is vested in the male, and the lesser status of the female plus the sexual potential of her body result in her victimization.
Women students not infrequently are targets of sexual harassment by male professors. The nature of the offense can range from “put-down” jokes and derogatory remarks about women in the context of classroom activities to solicitation for sexual favors in exchange for high grades. One woman student wrote an account of her experience in a political science course at a large state university.
This professor made sexist and derogatory comments about the women in the class, women in public life, women in general:
‘You women are going to waste your education raising babies.’
‘There is no future for women in political science. I don’t believe in women in government at all.’
‘Now if Justice Marshall had been a woman he would have sat down and cried, which is the reason—and a good one—we don’t have women on the Supreme Court.’
‘Any husband who is foolish enough to listen to what his wife says politically deserves anything he gets.’
I discussed with him the fact that his remarks were at first irritating and then progressively more offensive. 1 said that some of the women in the class felt intimidated and put down. The point is that if I, with all kinds of positive reinforcement from women professors and feminist friends, was brought down in spirit by this man, then surely so are other women students (Personal communication).
In another case, a graduate student in psychology reported being repeatedly pressured by her major professor to have sex with him. Such a situation is particularly precarious because the professor almost literally holds the student’s future career in his hands.
While many women in academia deal with the problem on an individual and private basis, some are taking action both to publicize the problem and to protect themselves. Workshops in university settings bring the issues into the open, so that institutions are forced to acknowledge that the problem exists. In 1978 a prestigious Eastern university, once all male, was sued by five women students who charged that its refusal to institute mechanisms and procedures to address complaints and make investigations of sexual harassment constituted violation of Title IX of the Education Act Amendments, thereby denying equal opportunity in education. Though the judge allowed the case of only one of the women to be tried on its merits, this was hailed as a victory because it recognized sexual harassment of students as a possible Title IX violation (Spokeswoman, April 15, 1978).
Although there are now legal remedies, the problem of sexual harassment is by no means solved. Unlike rape and battering, which leave physical evidence of their occurrence, sexual harassment may be hard to prove. Usually it involves the word of one person against another, with the alleged offender having the greater power. And if harassment is proven, what then? For women who are vulnerable, the consequences of making an issue may be onerous in themselves—ridicule, getting a reputation as a troublemaker, possible loss of job. Even so, the efforts of women have resulted in public acknowledgment of the problem, which can in itself act as a deterrent.
The Pornography Issue
Pornography is defined as “obscene literature, art, or photography, especially that having little or no artistic merit.” The word is derived from the Greek pronographios, which means “writing about harlots.”[56] Thus from earliest times the word pornography has implied the depiction of the sexual use of women as objects. In the past few decades, the production and distribution of pornographic materials has become a multibillion-dollar industry of international dimensions (Longino, 1980).
Until recently public attitudes toward pornography were organized around two viewpoints. The traditional view was that pornography was immoral and should be condemned because it portrayed sexually explicit material and was designed to appeal solely to “prurient interests,” that is, to arouse sexual feelings. This view was linked directly to the belief that sex was a private matter between husband and wife, to be practiced for procreation only, and that any stimulus to the arousal and gratification of gratuitous lust for its own sake was therefore to be condemned. In other words, it was the sexual content of pornography that made it morally objectionable.
The other prevailing viewpoint toward pornography, emerging publicly in the permissive climate of the 1960s, was that pornography was a variant of expressions of sexuality, that it was not harmful or wrong, that it could in fact have a liberating effect by helping people rid themselves of sexual repressions and “hang-ups” and feel freer to experiment and thereby enjoy their sexuality.
This latter viewpoint was reinforced by the publication in 1970 of the report of the U.S. government Commission on Obscenity and Pornography.[57] The commission, composed mostly of social scientists, agreed that pornography involved “the degrading and demeaning portrayal of the role and status of the human female ... as a mere sexual object to be exploited and manipulated sexually” (p. 239). Even so, the commission concluded that exposure to pornography does not promote antisocial behavior and can even help to develop more open communication in marital relationships.
Thus the wisdom of the 1970s was that pornography had sexuality as its essential element and that its effect was benign, if not actually therapeutic, in promoting the equation between sexual freedom and the good life: “Since free and unfettered sexual expression is valorized as a force leading to human liberation, liberals have associated pornography with the progressive and the good” (Diamond, 1980, p. 687). ”
As the women’s movement began to gather power in the early 1970s, however, a third viewpoint on pornography began to be heard. Feminists such as Kate Millett (1971), Robin Morgan (1977), and Susan Brownmiller (1975) scathingly attacked the liberal interpretation of pornography as essentially harmless and, at its best, an antidote to repressive sexual morality. Instead, they said, pornography features male dominance and female subjugation. Not only sexist and misogynistic, it depicts women being subjected to the most brutal and dehumanizing violence, “dramatized rapings, stabbings, burnings, beatings, torture, dismemberments, mutilations, and deaths in the name of male sexual pleasure or sheer entertainment” (Lederer, 1980, p. 16). Susan Brownmiller (1975), in her history of rape, Against Our Will, called pornography “the undiluted essence of anti-female propaganda” (p. 394) and connected its basic meaning to that of rape. Pornography, said the feminist critique, was not about sex at all, but, like rape, was about woman hatred, expressed by the sadistic display of power and violence to bring about the subjugation of the woman victim.
In some of the less sadistic material, women are portrayed as enjoying their humiliating and painful treatment: “... women are portrayed as turned on and sexually satisfied by doing anything and everything men order them to do, and what this involves is for the most part totally contrary to what we know about female sexuality; that is, it is almost totally penis-oriented, often devoid of “foreplay,” tenderness, or caring, to say nothing of love and romance. In short, • • . a celebration of male power over women and the sexist wish that women’s sexuality and values be totally subservient to men’s” (Russell, 1980, p. 27). It is worthy to note here that the theme of women’s enjoyment of the masochistic role in pornography echoes the traditional commentary that women provoke and invite their own rapes and that battered wives who stay with their husbands derive some gratification from their own” suffering.
Fears have been expressed that the ready availability of pornography with its blatant display of antiwoman violence has the effect of promoting and legitimizing rape and other forms of violence against women. By contrast, the liberal view has held that the use of pornography by men acts as a “safety-valve,” thus draining off violent tendencies. This was the view favored by the pornography commission, though the commission did not deny that a causal connection between pornography and rape exists. A case in point is the Denmark experience. Beginning in the 1960s, the Danes removed legal restrictions on pornography, and early statistics indicated that “sex crimes” took a downward turn. More recent data, however, indicate that the incidence of rape increased considerably in the 1970s, rising to the highest level yet experienced (Diamond, 1980).
Feminist response to pornography has been active and vocal. In 1976, a feminist group staged a demonstration and press conference in Los Angeles to express their outrage at a billboard of a chained woman covered with bruises, with a caption saying “I’m black and blue from the Rolling Stones and I love it.” The advertisement was removed. In 1977, women damaged a theater in Rochester, New York, where a pornographic movie named Snuff was showing. This film allegedly showed the actual torture, mutilation, and murder of a woman, solely for sexual stimulation. In 1978, in San Francisco, an organization called Women Against Violence in Pornography and Media held a national conference called “Feminist Perspectives on Pornography.” Over five thousand women participated in a “Take Back the Night” march through the city’s pornography district.
Many feminists theorize that the tremendous proliferation of violent pornography in recent years is a backlash effect of the women’s movement and of feminism itself. Since pornography partakes of the patriarchal value of the systematic domination of women by men, it serves a political purpose. Therefore, any threat to male power over women would be expected to result in an increase in its intensity and violence: “Enough women have been rejecting the traditional role of subordination to men to cause a crisis in the collective male ego. Pornography is a male fantasy-solution ...” (Russell, 1980, pp. 27—28). It has been suggested too that as women have become stronger and more assertive, some men And it easier to manifest their power over younger and younger people, thus accounting in part for the enormous growth of the market for child pornography in recent years (Russell, 1980).
The feminist response to pornography took a new, and to some, an ominous turn in the 1980s. American feminists began to polarize around two different perceptions of feminist sexuality. One group, radical feminists who reject male-dominated heterosexual sex, believe that the sexual practices of a patriarchal society stimulate violence against women. They condemn pornography, as well as sadomasochism, prostitution, adult/child sex, and sexual role-playing, as in butch/femme relationships. They reject these because of the dominant/subordinate power relations with which each is invested.
The other group, termed libertarian feminists, support any sort of sexual practice between consenting partners that gives pleasure, including pornography, sadomasochism, adult/child sex, and role-defined sex. They view the radical feminists as moral conservatives who want to focus on the dangerous aspects of sexuality in contrast to their own focus on pleasure.
In regard to pornography, the conflict seems to stem in part out of conflicting assumptions as to what is pornographic. Much erotica, for example, is infused with the ideology of romantic love between partners with equal rights to the sexual pleasure of their relationship. And erotic art has a long cultural history that does not necessarily depend on male dominance or reflect patriarchal values (see, e.g., Eitner, 1975). But it is also the case that much sexually explicit material carries the message of sexual arousal of men by depiction of violence against women (Ferguson, 1984).
Since the radical feminists basically repudiate heterosexual relations, and the libertarian feminists adopt a prosex position that includes acceptance of some behaviors that are unacceptable to mainstream attitudes about sexuality, neither camp provides a comfortable sexual milieu for most women. A possible resolution toward a feminist sexual morality would include the development of feminist erotica and sex education that would encourage new forms of feminist fantasy production, aimed at all types of audiences. This could have the effect of cutting into conventional pornography and bringing feminist sexual values that do not depend on male domination and violence into the public consciousness (Ferguson, 1984).
The victimization of women is by no means confined to acts of rape, battering, sexual harassment and pornography. These are only among the most blatant examples of intimidation and the abuse of power in. male-female relations. Feminist analysis during the past decade has been instrumental in provoking re-examination of old theories and attitudes that saw the victim as provocateur. Such acts are now seen as arising from social patterns and traditions, long taken for granted, wherein the subordination of women is the basic fact that underlies all of them. There is no more important fact in the study of the psychology of women.
Mental and Emotional Disorders of Women
Historically people who behave in strange, unpredictable, “mad” ways have been perceived as threats and have been variously punished, segregated, and “treated.” Until fairly recent times, such persons were thought to be responsible for their misery, which they had brought upon themselves by their own wickedness. Thus to the punishment by God was added the punishment by man, and floggings, torture, and murder were common (Zilboorg and Henry, 1941). The notion that such disturbed persons were sick rather than sinful is credited to Philippe Pinel, an eighteenth-century French physician who thought that the revolutionary slogan “Liberty, Equality, and Fraternity” should apply also to the inmates of asylums and persuaded the government to take steps to alleviate their miserable conditions.
Although the change in attitude toward such disorders was certainly an improvement, it became fashionable to label as “sick” all kinds of troublesome behavior from marital infidelity to bed-wetting. This overinclusiveness of the “sickness” concept has caused it to lose credibility among some theorists and students of human behavior, who have advised its abandonment altogether. Thomas Szasz, for instance, has been highly critical of his profession of psychiatry and its treatment of patients, which he has characterized as unethical and oppressive (1961). He has questioned the very existence of mental illness, and compared the examination, diagnosing, and treatment of mental patients to the inquisition, testing, and exorcism rituals practiced on witches by priests of earlier time (Szasz, 1970).
Concepts of mental health or mental illness vary considerably among professionals in our own society, and we have already seen that judgments about what is normal are subject to very different standards in different cultures. Questions such as, “What is normal,” and “Who is mentally healthy,” ask for definitions of values which cannot be supplied by empirical science. It is said that when Freud was asked what ought a normal person be able to do, he replied, “Arbeiten und lieben” (to work and to love). Most contemporary theories likewise include in their definitions of mental health effective mental and physical functioning and the ability to form satisfying interpersonal relationships. But even these reflect our Western value judgments of the good life. In 1937, Karen Horney pointed out the effect of cultural relativity: “With us a person would be neurotic or psychotic who talked by the hour with his deceased grandfather, whereas such communication with ancestors is a recognized pattern in some Indian tribes” (p. 15).
In our society, mental disorders are typically diagnosed in accordance with the classification system devised by the American Psychiatric Association and presented as the Diagnostic and Statistical Manual of Mental Disorders (DSM III, 1980).
Examples of mental disorders in this system include several important categories wherein women differ from men: affective disorders, anxiety disorders, somatoform disorders, personality disorders, substance use disorders, and eating disorders. A detailed description of psychiatric diagnoses is beyond our scope, but these selected categories will be defined briefly for purposes of the subsequent discussion.
Affective disorders include various types of mood disturbances such as manic or depressive episodes. Dysthymic disorder, or depressive neurosis (depression), is one of the most common of psychiatric diagnoses. Typical symptoms of depression include chronic tiredness, feelings of inadequacy and low self-esteem, decreased productivity, social withdrawal, loss of interest in pleasurable activities, pessimistic attitude, tearfulness, and thoughts of suicide. Symptoms may vary in intensity and duration, such that some depressed persons may function adequately and never seek treatment, while others may be incapacitated and suicidal.
Anxiety disorders include phobias and anxiety states. Common phobias are agoraphobia, a strong fear of being in public places such as streets, stores, buses, or crowded areas; and social phobia, a persistent fear and avoidance of situations in which the individual is exposed to scrutiny by others and fears acting in ways that will bring about humiliation and embarrassment. Anxiety states include panic disorder, severe panic attacks for no apparent reason, with such symptoms as palpitations, trembling, faintness, and fear of loss of control; and post-traumatic stress disorder, in which an individual who has experienced a severe stressor, such as a life-threatening assault or a natural catastrophe, has episodes of reexperiencing the event and other symptoms such as feelings of detachment from others, sleep disturbances, impaired memory, and avoidance of activities that arouse recollection of the traumatic event.
Somatoform disorders are those in which a person complains of physical symptoms that are not explained by physical disorder or injury and are not side effects of drugs or medications. They include somatization disorder, in which the patient has many vague symptoms (a minimum of fourteen for women, twelve for men) that may involve any or all of the bodily systems; and psychogenic pain disorder, in which the patient complains of severe pain for which no organic pathology can be found and because of which there is some gain for the patient, such as avoidance of a noxious activity, or receiving support from others that he or she might otherwise not get.
Personality disorders describe basic personality patterns that are maladaptive for the individual or for society. Some commonly diagnosed personality disorders are paranoid, with pervasive suspiciousness, hypersensitivity, and restricted range of feeling; histronic, with self-dramatizing, overreacting behavior and perception by others as shallow, vain, and manipulative; antisocial, with early onset and continued pattern of such behaviors as inability to sustain effective work or parenting activities, repeated encounters with the law, no enduring interpersonal attachments, repeated fights, irresponsibility in finances and planning for goals, lying, and recklessness; compulsive, with restricted ability to express feelings, perfectionism, excessive devotion to work at the expense of relationships, indecisiveness, with inordinate worrying about making mistakes or setting priorities; dependent, with excessive reliance on others, subordination of own needs to those of important other to avoid having to rely on self, lack of self-confidence, vision of self as helpless and stupid; and borderline, with impulsivity, unstable relationships, inappropriate anger, identity disturbance, mood shifts, physically self-damaging acts, and chronic feelings of emptiness or boredom.
Substance use disorders are those in which a person has a pattern of pathological use of alcohol, barbiturates, cocaine, or other drugs such that he or she experiences impairment in social or occupational functioning. The pattern of pathological use may include inability to cut down or stop using the substance, repeated efforts to gain control of usage, daily intoxication, and physical effects of overdose. Impairment of function may include loss of job, loss of friends, fights, accidents, and legal difficulties.
Eating disorders are usually manifested in adolescence and young adulthood. Widely publicized in recent years, they include anorexia nervosa and bulimia. Anorexia nervosa is characterized by an intense fear of becoming obese, with disturbed body image (i.e., perceiving oneself as fat when one is actually thin), severe weight loss by excessive dieting, and refusal to maintain normal body weight. Bulimia includes recurrent episodes of binge eating terminated by self-induced vomiting and repeated attempts to lose weight by restrictive diets, vomiting, or use of cathartics and diuretics. The bulimic patient is aware that her eating pattern is abnormal and fears that she cannot control it. She has feelings of depression and low self-esteem after binging.
These are only a few of the categories of mental disorders that are described in the DSM III. They are included here because they are prominent among those in which gender differences appear; thus they have particular relevance to the psychology of women.
Gender and mental disorders
Earlier we noted the dichotomy that occurs after childhood in the classification and treatment of problem behavior, and how some behaviors come to be seen as criminal and others as symptoms of mental illness. We have already seen that the behavior of women compared to men is infrequently seen as criminal. In the area of mental disorder a differing picture emerges: women are overrepresented among the help-seekers, and their diagnoses and treatment are different from those of men.
It is not a simple matter to assess accurately the incidence of mental and emotional problems in a population, since many persons do not seek treatment, and diagnostic information for those who do may go unrecorded in some cases or may be inaccurate or imprecise in others owing to varying interpretations of patients’ syndromes by different practitioners in different treatment settings. Available data, however, show that in our society more women than men are treated for mental disorders (Russo, 1985). In 1977, for example, 5.6 percent of females of all ages, compared to 3.5 percent of males of all ages, visited health care services for treatment of a mental health-related problem (Horgan, 1982). Data from a 1980 national sample of patients of psychologists’ and psychiatrists’ office practices revealed that 59.5 percent were females, compared to 40.5 percent for males (Taube et al., 1984).
A study of psychologists in private practice in the southeastern United States found that the greatest percent of the primary clientele of both male and female clinicians consisted of individual female clients, 37.5 percent and 41.4 percent respectively. Less than 1 percent of the clients of female clinicians, and 12.6 percent of the clients of male clinicians, were individual males (Pendergrass, 1974).
Finally, one other interesting finding relates a sex difference to the incidence of mental disorders among the intellectually gifted. The Terman longitudinal study of gifted children (see Chapter 6) found that as children, the boys had a higher incidence of nervous disorders than the girls. But as adults the rate of psychosis among women was higher than the expectancy rate in the general population, while the rate for men was lower.
Table 12.3 Mental disorders with unequal distribution for women and men{14}
| More common for women | More common for men |
|
Affective disorders Major depression Cyclothymic disorder Dysthymic disorder Anxiety disorders Agoraphobia Social phobia Panic disorder Somatoform disorders Somatization Psychogenic pain Personality disorders Histrionic personality disorder Borderline personality disorder Dependent personality disorder Eating disorders Anorexia nervosa Bulimia Multiple personality Psychosexual disorders Inhibited sexual desire Inhibited orgasm |
Substance use disorders Alcohol hallucinosis Impulse control disorders (e.g., kleptomania, pyromania) Factitious disorders (voluntary production of physical or psychological symptoms to gain “patient” role) Personality disorders Antisocial personality disorder Paranoid personality disorder Compulsive personality disorder Psychosexual disorders Transsexualism Paraphilias (e.g., fetishism, pedophilia, sexual sadism, and masochism) |
The DSM III provides information on gender differences in incidence of those mental disorders where such data exist. Table 12.3 presents some disorders that are more commonly diagnosed in one sex than in the other.
Inspection of the gender-linked categories of mental disorders shown in Table 12.3 suggests some patterns of male and female adaptations with which we are already familiar. Depression, fearfulness, and somatization reflect internalization of conflicts, compared to male bias toward substance abuse, impulsivity, and antisocial acting-out behaviors. Histrionic and dependent personality disorders present configurations that are exaggerations or caricatures of traditional notions of femininity. Eating disorders reflect, among other things, a pathological concern with body image. Those psychosexual disorders more common among women are characterized by inhibition of sexual response, whereas those that are more common among men include asocial aims as well as antisocial, hurtful acting out against others. The implication is that when women and men become mentally ill, the forms that their disorders take are to some extent significantly influenced by adaptations that their minds and bodies have already made to the sociocultural conditions of being female and male in our society.
All these data show that women have higher rates of mental disorder in several important categories than men do. When the data are examined by marital status, however, a somewhat different picture emerges. Studies which report marital status of mental patients agree that single, divorced, and widowed women have fewer mental problems than men in the same categories (Russo, 1985; Gove, 1980). Therefore it is the population of married women which accounts for the surplus of women among the mentally ill. The shift from being married to being divorced or widowed has a more negative effect for males than for females, and marriage has a more advantageous effect for males than for females. The extent of the mental health benefits of marriage is a function of both race and gender. One study found that marriage was associated with a 71 percent reduction in mental illness rates for minority men, 63 percent for white men, 28 percent for white women, and 8 percent for minority women (Russo, 1985). But why would single men have higher rates of mental illness than single women? Staying single does not cause men to have mental problems any more than it does women; rather, for men, the relationship is the other way around; men with serious mental problems are more likely to stay single. For example, male schizophrenics are more likely to stay single than are female schizophrenics (Birley, 1968; Garai, 1970). Taking the initiative in courtship and providing for a home and the support of a family require skills and resources which such a person rarely has. Female schizophrenics, on the other hand, are spread more evenly among the single and married populations of women.
Suicide
Suicide and attempted suicide are behaviors which clearly reflect very serious degrees of personal distress. Though not themselves defined as mental illness, they represent behavioral solutions, or attempted solutions, to intolerable pressures of anxiety, depression, or psychotic distortions of reality often precipitated by or associated with severe environmental stress. Here also the differences between the sexes are remarkable: men commit approximately three times as many suicides as women, while women make about four times as many attempts as men do (Garai, 1970). A simple comparison of suicide rates for males and females does little, however, to enhance understanding of the phenomenon. One could interpret the much greater number of attempts by women as evidence that more women are acutely distressed; but on the other hand, more men are successful. Men are more likely to use violent methods, such as firearms and hanging, while women use less aggressive methods such as pills or gas. The rate of suicide among women has greatly increased in the United States in recent years though that for men has not (Kushner, 1985). Furthermore, women in professional occupations such as medicine and psychology have a suicide rate about three times that of women in general (Schaar, 1974).
The differential rates of completed suicides by women and men have led to the historical treatment of suicide as gender-specific, that is, as reflective of “male” behavior. Women in their traditional domestic roles, so the argument goes, may make suicidal attempts, or “gestures,” but their completed suicides are infrequent. It is only when women begin to move out into the world and take on “male” roles that their rate of successful suicide rises. The notion of the “maleness” of suicide seems to suggest that the best way for women to maintain their mental health is to keep their place in the traditional institutions of patriarchy.
This argument, resting on the assumption of differential rates of completed suicides for women and men, has recently been challenged (Kushner, 1985). This revisionist view argues that the failure to count attempted suicides, made more often by women, gives the false impression that men are more suicidal than women are. In fact, many women who attempt suicide have as strong an intention of dying as do men who complete their lethal act. The strength of the suicidal intent is not related to the method used. Differences in suicidal completion rates between women and men are not a result of their gender, but reflect the methods available to women. Having had less access to lethal technology, and having been socialized to eschew violence, the methods chosen by women make it more likely that their intent will be thwarted by use of an ineffectual method or by discovery:
To take this historic pattern as an indication of the emotional needs of women is to perform violence of a different sort. Moreover, limiting . official statistics on suicide to completions ensures that suicidal behavior among women will be trivialized when compared to self-destruction among men (Kushner, 1985, p. 551).
Suicide rates are known to vary with marital status, with the lowest rates occurring among married persons, intermediate rates among the widowed and single, and the highest rate among the divorced. While males have a higher rate of suicide than females in all these marital categories, the disparity for males across marital categories is much greater than for females (Gove, 1972). For instance, for the ages twenty-five to sixty-four single females in the United States are 47 percent more likely to commit suicide than married females, while single males are 97 percent more likely to commit suicide than married males. Likewise the disparity for widowed and divorced males compared to married males is much greater than for females in the same categories. For example, the suicide rate for widowed females is about twice that for married females, while the rate for widowed males is over four times that for married males. As with mental disorders, it appears that the change in marital status from married to divorced or widowed has a more devastating effect on men. Likewise, the higher rate of suicides among single men compared to married men can be explained by the observation that men who are at greater risk for suicide because of emotional instability or other personality problems are less likely to get married, thus swelling the numbers of potentially suicidal men among the unmarried.
Social Roles and Mental Disorders
The higher rates for females in important categories of problem behavior raise an interesting question: What happened during the course of time to those auspicious beginnings of girlhood, when by all signs she was destined for a smoother developmental course than her brother? Most of the evidence indicates that her advantage begins to be lost during the years of puberty. Several plausible explanations have been presented, all of which have merit. But the search for the single cause is a vain one; a satisfactory theory will need to integrate several interacting factors contributory to this important gender difference.
No one proposes that women are genetically at greater risk for mental disorder than men are. In fact the opposite is more plausible, since the second X chromosome confers protective effects on females who have fewer genetic defects at birth and a lower incidence of central nervous system pathology. Biologically, females have an adaptive advantage that manifests itself in many ways. during their life span. But women’s biology is different in ways that have been seen as significant for mental health by some (including a White House physician who stated that a woman could never be president because of her “curious mental aberrations” associated with “raging hormonal imbalance”).[58] The decline of estrogen premenstrually and during the climacterium seems to be related to mood changes as well as to somatic symptoms in some women, and the high incidence of depression, especially in older women, may reflect a contribution from this source.[59] If the involution of the ovarian function was a major cause of depressive disorders, the incidence should be much higher than it is. Since women’s biology is the result of a long process of selection for adaptation, not maladaptation, it is logically improbable that it would have a decisive negative effect on her psychological well being.
Other explanations for the differences in mental health between men and women are based upon observations of gender-related socialization practices, the social roles of adult men and women which are the goals of the socialization process, the ways that the lives of women differ from the lives of men, and the gender-linked expectations of society, all of which are closely related to each other.
The effects of socialization into gender roles become more salient during puberty, when body changes further enhance sex differentiation, and relationships with the other sex and the development of social and interactional skills become critical concerns. Even in adolescence, girls seem to have a greater investment in personal relationships than most boys do. In 1963, Erik Erikson described intimacy as a normal achievement of late adolescence, a capacity to commit oneself to affiliations and partnerships, a stage of readiness for “true genitality” with one of the other sex. Many writers have argued that women value intimacy and affiliation more, and thus are more affected by their disruption or loss. Men, on the other hand, invest much of their energy in achievement strivings and the realization of vocational goals, valuing success in these areas as well as success in achieving a truly intimate relationship. Now the capacity and need for intimacy are not in themselves conducive to mental disorders. But girls and women whose identity is primarily maintained through their relationships with others and who have not developed an autonomous self-concept may be especially dependent on their affective environment and thus especially vulnerable to its course. In fact, in one view “failure to achieve intimacy with a man is probably the most serious factor precipitating mental dysfunction in women” (Garai, 1970, p. 134). While the validity of this assertion is yet to be demonstrated, there is little doubt that the achievement of intimacy is an important need for most women.
Gender-role socialization may be particularly important in the development of the eating disorders, bulimia and anorexia. More than 90 percent of people with eating disorders are women, an observation that inevitably calls for an explanation for such a huge discrepancy. Bulimia in particular is a near-epidemic on college campuses, and its prevalence has generated a considerable body of research (e.g., Striegel-Moore et al., 1986; Boskind-White and White, 1983).
Risk factors for the development of eating disorders are identified in sociocultural, developmental, psychological, and biological variables. The stigmatization of obesity, the heightened concern of adolescents with their appearance, the special vulnerability of young women with poor self-concepts and low self-confidence, and genetic effects on body weight are examples of these. Of particular importance to our discussion are socialization factors that impinge differentially on girls and women and account in part for the high incidence of these disorders in the female population in our society.
A woman’s perception of her body as she compares it to her conception of the ideal is one motivation for the development of an eating disorder. Thinness is a highly valued element of femininity and beauty, promoted by television, magazines, and diet books. Since beauty has such a central role in the feminine stereotype, it follows that women who espouse such values and who feel that their bodies do not conform to the ideal may try to reach their goal by the self-punitive and often dangerous methods of self-starvation or binge-and-purge. And it may not be chance that the explosive growth of the eating disorders has occurred during recent years as the beauty standard for women has moved toward an increasingly thin ideal, documented by the changing measurements of Miss America contestants, Playboy centerfolds, and female models in advertisements (Striegel-Moore, 1986). The fact that women much more than men develop eating disorders seems to be related to these pressures. Studies have shown that girls who are unhappy about their weight attribute it to overeating and respond by going on diets, while boys attribute weight to “excess bone and muscle.” Among high school students in one study, half the girls were concerned about their weight, compared with only 13 percent of the boys (Freedman, 1986). Differential perception of self and others, and values attached to “ideal” beauty, thus pressure girls and women more than they do boys and men to try to bring their bodies into conformity with their vision of perfection.
Some theorists contend that there is a relationship between the gender roles of adult women and men in our society and the rates of mental illness (Gove, 1980; Gove and Tudor, 1973). Women are more likely than men to have emotional problems because of their roles, for the following reasons: first, most women have a single major role, that of housewife, which includes being a mother. Men have two, head of the household, which includes being a father, and worker. Although a very large percentage of women are employed, most are in low-level jobs whose importance is economic, not central to their self-esteem and identity. Thus if the woman does not find her domestic role gratifying, she typically has no other major source of gratification. Second, since the major activities of the housewife do not require a high level of skill or education, they must be boring and frustrating to many women who are overqualified for the job. Third, the role of housewife is poorly defined and practically invisible. There is no special set of requirements for it, and its very diffuseness permits women to give play to their problems in a way that a structured job, subject to evaluation, would not. Fourth, the married woman who works is usually in a less satisfactory position than the married male. Not only does she earn less in a job with which she is minimally involved, but typically when she comes home she performs most of the household chores, so that her work day is much longer than her husband’s. Fifth, the expectations for women are unclear and even contradictory. Their lives seem to be contingent upon what others do, especially family members. Though educated in the same ways as men, they are still not treated as equals and remain essentially in the old institutionalized positions.
Conflicts and problems associated with family roles, in particular, are associated with higher rates of mental disorders. Whereas earlier theorists of psychopathology leaned toward locating the source of mental health problems in the afflicted person’s psyche, it is now clear that many such problems are generated by environmental stress, that is, by situations over which the individual may have little or no control. For example, low-income mothers in single-headed households with young children have the highest rate of depression of any demographic group (Russo, 1985). Generically, it is plausible that such women are under much more stress than are those with comfortable incomes, helping mates, and toddler-free homes. Marriage, of course, is no panacea. Marital difficulty is the most frequently reported problem presented and discussed by depressed women in outpatient treatment (Russo, 1985).
Some have noted that the typical emotional state for women is depression, and that the mental health of housewives is “public enemy number one” (Bernard, 1973). In 1942, Jessie Bernard proposed what she called the shock theory of marriage to explain the commonly reported phenomenon of the deterioration of mental health among married women, including the observation that the disparity between such women and their never-married sisters grew greater with age. Some of the conventional ingredients of the shock included the anti-climactic realization after attaining the sought-after status of married woman that she is now just a housewife, a role that involves menial labor and is low in status both to her and to society.
A more recently recognized shock is the fallacy of the sex stereotypes around which she has built her expectations (Bernard, 1971). Just as the child discovers the fallibility of its parents, the wife discovers her husband’s weaknesses and dependencies. She finds that he does not really know more than she, that he is not the calm, rational dealer in facts and relevant arguments, that he is not the kind of person the male stereotype pictures him to be. She finds that she is not really the weaker vessel and that often she must be the strong one in the relationship. Thus expectations of the marital relationship, built on stereotypes, and the reality of the roles themselves, result in a dissonance and a disillusionment for women, putting too much stress on those who are vulnerable and who are already at risk for the development of a mental disorder.
The gender-role explanation for higher rates of mental disorder in women is based, then, on the components of the adult role, on the realities of life for the average adult female and their potential for producing stress beyond the coping capacity of many women. The discrepancy between these realities and prior expectations built up by stereotypes is a secondary component of this explanation, a contributor to problems inherent in the role.
Another explanation for the incidence of mental disorders in women is based on the observation that women are freer to express how they feel than men are. In community surveys of mental illness where the data were self-reports of psychiatric symptoms, women reported more symptoms than men did. The investigators questioned whether this sex difference was real, suggesting that it could reflect men’s reluctance to admit to unpleasant feelings and sensations, since it is “more culturally appropriate and acceptable for women to be more expressive about their difficulties” (Phillips and Segal, 1969, p. 59).
Clearly, females of all ages in our society are permitted more freedom in the display of emotions of all kinds, although the mode in which the emotion is expressed may differ for the sexes. For example, if a woman is enraged she may cry, become hysterical, or withdraw; a man may shout, curse, or retaliate. The assertion that women are emotional does not really mean that women compared to men are emotional in the sense that emotionalism is a female attribute, like having breasts; rather, it means that women in general are more expressive of feelings. They have permission to show to others that they are experiencing grief, anxiety, excitement, joy, and concern. The male is expected to be more stoic, to look upon emotionally arousing situations almost as if they were problems to be solved. “Take it like a man” means don’t cry, do something about it; doing something about it, the issuance of an instrumental response, is one way to handle feelings, especially anxiety and fear (Kagan, 1972). An important corollary is that it is more acceptable for women to admit feelings associated with problems, such as depression, inadequacy, guilt, and low self-esteem, whereas men must avoid any show of weakness or inability to cope. Thus there is less dissonance for a woman when she takes the step of seeking help and becoming a patient and a statistic.
The Double Standard for Mental Health
During the 1970s researchers, especially women, began to examine old assumptions about the mental health of women and men, ideas about what is “normal” feminine and masculine behavior and personality, and the values associated with them. Early research along these lines strongly suggested that different criteria guided the thinking of clinicians as well as of lay people when they made evaluations about males and females. Findings emerged that seemed to reveal a double standard for what constitutes mental health and the healthy or nonhealthy personality—a double standard based on sex category.
One study focused on the hypothesis that the standards for evaluating mental health are different for males and females in our society (Broverman et al., 1970). Male and female practicing clinicians were given a set of 122 bipolar adjectives, each of which describes a behavior trait or characteristic such as:
very aggressive .... not at all aggressive
doesn’t hide emotions .... always hides emotions
The clinicians were divided into three groups. The first group was asked to indicate for each item the pole to which a mature, healthy, socially competent man would be closer; the second group was asked to describe in this manner a mature, healthy, socially competent female, and the third, a mature, healthy, socially competent adult, sex unspecified. The results revealed that the clinicians strongly agreed on the characteristics of healthy men, healthy women, and healthy adults, sex unspecified. But while the concepts of the healthy, mature man and the adult were not different from each other, the clinicians were significantly less likely to attribute to healthy women the same traits that they saw in the healthy adult. Women were seen as more submissive, less independent, less adventurous, more easily influenced, less aggressive, less competitive, more excitable in minor crises, more emotional, more conceited, and less objective—a strange description of a mature, healthy person. This finding suggests that the ideal personality is essentially a masculine model, and that women who conform to the female model are then in the curious position of being “normal” and deviant at the same time (Broverman et al., 1970).
In another study clinicians were given a psychological and educational history of a college student who was always identically described except for sex, John or Joan, and political orientation, left or right politically active. The clinicians ascribed significantly greater maladjustment to the left-involved female than to her male counterpart, and their verdicts for her were more severe than for the right-involved youth of either sex (Abramowitz et al., 1973).
Such studies, called analogue studies, were very popular in the 1970s. Analogue studies are those in which a contrived task that is analogous to “real life” is presented to subjects under controlled laboratory conditions. Analogue studies are easier to design and carry out and are more methodologically rigorous than are naturalistic studies. Such early analogue studies were very useful in demonstrating gender bias among clinicians and the double standard of mental health. However, recent studies indicate that analogue studies of such phenomena may have outlived their usefulness owing to clinicians’ increased awareness of feminist values and changes in women’s social roles. That is, the analogue situation itself is sufficiently transparent that its intent, to look for gender bias, becomes obvious, thereby leading the subject clinicians to endorse socially acceptable, nonbiased attitudes. Either that, or gender bias has disappeared from clinicians’ behavior and judgments. Naturalistic studies, however, using real-life clinical data continue to support feminists’ beliefs that patient gender does make a difference in clinical judgment:
It would be comforting to conclude that the analogue data are accurate and that sexism in clinical practice, if it ever did exist, is no longer a problem. This conclusion, however, is difficult to draw.... Even if glaring abuse of female patients is restricted to a small segment of mental health professionals, it seems unlikely—given the long-venerated traditions of sex role socialization in our culture—that subtle sexism is as rare as analogue research would appear to indicate (Davidson and Abramowitz, 1980).
The double standard of mental health clearly reflects role typing and sexual stereotypes. In summary, it holds, first of all, that the criteria for judging certain kinds of behaviors normal differ for males and females, secondly, that the traits which make up the male criterion are the norm for the healthy adult and are more highly valued in this society, and thirdly, that females who conform to the “feminine” criterion are thus not “healthy” by definition. The woman is put in a precarious double bind: if she is feminine, she embodies a collection of traits which are negatively valued. If she is masculine, she violates the behavioral norms for her sex and becomes subject to all the sanctions imposed upon deviants. Though the double standard is real, part of its identification is attributable to semantics and part to certain concepts that are held both by psychologists and by society. Taken together, these tend to perpetuate inaccurate conclusions with regard to the healthy personality.
The semantic problem lies in the differential designation of behaviors and personality characteristics as masculine or feminine, which implies that males do or ought to exhibit the masculine ones and females the feminine ones. Thus empathy is a feminine characteristic and inventiveness is masculine. The stereotypy here is obvious, since neither of these characteristics, nor dozens of others likewise sexually labeled, is exclusively in the repertoire of one sex and not the other. But the consensus for such designation is very strong, and it gives rise to the serious problem that behaviors are dichotomized along sex lines, thus setting the stage for differential valuing. For example, certain characteristics were agreed upon by college students to be more desirable in American society for males and females respectively (Bem, 1974). Males should be assertive, athletic, individualistic, and self-reliant, while females should be affectionate, compassionate, loyal, and understanding. These are only a few of the traits attributed to each sex. The students’ descriptors, with few exceptions, are not strongly negative or pejorative if applied to either sex; that is, it is acceptable for males to be affectionate, compassionate, and loyal, and for females to be assertive, athletic, and self-reliant. But the prevailing values of American society are such that as abstractions the masculine traits are likely to be seen as more valuable because they serve the goals of society. If they are “masculine” in most peoples’ minds then we have a double standard.
The other contributor to the double standard that is not part of its reality base is the concept that masculinity and femininity are mutually exclusive, that a person is either masculine or feminine but not both. This highly artificial dichotomy is incorporated into many personality tests so that a person’s orientation as measured by her performance on the test is in either a “feminine” or “masculine” direction.
However, some personality theorists have introduced the concept of androgyny as a replacement for sex-linked evaluations of personality (see, e.g., Cook, 1985). Their view argues that all individuals integrate in varying degrees personality traits that have been called masculine and feminine, and that socially desirable traits instead of characterizing one sex or the other are androgynous in that they characterize the healthy human regardless of sexual identity. Thus both a male and a female might be both assertive and yielding, forceful and compassionate, ambitious and sensitive to the needs of others. Such a person would be flexible, able to adapt to the needs of the situation and to engage in behaviors that were appropriate to it. By contrast, the highly sex-typed person who is motivated to behave consistently with a sex-role standard would have to suppress those aspects of her or his personality that were incongruent with that standard.
Support for such an androgynous model of personality was found when masculinity and femininity as two separate dimensions of personality were studied. College students who ascribed to themselves both instiumental (“masculine”) and expressive (“feminine”) tendencies were higher in self-esteem (Spence, 1974). College women who scored high on a masculinity scale were no less expressive but were more instrumental than feminine women were (Heilbrun, 1968b). Furthermore, the combination of goal-directedness and interpersonal sensitivity found in the masculine girls defined a more effective personality than that found in the feminine girls.
Perhaps the best androgynous model of personality, incorporating a nonsexist description of the healthy person, is based on Abraham Maslow’s views of the development of personality (1954). A distinctive feature of Maslow’s investigations is its focus on healthy, creative persons, in contrast to the more typical concern of psychologists with the pathologies, weaknesses, and negativisms of humans. Maslow thought that all humans have needs, capacities, and tendencies which are essentially good or neutral rather than evil, and that healthy, normal development consists in actualizing this basic nature, providing the environment in which it can grow from within rather than being shaped from without. When persons become miserable or neurotic, it is because the environment has made them so through ignorance and social pathology.
Maslow studied people who were “self actualized,” who had succeeded in developing their basic, healthy inner natures to their fullest expression. He undertook a series of studies whose goal was the discovery of characteristics which distinguish such persons from ordinary ones. His subjects came from all sectors of life; some were historical figures such as Lincoln, Whitman, and Thoreau; while others, such as Albert Einstein, were living. Among those he studied were four women: Eleanor Roosevelt, Jane Addams, Ida Tarbell, and Harriet Tubman.
What are the distinguishing features of the personalities of such actualized persons? They are realistically oriented, accepting themselves, other people, and the natural world for what they are. Their values are democratic, and they can identify readily with all kinds of people. They are at home in the world. They are spontaneous, open, and relatively free of neurotic defenses. Their appreciation of people and things is fresh rather than stereotyped. They have a childlike quality which lets them see and experience and feel as if each time is the first. They are problem-centered rather than self-centered. They are creative and resist conformity to the culture, transcending it rather than merely coping with it. Such self-actualized persons have a few deep relationships with certain important others. Emotionally self-sufficient, they strive for autonomy in their lives. They require privacy and enjoy solitude. With others they are never exploitative, nor do they confuse means with ends. Their humor is philosophical, often at their own expense, rather than hostile.
This is clearly a concept of the healthy personality whose features are independent of sexual identity. Biased toward neither masculinity nor femininity, it suggests that the most valuable traits are human traits, with no sex label, and by implication it advocates the kind of nurturance that freely permits the emergence of individual traits that are not a function of an arbitrary assignment based on sexual category.
An early study suggests how an androgynous model of personality might be manifested in healthy women. He found that women who were high in self-esteem were also tolerant of others, assertive, willing to take initiative, decisive, self-reliant, independent, and ambitious. They permitted themselves a wider range of sexual experience, had no fear of the body or its organs, and eschewed altogether the double standard of sexual behavior (Maslow, 1942). These are characteristics that are valued in our society, and are seen as descriptive of the healthy person, a far cry from the feminine vision of the clinicians (Broverman et al., 1970). Such characteristics do not preclude those positive ones usually attributed to women, which, whether manifested by women or by men, underlie the emergence of empathy and concern for others into human relationships. One remembers again Margaret Mead’s proposal that society make possible a broad and flexible range of models that would permit the unfolding of all temperamental variations in the absence of pressures to conform to a model based on sex category.
Women as Patients
The role of the patient is more compatible with the traditional female role than with the male. “Patient” behavior includes weakness, dependency, irrationality, childishness, submission to authority, and acceptance of care and attention. The patient, whether the disorder is mental or physical, is not expected to behave like a normal person. Rather, regression to a less effective and competent mode of functioning is expected and permitted. Thus an analysis of the patient role reveals it to be uncomfortably close to the traditional female role. The role of the sick one is less deviant for women than for men. When a woman becomes ill, she goes or is taken to a helper, usually a male, with whom she enters into a relationship that parallels others she has experienced, e.g., father-daughter, husband-wife, all having in common the dyadic male-female constituents who are respectively dominant and submissive, strong and weak, authoritative and yielding.
Not only is her “femininity” reinforced by the role of patient, but her helper, her physician or other therapist, is quite likely to share common social assumptions about her personality and behavior, and to treat her accordingly. For example, when physicians were asked to describe “the typical complaining patient,” sex unspecified, 72 percent spontaneously referred to a woman and only 4 percent to a man; 24 percent did not mention the sex of the patient (Cooperstock, 1971).
Women fit so naturally into the role of patient that often their complaints are seen as not “real,” as psychogenic in nature and at best uninteresting. One researcher found that women are held in low regard as patients, that less concern is given to their specific conditions and to their health care, compared to males. Included as examples are the observations that women are subjected to a high rate of hysterectomies, often without adequate indications; and that such research questions as the relationship between breast cancer, the second leading cause of death in women, and trauma attract neither medical researchers nor funding. Women were more likely than men to have their depressions and anxieties treated by drugs rather than to be helped to uncover the cause of the symptoms. Stereotyped attitudes and assumptions about “woman’s place” pervasively colored the doctor-patient relationship, and women were seen as unreliable personal historians whose emotionality always enhanced their disease—or itself was the disease (Howell, 1974).
Women receive a disproportionate number of drug prescriptions for both mental and physical disorders. In a study of 1.5 million prescriptions written by general practitioners in Australia, 80 percent were for mental disorders, most commonly for depressive neurosis, and the drugs were issued far more frequently for women than for men (Rowe, 1973). In this country, women get 60 percent of the prescriptions for nonpsychoactive drugs and 67 percent of the prescriptions for psychoactive drugs (Russo, 1985).[60] The heavy involvement of women in drugs tends to be hidden under the guise of legitimacy, since they are procured from physicians.
Perhaps the female-role stereotypes held by physicians influence them to over-prescribe drugs for women. For example, one study found that physicians were willing to prescribe tranquilizers to housewives because they could always take naps and needn’t be alert (Brodsky, 1971). Physicians saw daily use of Librium, a strong sedative, as much more legitimate for housewives than for students (Linn, 1971).
Advertising also plays a part in influencing physicians’ treatment of women. Increasingly, problems in living are defined as appropriate for drug therapy, with drug advertisements broadening the range of problem situations which allegedly can be helped by drugs. A content analysis of drug advertisements in leading medical journals over a five-year period revealed that men and women were depicted differently in the following ways:
-
Sex stereotypes were confirmed almost without exception in the ads.
-
Psychoactive drugs tended to be associated with female patients.
-
Nonpsychoactive drugs tended to be associated with male patients (despite the fact that women take more of them than men do), this fact implying that men have “real” illnesses, while women have mental problems.
-
The symptoms listed for male and female users of psychoactive drugs were different. Men presented specific, work-related symptoms, while women complained of diffuse anxiety, tension, and depression.
-
Male patients were depicted as older on the average, but in a wider range of ages than female patients.
-
Women’s illnesses tended to be shown as irritating to others and as socially embarrassing.
-
Women were shown as recovering from mental illness when they began to reassume sex-stereotypical behaviors and attitudes (Prather and Fidell, 1975).
Women and the Medical Profession
Most people would probably like to be able to take for granted that their diagnosis and treatment by highly trained professionals are carried out with scientific detachment, free of bias emanating from the sex of either the professional or the patient. One study strongly indicates, however, that such is not the case. Twenty-six clinicians, male and female psychiatrists, psychologists, social workers, and nurses, provided diagnoses for two hundred adult outpatients at a California community mental health center. Not only was severity of diagnosis directly related to the professional status of the clinician, but an interesting sex difference emerged. The relationship between professional status and severity of diagnosis held for the male, but not the female, clinicians. Female assessors were twice as likely to give a more benign diagnosis, whereas their male counterparts were disposed toward the more serious diagnoses of the psychoses. Further analysis revealed that sex of patient was important, too. The difference between the male and female clinicians’ degree of diagnostic severity was accounted for by female patients, with the female clinicians being especially disinclined to give severe diagnoses to female patients. Male patients were about twice as likely to receive more severe diagnoses, regardless of clinician sex. The authors suggested that the female clinicians’ leniency may stem from female socialization, which fosters empathy and inhibits aggression. This was reinforced by the female clinicians’ responses to questions regarding their lack of use of the more severe diagnoses. Their considerations included questioning of their own professional preparation, the derogatory connotation of a severe diagnosis, and their concern that it would stigmatize the patient for life (Wright et al., 1980). While the study supports the conclusion that women receive more lenient diagnoses from other women than from men, its importance is in its revelation of the subjective nature of diagnosis, which is dependent not only upon the objective criteria of professional standards, but also upon such clinician attributes as sex and status.
When a woman becomes a patient, then, for whatever real reasons, she enters a role which is invested with an accretion of assumptions, values and attitudes called forth by her identity as woman. It would be surprising indeed if her treatment did not reflect both the dimensions of the role and that special identity. Medicine is practiced in a social context and is no better insulated from cultural values than is the law or education. In order to eliminate sexism in medical practice, the following recommendations could be incorporated: (1) strengthen the historical and social science components of medical education; (2) reduce sexism in medical training, as well as in textbooks and journals; (3) minimize the power difference between physician and patient; (4) provide referral and alternative treatment facilities for the sexual, social, and other kinds of problems that women may tend to take to physicians; (5) promote education concerning health and treatment so that patients can make intelligent selections among physicians and treatment strategies; and (6) develop empirical evidence concerning the efficacy of various practices and treatments now in use (Fidell, 1980).
Evidence of attention to these concerns is now emerging. Some women physicians, for example, are calling attention to’ the demeaning attitudes about women which permeate medical training. At one medical school, two hundred students endorsed an open letter to their faculty pleading for an end to sexist terminology:
... We ask particularly that condescending jokes and statements concerning women and the women’s movement be avoided.... Some examples of insensitive statements made last year include: 1) the use of male norms as human norms ... ; 2) addressing the class as “gentlemen” rather than students; 3) the continued reference to adult women as “girls”; 4) asking medical students to wear jacket and ties rather than appropriate attire (Howell, 1974, p. 307).
Another example is the rise of the women’s self-help movement, which seeks to demystify medical practice and to make medical information more available to women so that they can better participate in medical decisions regarding their bodies. A notable contribution is the book The New Our Bodies, Our Selves, which informs women in plain language about their bodies and their functions and dysfunctions, thus reducing the knowledge gap between woman and physician. The effect can be to reduce the power gap as well.
Women and Psychotherapy
The term psychotherapy is applied to the use of psychological techniques by trained persons—clinical psychologists, psychiatrists, and social workers—to alleviate mental and emotional disorders or problems in daily living. Its usage is very general and is appropriate to a broad spectrum of theoretical orientations. Techniques may include giving emotional support and acceptance, retraining, hypnosis, releasing and interpreting feelings, or simply giving advice and directions. It carries no implication about the seriousness of the problem or the length of treatment. It has been used to describe the treatment of everything from nail-biting to schizophrenia, for periods varying from one session to several years. Almost always psychotherapy implies a personal consultation between a therapist and a client. Implicit in the practice of psychotherapy is the goal of change in the client—change in behavior, attitudes, beliefs, feelings, approach to life, well being, and mental health. While the extent to which psychotherapy of all kinds actually is effective is controversial, it is generally agreed that it is most helpful with younger, better educated clients whose values are similar to those of the therapist. Many persons who seek and receive psychotherapy are not mentally disturbed in the clinical sense; they are not suffering from a mental disorder. Such persons are often seeking help in dealing with a problem in their lives, like an unhappy marriage, misbehaving children, or lack of vocational or educational success.
Woman have always been the main consumers of psychotherapy from Freud’s era onward.[61] On one extreme, psychotherapy and marriage are seen as the two socially approved institutions for American women. In recent years psychotherapy as it affects women has come under critical scrutiny by feminists, especially by feminist therapists. These critics see psychotherapy as reflecting and reinforcing traditional values, beliefs, and attitudes about women and their roles, and thus failing to come to grips with the real problems of women inherent in their traditionally subservient and powerless role. It is the traditional role of women and stereotyped beliefs about women in relation to their role that are responsible for the increasing numbers of women who seek help for mental and emotional problems and for the ways they are dealt with by professional helpers in and out of institutions. To the extent that the values and goals underlying the treatment process reflect those held to be “normal” by the society as a whole, the therapy must reflect the pervasive sexism characteristic of the society (Hare-Mustin, 1983).
Although patients and therapists vary greatly in their demographic characteristics, the typical client in therapy is a white, middle-class woman, married, divorced, or single, while the typical therapist is a white, middle-class, married male (Greenspan, 1983). Thus both have been socialized within the traditional model of male-female relationships and are likely to share the values and attitudes inherent in that model. For women, the psychotherapeutic relationship is not unlike marriage. Not only is it a male-female interaction, but the therapist has or is perceived by the patient as having power, authority, control, and arcane knowledge which he will use to help her with her problems. Conditioned to expect and to value such attributes in males, she can move into the relationship without violating her sense of the fitness of things. The therapist can be a surrogate father, husband, lover, or priest-confessor for her in a role interaction that is both complementary and respectable.
The traditional definition of female sexuality and role behavior, the nature of the psychotherapeutic relationship, and the predominance of male therapists all may contribute to the formulation of goals for female patients that feature adjustment to their place in society. The therapist with traditional assumptions about sex roles, trained in an approach that has as its criterion for restoration to health the patient’s ability to function in conformity with society’s expectations, may interpret as pathological a woman’s expressions of discontent or condemnation of the feminine role.[62] The goal of adjustment to that role places the questioning woman in a very serious predicament. On the one hand she is enjoined to enjoy being a woman, while on the other, evidence all around her convinces her that psychological and physical femininity includes a collection of low-valued traits and the relegation to a role and status which not only do not command respect but are mostly irrelevant to contemporary life.
Psychoanalytically oriented psychotherapy which interprets women’s behavior through Freudian explanations and concepts has come under the heaviest criticism from feminists. The continuing influence of psychoanalytic theory on contemporary psychotherapy was illustrated by the psychoanalytic treatment of a woman who had become a patient after her former therapist and she had had a love affair. Analysis of this account of the four-and-a-half-year treatment of this woman reveals the patriarchal and authoritarian framework, of the treatment model, the assumptions underlying interpretations of the patient’s behavior during therapy, and the critieria that defined a successful outcome.
Treatment was based on Freudian theory, with modifications which the therapist thought were necessitated by her periods of regression:
having her sit up; permitting her to phone me at any time of the day or night; prescribing drugs on one occasion; insisting the patient and her husband visit each other .. . prohibiting a divorce; physically restraining her in the office ... demanding the patient be hospitalized; insisting ... that treatment continue until I agreed to terminate it; and, finally, that the patient adhere to the psychoanalytic method despite whatever feelings she might develop in the course of the treatment (Voth, 1972, p. 394, italics added).
This insistently controlling and authoritarian approach was thought to be necessary because of the patient’s rage and feeling of deprivation which resulted from her father’s death when she was very young, and from her former analyst-lover’s capitulation to her seductiveness which had ended so disastrously. Her strong penis envy drove her to wish to triumph over men; “She had defeated a man, proved herself superior to men, and had won the forbidden father” (p. 397), but in reality, “she had gotten neither a penis nor her father” (p. 396). At one point the patient attempted to wreck the office and had to be physically subdued. This incident was analyzed as a revelation of her resentment at continuing treatment and having to become more feminine. But when she became aware that termination was near, this plus “the challenge of accepting her feminine gender and feminine responsibilities and commitments” (p. 397) led to several suicidal gestures which were interpreted as a last resistance to acceptance of the fact that she would never get what she wanted, presumably a penis. But finally she said, “I guess it’s time for me to shape up and become a woman, wife, and mother” (p. 398). Even so, she continued to talk of committing suicide by drowning. At termination, the treatment was judged to have been fairly successful; “the patient was generally well controlled and friendly. Her child was doing well; she had a reasonably good social life, included in which was membership in a women’s club. The marital adjustment was much better; frigidity and bodily symptoms had disappeared; only brief periods of mild depression remained” (Voth, 1972, pp. 399–400).
In 1975 the American Psychological Association carried out an investigation of sex bias and sex-role stereotyping in psychotherapeutic practice. Women psychologists were asked to respond to a questionnaire regarding actual incidents and circumstances illustrating sexism in psychotherapy with women. Their responses illustrated five areas of sexist behavior which were of common concern: fostering traditional sex roles, bias in expectations and devaluation of women, sexist use of psychoanalytic concepts, sexual exploitation of female clients, and viewing women as sex objects. The greatest number of complaints was in the first category, with examples of therapists who encouraged women clients to get married, or to perfect themselves as wives, who depreciated the importance of a career, or who used clients’ attitudes toward motherhood as evidence of emotional maturity or lack of it. One therapist wrote, “I have had women report to me that they could not continue in therapy (with a previous therapist) because the objective seemed to be for them to learn to adjust better to their role as wives, mothers, daughters (underlings of one kind or another) and they needed to become free persons” (p. 4). Others reported knowledge of male psychologists who encouraged clients to continue to be docile, passive, seductive, and nonassertive, and to stay in professions “open to women” (p. 4). Respondents who had been in therapy themselves reported experiences of being pressured to have vaginal orgasms and of being told that their competitiveness was due to penis envy (Asher, 1975).
Feminist belief that sex bias exists in traditional psychotherapy has not, however, gone unchallenged. One writer criticized the research documenting sex bias on the grounds that it is methodologically unsound and does not empirically demonstrate that the sex of the client and the sex of the therapist make a difference in how therapy is conducted (Stricker, 1977). A major problem for such research is that it is extremely difficult to make observations in naturalistic, that is, “real life,” settings such as the practitioner’s office. Consequently most of the recent studies have been analogue experiments, in which therapists are asked to make evaluative statements, diagnoses, and prognoses based on fictitious information supplied to them by case report or viedotape. Such experimental studies have not, in general, supported the belief that therapists, male or female, treat patients differentially on the basis of sex. Others reviewing the problem note that the analogue type of study may have become so transparent to sophisticated clinician-subjects in such research that their responses will be in the socially acceptable (that is, nonbiased) direction, regardless of how they really behave in the consulting room (Davidson and Abramowitz, 1980). “[W]e may never be able to ‘prove’ that certain attributes relevant to sex bias are prominent among therapists. We can point to such attributes in individual cases, however, and we can prepare clinicians for their vulnerability to sexist behavior” (Brodsky, 1980, p. 335).
Growing concern about sexist assumptions and biases in the therapeutic situation and their effects on women has begun to result in the introduction of feminist values into psychotherapy with women. Feminist therapists of many different theoretical orientations have changed their ways of interacting with clients to reflect the feminist consciousness of the effect of the historical social oppression of women on their lives. A common goal of therapy illuminated by feminism is to help the client become aware of the social and political context of their psychological problems. Most feminist psychologists, female and male, identify themselves with the broad humanistic movement in psychology, which emphasizes individual growth and awareness of one’s feelings and their expression, valuing the quality of individual experience and its importance to the person rather than the dedication of oneself to the pursuit of goals defined by others as valuable. Self-nurturance and attention to one’s own needs are encouraged, especially in women who are on the self-defeating course of allowing themselves to be excessively influenced by the needs and expectations of others because they fear the consequences of others’ displeasure and the possible loss of love.
Typically, a woman who is involved in feminist therapy begins to see the extent to which external forces have shaped her behavior and are controlling the course of her life. As this insight develops, she experiences anger and frustration along with the realization that her problems are not all her fault, as she may have believed, but are at least partly caused by the fact that she is a woman in a sexist society. The therapist, fully realizing the pressures and demands that diminish women and drive them “crazy,” offers the client supportive understanding as she helps her to channel her anger, to identify the obstacles that are preventing her growth, and to seek out alternatives to her present behavior and life style. The client of a feminist therapist does not necessarily become a feminist herself, however, or adopt the value system of her therapist. She may wish to continue in a rather conventional marriage, for example, but under different conditions, such as greater personal freedom and greater involvement in activities outside the home without feeling guilty. Under such circumstances the goal is to help her to grow into the whole person she can be and to have the kind of life which is fulfilling to her, within the context of her personal circumstances and the framework of society. At times, however, the new consciousness that develops so alters a woman’s perceptions of herself and her life that nothing short of a drastic change will permit her to take advantage of her revised concept of what her life should be like. In either case, the therapist helps the individual to recognize the choices that are realistically available to her in her situation, and to identify the consequences of each of them. Unwillingness to face the need for change, to experiment with new ways of doing things, is seen as a form of self-betrayal, a refusal to take the risks inherent in the beginnings of growth. The woman must, in a sense, create herself. If her work is boring and unpromising, or a once-important relationship now sterile, she must confront these realities and examine what she can do to change them.
Theoretical interest in feminist therapy is intimately connected with its practice. An example encompassing both is a three-phase model of women’s mental health that moves from harmful adaptation to corrective action and health maintenance. Harmful adaptation is the process by which women learn to accept dependency and to practice self-negating behaviors. In adapting to the requirements of the patriarchal power system, women are harmed because they must thwart their own development and growth and deny their own nature as they internalize and justify the values of compliance and subordination within that system. Corrective action is a series of continuing steps in feminist therapy whereby the woman client begins to experience herself as a separate person and to become aware of the harmful adaptations she has made and their effects on her perception of herself. She begins to develop her own identify, apart from those with whom she is identified, such as husband and children, and to take on responsibility for building her own strengths and developing her own goals. Along with these growth experiences, she participates in health maintenance actions that validate the corrective actions she is taking and help her build a new basis for her life. Health maintenance includes developing a sense of pride in her identity as woman, forming relationships with other women that include sharing of experiences and pooling of strengths, and working with other women for change in power systems and the creation of alternatives to them. The movement is from acceptance and identification with the male-dominated status quo to the discovery of a consciousness of self and of one’s own needs and goals, to the emergence of pride in one’s womanhood and identification with other women, forming alliances in strength to meet woman-defined goals (Ballou and Gabalac, 1985).
Ideally, the goals of feminist therapy are not different in kind from the goals of all therapy: the alleviation of personal distress and the removal of growth-inhibiting influences and behaviors so that the person can mature emotionally and live effectively, in accordance with her desires and standards. The difference is in the extent to which the feminist therapist places the blame for the client’s problem on the structure of social institutions and stereotypes and encourages the client to see how these are affecting her and to challenge their impact on her life. Thus a feminist therapist would place herself in opposition to all the forces which attempt to pressure women toward submission to the status quo. This stance requires that she be aware of these forces and know what they are and what they are doing to women. In this respect, more than any other, she is different from nonfeminist therapists who may never have thought about sex roles as factors in emotional problems, who see sex roles as the natural order of things; if women, and men as well, are not adapted to their roles, then the maladaptation is seen as a problem. The feminist therapist would see the requirements of the role as itself a problem.
In 1978 the American Psychological Association published a set of thirteen guidelines for therapy with women (Task Force on Sex Bias and Sex Role Stereotyping, 1978). These reflect findings from the earlier study on sex bias in therapy. The intent of the guidelines is to sensitize therapists and to help them avoid sexist practices and assumptions as they deal with female clients.
There is a need to train all therapists to fill a greater number of roles. They should become experts on the research into sex differences and the psychology of women. Most therapists have little training in these areas and little understanding of the cultural and social antecedents of discrimination. They should be informed about alternative life styles and sex roles. Although trained to be passive with regard to innovative social trends and to avoid imposing their values on their clients, they should be willing to encourage women to seek out paths to self-esteem, even if these threaten to conflict with old family patterns of dominance. Their willingness to help educate the community and to work with groups has more potential for effecting change in attitudes than has the traditional mode of seeing only a handful of patients a week. Finally, more women should be encouraged to enter the mental-health fields at professional levels. Female clients could expect greater sensitivity to their conflicts, and empathy with their feelings; male clients could be confronted with the ways their stereotypes affect them, even within the dyad of the therapeutic relationship.
Alternatives to Therapy
Alternative kinds of help for women began to appear in the late 1960s and 1970s as part of the renaissance of feminism. One of the earliest of these is consciousness-raising (CR), a central feature of the women’s movement in its first few years. Women began discovering that the sharing with each other of their personal experiences and the examination of their lives in a society which conferred power on men and only indirectly on women was a potent technique for introducing women to the feminist perspective, for generating feelings of mutual supportiveness and sharing, for getting women in touch with each other and for breaking down barriers of suspicion and distrust which had kept them apart.
Consciousness raising is not therapy in the usual sense. The roles, the relationships, and the setting are all quite different. The CR group typically consists of a small group of women, five to ten in number, who meet weekly in each other’s houses to talk. Groups often are very diverse in membership, cutting across lines of age, race, and socioeconomic status. Such diversity enables the group to approach one of its goals, which is to realize the commonalities of experience among women, and the ways that society oppresses all women regardless of the individual differences in their personal situations.
Because of the egalitarian ideology of the women’s movement, the groups are leaderless. Each woman is her own authority, knowing better than anyone else her own personal experience. She shares this with the other members of the group, in conformity with certain informal norms: members are not interrupted or criticized; no one dominates or competes for a chance to speak; differences in life styles, backgrounds, and values are tolerated; members are supportive of each other but do not give specific advice.
Some groups use guidelines which offer suggestions for topics, while others deal with issues that arise spontaneously. Some examples for discussion include feelings about other women, experiences with men, feelings about one’s self and how one would like to change, sexual experiences, and family arrangements, such as the division of tasks. A major goal is the development of awareness so that one sees oneself and one’s experiences in a different light, as shaped by the sexual caste system of society rather than by one’s own misdeeds and shortcomings.
The content of the conversation of a small group of women during several sessions of their CR group revealed four main content categories. “Primary statements” synthesized each category. The content categories and their primary statements, with verbatim examples, are as follows:
-
Feelings about other women—women in the group desire support and trust from other women:
I was really quite glad that you did it—embraced her. Because I’ve thought since then how difficult it would be for me to reach out and touch someone. And yet there are times when I have wanted desperately to be able to do that and have felt a real sense of restraint. I find it very difficult to touch people physically.... I really appreciate the fact that the people in this group have reached out and allowed me to feel free to share some of whom I am and certainly have opened themselves up.
-
Self-perception—women in the group want to strengthen their self-concepts as physically acceptable and worthy individuals, to break out of the passive female role, and to establish themselves as independent mature people:
No, it’s being able to do it, not necessarily to feel that you can do it. I think that to be liberated you don’t necessarily have to live alone, you have to be able to live with yourself alone ... you’re accepting responsibility for yourself, for your actions, and not depending upon someone else to motivate you, to make you do certain things, to fulfill you.
-
Feelings about men—women in the group are seeking to restructure their priorities in intimate relationships with men, to seek independence, responsibility and autonomy, instead of security and passivity:
I guess I reject the idea that a woman has to be a nice guy and suffer in sex and sacrifice and I’m not about to suffer and sacrifice. I’ll suffer and sacrifice for somebody I’m into a relationship with and who cares about me and who I care about and who’s trying. But I’m not going to suffer and sacrifice for somebody that doesn’t, isn’t trying, and doesn’t care about me and all that.
-
Feelings about motherhood and children—women in the group want to accept motherhood and children as an integral part, but not the sole defining feature, of their identity:
Having four kids around all the time, it doesn’t take very long before you think that you’re an ogre when you go through the whole day doing all these hassles and everything ... you just get so tired of it and the mother is just saying, “Oh, my God, is there nothing else in the world except these little kids ... it just seems like it’s endless and it’s so dull a routine (Fish, 1975).
What effects does participation in CR groups have on women? Some of the most common Endings in the research include changes in perceptions and attitudes toward self, others, and society, with increased self-respect along with increased awareness of sexism in traditional gender roles; increased awareness of a commonality with other women; and the development of profeminist views of the female experience and the nature of female oppression) (Kravetz, 1980). As women learn to see themselves differently, they seek new definitions of self that are independent of the old contingent identities of wife, mother, or daughter, and they begin to move toward independence, autonomy, and self-acceptance. For many, the group has been the first time they have related in a trusting and noncompetitive way to other women; the feeling of a common sisterhood of women becomes strong. Often a new understanding of the mother emerges, evoked by recognition of the constraints under which she too lived. The convention that women cannot work together or trust each other conies to be seen as a device for keeping women apart, preventing them from gathering strength and thus maintaining them in the old positions of powerlessness and inferiority.
The ideology and goals of consciousness raising derived from a new, informed concern for women, by women, and of women. Clearly it cannot replace therapy for all women who have problems; some women who are in a CR group are also in therapy. Its constituency is mostly middle-class, educated, white women who are psychiatrically normal. It has, however, helped many women to rid themselves of the belief that the problems they have in living are altogether their doing, thus helping to break up old patterns of guilt and self-destructiveness.
In addition to CR groups, many other alternatives to psychotherapy for women have appeared. Some states have passed legislation funding centers for “displaced homemakers,” women who find themselves divorced at midlife, having the need to support themselves for the first time, often with few marketable skills. These centers offer support, counseling, skill evaluation, assistance in setting goals, writing resumes, and job-hunting, and other basic help to meet the needs that such women have. College campuses now have women’s centers, where women students can come to talk in groups, where paraprofessionals offer peer counseling, and a supportive environment helps women cope with the stresses of college life and personal crises.
Growing awareness of women as victims of violence, discussed earlier in this chapter, has created new systems for helping them, where none existed before. Shelters for battered women and their children are now found all over the country. Women may stay in these shelters for a few days or weeks, working with staff on their problems and making decisions about the future. Women who are victims of rape may now turn to rape crisis centers, where counselors help them to deal with their trauma, accompany them to the hospital, or go to court with them if necessary.
In addition to these social institutions, self-help books on assertiveness and problem-solving for women are widely available. Universities and other training centers offer courses in such women’s issues as divorce, single-parenting, career-planning, and self-assertion.
It is important to note once again that all of these forms of help for women, as well as feminist therapy, have grown directly out of the women’s movement and the feminist ideology of women helping women. Women have thus mobilized their own strengths to give support and assistance to other women in forms that never existed before.
In this chapter we have looked at some aspects of the experience and behavior of women who are in conflict with society, of those who are victims of violence, and of those who suffer from mental and emotional disorders. We have selected for emphasis those areas that are different for women and men, where the problems and maladjustments of women seem to be related to the roles they are relegated to in the society. The statistics on women in prison and women in therapy reflect these roles to some extent, though it is not possible now to know how many of women’s conflicts are role determined and how many result from the pressures of contemporary life, which affect everybody, regardless of sex. When women are victims of violence in such gender-related crimes as rape, battering, and sexual harassment, it is clear that women’s historical and traditional roles, especially their subordination to men, provide the context wherein such acts can occur. Research on problems that typically affect women and on the ways women cope with them is only a few years old. Research on problems that affect both men and women has usually studied men only. Few studies, for example, deal with women who are alcoholic or who commit crimes of violence. Differences in age, race, socioeconomic level, and education are obviously important variables in women’s problems and conflicts. Much more research is needed across the whole spectrum of problem behavior, so that knowledge can enlighten the efforts of those who try to help.
13. Middle age and aging
In masks outrageous and austere
The years go by in single file;
But none has merited my fear,
And none has quite escaped my smile.—Elinor Wylie, Collected Poems of Elinor Wylie[63]
As with other phenomena of women’s lives, aging has biological, sociocultural, and experiential components. Physical changes accompanying aging are universal, though individuals vary both in their resistance to such changes and in their resources to cope with them. Societies differ in their attitudes toward older people, the status accorded to them, and the roles assigned to them. These differences are reflected to some extent in the meaning that aging has for the individual. The significance of growing older for the individual woman is a composite of her physical and socioeconomic status, societal views, and her own perceptions and valuing of herself as a person.
In some traditional societies in, for example, Southeastern Asia and Central America, where young women are carefully guarded and restricted, older women are defined as asexual and thus can be freer from restraints. They can move about the city at will and interact freely with men. They have considerable power over the younger members of the family and often run the entire extended family. They may engage in business and other activities not permitted younger women, who may, in turn, be envious of the freedom and status they enjoy (Safilios-Rothschild, 1977).
In our society, by contrast, aging has traditionally been for women an unenviable prospect. Her most socially valued qualities, her ability to provide sex and attractive companionship and to have children and nurture them, are expressed in the context of youth, which is endowed with physical beauty and fertility. As she ages, she is seen as less physically attractive and desirable, and her reproductive and nurturant functions are no longer relevant. Since traditionally women have not been encouraged to develop those qualities that often improve with age, such as intellectual competence and the ability to apply mature wisdom to the solution of problems, the literature on older women has often focused on motifs of loss: of youth and physical attractiveness, of the regular reminder of femininity in the menopause, of children and perhaps husband, of purpose in life. The extent to which these changes are problems, however, depends upon cultural definitions and prescriptions for women and their roles and upon idiosyncratic variables of personality and circumstances. No biological imperative programs women to feel worn out, useless, and depressed during the second half of life. Furthermore, the dissemination of knowledge about health and nutrition and the development of new technologies to prolong life and to enhance physical well-being among both young and old hold forth the promise for the future of an aging experience less fraught with physical and psychological problems.
But women become middle aged and older, as do men, and hardly anyone views the prospect with complete equanimity. What does it mean to a woman to move past youth? What is it like? How does it feel? How do others feel toward her? In this chapter we shall consider some of the physical, psychological, and social aspects of the middle and later ages of women, and, on the basis of current knowledge, identify some of the factors that mediate both their successful and unsuccessful aging in Western society.
Biological Aspects of Aging
The biology of aging is concerned with changes that occur in individuals within a species as a function of the passage of time, and with explanations for characteristic lengths of life.
As persons grow older, they change in appearance because of certain biological changes that occur gradually over the life span. The more important ones of these are increase in connective tissue fibers between the body cells, gradual loss of elastic properties of skin and blood vessels, increase in fat, decrease in muscular strength, and diminution of secretions from the gonads, an effect that is more marked in women and is associated with loss of fertility.
These changes have their onset at different chronological ages and progress at different rates depending upon genetic and environmental variables. In general, such changes as these reduce the individual’s adaptability to withstand physical and psychological stress and to recoup strength and recover from illnesses and traumas.
Changes that occur in the central nervous system as people grow older result from quite complex events, including cell death, oxygen deprivation, and chemical changes in the cells themselves. Since these cells do not reproduce themselves, when cells are lost from disease, toxins, traumas, or other causes the diminution in number over time can result in a decrease in the efficiency of the brain’s functioning. The most pervasive effect of changes with age is a slowing of central nervous system activity causing, for example, the person’s reaction time to become longer. Clearly this change can affect a wide range of behavior, from intelligence-test performance to driving an automobile. But given the vast body of literature on sex-related differences in cognitive performance in children and young adults, little is known about such differences in older persons (Cohen and Wilkie, 1979). Since variability in test performance increases with age, it would seem important to search for the sources of such variation in individual difference factors such as sex, health status, life style, and so on. A review of the sparse literature on sex-related differences in older people yielded few clear-cut results (Cohen and Wilkie, 1979). It does appear that females perform better on tests of verbal ability, especially under fast-paced conditions, while males are superior on tests of spatial abilities. While the source of these differences is not known, they are consistent with findings on younger populations as described in Chapter 4.
Longitudinal studies measuring the same persons across time indicate however that those with superior intellectual ability decline hardly at all and may even continue to improve their performance, at least to age fifty. Persons of average ability begin to decline slightly after age thirty. As one would expect, a more precipitous decline is observed in those with accelerated brain changes owing to disease processes. The important point is that there is no drastic decline in intellectual ability in healthy older persons as a function of age (Kimmel, 1974).
The importance of this fact to the psychology of women is the difference not in ability as compared to men of any age, but in the extent to which ability is used as a resource, is cultivated to broaden interests and to enhance life’s satisfactions as the years go by.
Although the life expectancy for humans has increased remarkably in the last century, the upper limits of life span have changed little; that is, the proportion of persons in the population who reach such an advanced age as eighty has not changed much (Birren, 1964). Thus the upper limits of life for the individual seem to be genetically fixed, with the likelihood of living out this potential span dependent upon life conditions and events such as nutrition, medical care, accidents, and so on. As such environmental factors come under improved control, the genetic determinants of longevity emerge more clearly. One of these determinants is sex linked. As life expectancy has increased for both sexes, women have gained more years than men have. There is now a 7.7-year difference in average life expectancy: 69 years for men and 76.7 for women. The gap has widened from only 4.3 years in 1940 (Koten, 1978).
Women are the only primates who outlive their reproductive capacity. Females of other species do not have a true menopause (Riopelle and Rogers, 1965). The termination of women’s reproductive capability relatively early in life is adaptive for the production of healthy children.
Since the female’s ova in immature form are already present in her ovaries at birth, they are as old as she is at any given time. Cells develop defects in their genetic material over time, and ova also are susceptible to processes of aging which would be incompatible with the production of healthy offspring. An example of this is the well-established fact that the risk of bearing a child with Down’s syndrome (mongolism) increases remarkably with age (Nortman, 1974). Sperm by contrast are continuously produced in the testes and thus are not subject to the same risk of aging. Thus the termination of ovulation prevents what would otherwise be a rapidly increasing percentage of abnormal offspring.
Psychological Reactions
How do women feel about themselves and their lives when they reach the middle years? How do they react to the changes in body and in life style that accompany aging? Although women have higher rates of mental disorder in some important categories, notably the depressive disorders (see Chapter 11), the evidence is by no means clear that a majority of women find their middle years to be dismal and frustrating. The research, in fact, presents conflicting evidence, which has yet to be reconciled (Barnett and Baruch, 1978). A study of the perceived quality of life found no evidence that women’s lives are less rewarding than men’s. (Campbell et al., 1976). Yet another study of four groups of women and men at “turning points” (high school seniors, newlyweds, “empty nest,” and preretirement couples) found that the middle-aged women had the poorest self-concepts, were the lowest in life satisfaction, and felt the most despair (Lowenthal et al., 1975).
Earlier theories and research on middle-aged women almost without exceptions were based on assumptions that this time in the life cycle was highly problematic and that women had good reason to look forward to it with foreboding (Bart and Grossman, 1978). These assumptions seem to reflect the notion of biological determinism of female behavior. If the mind-body relationship is closer for women than for men, if women’s lives are defined mainly by their reproductive and maternal functions, then their terminations in the menopause and the empty nest would have profoundly negative effects on women in the middle years. But some writers are critical of the lack of attention to other variables in women’s lives, especially work and its conditions and gratifications, on women’s well-being as they move through life (Barnett and Baruch, 1978). For example, they cite a British study which found that for women who were both under stress and unable to turn to a confidante, work prevented the development of mental symptoms; only 14 percent of the women who worked outside the home developed symptoms, compared to 79 percent of those who were at home (Brown et al., 1975).
In this section, we shall look at some reported effects of menopause and some findings on depression and its relation to role loss in older women. Finally, we shall consider some emerging research that holds some surprises.
The menopause has been likened to a rite de passage, a ritual symbolic of the passage of the person from one role to another (Skultans, 1970). The menopause itself, the cessation of the menses, is a biological event which parallels other events along the course of aging. Although it is the manifest sign of the end of reproductive life, its symbolic meanings invest it with an importance which extends far beyond its biological definition. The cessation of the monthly bleeding after some thirty or thirty-five years comes as a specific physical event at a time when the woman also observes signs of aging in face and body, and experiences drastic role changes as children mature and leave home. Thus the menopause can appear as a sign of change, and the climacterium as a change of life, as it is aptly called by many—change in body, change in role and life style, and often change in the evaluation of the person by both herself and others.
Menopause on the average occurs among American women at age forty-nine. Although about 80 percent of women report some physical symptoms, most of these are minor (Perlmutter, 1978). However, a wide variety of other reactions are related, ranging from fear and boredom to relief and renewed vigor. Helene Deutsch, perhaps because of her emphasis on motherhood as the core of femininity, saw the psychological reactions to the menopause as being among the most trying of a woman’s life. Others take a positive view of the climacterium. Healthy women, newly freed from the demands of childbearing, can respond to the biological change with an influx of energy which could be directed to new aims, with a new impetus for socialization and learning. The many interests and productions of women after the climacterium, and their improvement in physical and emotional health, were cited as evidence that this period, in a psychological sense, is a developmental phase, a “challenge for the reorganization of the personality” (Benedek, 1959, p. 745).
The problem with most psychiatric and psychoanalytic studies of menopausal women is that they are based on observations of women who either perceive themselves or are perceived by others as having problems and needing treatment. On balance, the data are more supportive of the belief that healthy women move effectively through this phase than they are of Deutsch’s theory that women mourn the loss of their reproductive capacity and have great difficulty in coming to terms with their changed condition.
Supportive of this view is a comparison of beliefs of medical professionals and menopausal and postmenopausal women on the nature and causes of menopausal symptoms. The subjects—physicians, nurses, and laywomen aged forty-seven to eighty—were asked to evaluate fifteen frequently reported menopausal symptoms in terms of frequency, severity, and causality. 4 he women rated menopausal symptoms as significantly less frequent and less severe than did the medical professionals. They also were more likely to attribute symptoms to somatic, or physical, causes than were the physicians, who were more likely to judge them as psychogenic. Thus the laywomen had a more benign, less pathology-oriented perspective on menopause. When asked what they saw as a major factor in determining menopausal difficulties, other differences among the groups emerged. While all identified psychological and social factors as important, only the laywomen mentioned the importance of an active lifestyle in which physical fitness and activities outside the home are important. Worthy of note is the observation that literature on menopause that is directed to women emphasizes prevention and wellness through diet, exercise, and positive attitude. Medical practitioners, by contrast, focus more on traditional medical diagnosis and treatment in a context of illness (Cowan et al., 1985).
A group of one hundred white women aged forty-five to fifty-five were studied. A third of the women were still menstruating regularly, a third had not menstruated for at least two years, and the remaining third were in a transitional period. But presence or absence of the menstrual cycle was unimportant in the psychological status of the women; in the larger context of the biological, psychological, and social cues that signify the climacterium, they were more alike than they were different. That is, their life stage with its implications which were common to all of them was more important than the presence or absence of menses. Only 4 percent mentioned the menopause as an important worry, while more than half said that their greatest concern was widowhood. Other fears included cancer, children leaving home, or just aging. Asked about the most positive aspects of the menopause, three fourths named the elimination of the fear of pregnancy and of the bother of menstruation. Some mentioned better relations, including sexual relations, with their husbands. Only twelve of the one hundred women were unable to see any positive value. Some reported improvements in mental and physical health with increases in energy and feelings of well being. They attributed these changes to individual variables, not to a general effect of the menopause. Interestingly enough, when asked to compare themselves to “women in menopause,” they consistently rated themselves more favorably—they saw the problems in others rather than in themselves. These responses were seen as a defense mechanism which revealed the underlying ambivalence of the women toward the menopause, ambivalence rooted in personal and cultural attitudes toward aging and femininity (Neugarten, 1973).
Though most women take the climacterium in stride and play down the importance of menopause in their lives, about 10 to 30 percent have physical or emotional problems serious enough to cause them to seek medical help (Cowan et al., 1985).[64] Aside from the readily recognizable physical symptoms which have come to be associated with the menopause, the most frequent and most serious psychological problem of women in this age group is depression. In psychiatric terms depression is characterized by apathy, loss of interest and zest, loss of energy and appetite, feelings of worthlessness and guilt, and in serious cases the belief that life is no longer worth living. Feelings of depression and even prolonged depressive episodes are common experiences by no means unique to middle-aged women. But its incidence for this group has been extensively noted for many decades, and a sizeable literature on the phenomenon now exists (e.g., Sherman, 1971).
Depression which lasts longer than a fleeting despondency, or “the blues,” is usually interpreted as a response to loss of something of value to the individual; loss of a loved one, loss of self-esteem, loss of purpose and meaning of life. If we look at menopausal depression in the light of this interpretation, we can see at least a partial explanation foi’ it on the basis of role loss. A girl in our society is socialized to be as sexually attractive as possible so that she can find a mate, marry, and become a mother. If she follows this prescription, she faces the inevitable prospect of loss of youthful beauty, loss of children and their need for her, and probably loss of husband. To the extent that she identifies with her roles of mother and wife and evaluates herself by her performance of them to the exclusion of other roles and measures of her value, she is vulnerable to the feeling that her life has lost purpose and meaning when the roles are no longer relevant.
But too much free or uncommitted time is only one of the parameters of an epidemic condition. Cultural practices and attitudes, the availability of other roles, the extent of the role loss, and, perhaps most important, the emotional investment or involvement in the maternal role are all implicated in the adaptive outcome for the woman at this time of her life. An extensive study of depression in middle-aged women brought forth evidence on the variable importance of these factors. First, anthropological data on thirty societies and another six cultures were studied for information on menopausal reactions. Second, the hospital records of 533 women between the ages of forty and fifty-nine without previous hospitalization for mental disorder were reviewed. Third, interviews were conducted with psychological testing of twenty of the women to obtain information on maternal role loss (whether a child had recently left home) and type of relationship with children and husband. The results of the study were as follows:
-
Depressions in middle-aged women are due to their lack of important roles and consequent loss of self-esteem, not to the hormonal changes of menopause. In societies where the woman’s status was enhanced with increasing age, such depression did not occur. In the two where the woman’s status declined, as in ours, the effects were similar to those in Western countries.
-
Those hospitalized women who had a diagnosis of depression were more likely to have suffered a recent maternal role loss than were the nondepressed women.
-
Women who had overprotective or overinvolved relationships with their children were more likely to be depressed in their postparental period than were women who did not have such relationships.
-
Housewives had a higher rate of depression than working women when children left, since not only the maternal role but also the housewife role shrinks as the number of people to be cared for decreases. Working women, on the other hand, were less affected since they had another role in which they were active.
-
When ethnic groups in the sample were compared, Jews had the highest rate of depression, Anglos second, and blacks the lowest.
The traditional Jewish mother identifies very closely with her children and is susceptible to feelings of desertion and to self-punitiveness when they leave. The black woman, by contrast, is much less likely to suffer depression in midlife. Traditional patterns frequently include an extension of the mother role by caring for her daughter’s or other relative’s children while their mother works. Also, since the black woman is more likely to have been employed outside the home while her children were growing up, she might have avoided the intense involvement with her children’s lives and the vicarious living through them which characterized the Jewish mothers in the sample (Bart, 1971).
Thus depression is most likely to be found among those middle-aged women who are housewives, who have suffered a maternal role loss, and who had overprotective, overinvolved relationships with their children. Such a supermother has a conventional view of her role, an attitude of dedication, and a readiness for martyrdom. The depression developed because such a woman believed that by subjugating all her own needs to those of her family, especially for her children, she would reap the rewards of such selflessness later. Then when children left to pursue their own interests, she perceived that the pot of gold was not there, that her offering was not recognized; thus, her life seemed meaningless (Becker, 1964). In Portnoy’s Complaint, contemporary novelist Philip Roth described such a mother as she seemed to her young son:
It was my mother who could accomplish anything, who herself had to admit that it might even be that she was actually too good.... Weeping, suffering, she grated her own horseradish rather than buy the pishachs [urine] they sold in a bottle at the delicatessen.... The energy of her! The thoroughness! For mistakes she checked my sums; for holes, my socks, for dirt, my nails, my neck, every seam and crease of my body ... where health and cleanliness are concerned, germs and bodily secretions, she will not spare herself and sacrifice others.... Devot ion is just in her blood (p. 11).[65]
A broader cultural explanation, applicable not just to supermothers but to women in general, has become a challenge to psychiatrists and psychologists who treat middle-aged women with depressions. Women become depressed during this period because “they do not have enough reasons for satisfying action, and when they lose the one apparent reason upon which they predicated their lives— their femininity—their whole action world caves in. Let us be brutally direct: Menopausal depression is the consequence of confining women to a too narrow range of life choices or opportunities. It is a social and cultural phenomenon, for which the ‘designers’ of social roles are to blame. We create menopausal depression by not seeing to it that women are armed with more than one justification for their lives” (Becker, 1963, p. 358).
Supporting the above analysis is a reinterpretation of a case of Freud’s. A fifty-three-year-old woman became insanely jealous of a young girl working in her husband’s factory, believing that he was having an affair with her. Although her accusations were without foundation, she could not put them out of her mind. Freud saw her for two hours and decided that she feared that her attractiveness was waning, particularly her attractiveness to her young son-in-law, with whom she had an unconscious desire to commit adultery. Thus, her delusional accusations toward her husband were a cover for her own forbidden libidinous wishes for the love of the younger man. But there is no evidence in Freud’s account of the case that the woman was attracted to her son-in-law. Rather, the crux of the matter probably lay in her feelings toward the young career woman who had violated all the norms but was reaping the rewards of working in a man’s world, receiving money, and being treated with respect. The wife, on the other hand, had played by the rules, and her children had now grown up and married, leaving her alone with little to do while her husband continued to work at his factory and to enjoy a useful life. Her whole reason for being in the world had vanished, and her jealousy was a cry against helplessness, against personal and social injustice: “I have been cheated.” This jealousy-language, was the only cognitive tool she had to express the undermining of her sense of value as a human being. Yet Freud interpreted it as a cover for unacceptable sexual instincts and put the fault on the woman while maintaining the fiction that the social order was ethical and just (Becker, 1963).
Also analyzed was the guilt often felt and expressed by depressed women. The ordinary, conventional, mild housewife, searching for meaning in a life which no longer has any, takes on the total blame for her failure. Everyone else is good—only she is sinning, worthless, guilty. The key to understanding the paradox of such guilt-language in the absence of an apparent cause is the recognition that by its use the woman is attempting to make sense out of her inexplicable depression. Why should she be depressed? It is obvious that she has everything: a home, husband, children, and the knowledge that she has been patient and faithful in the role for which she was trained. If she now feels useless, it must be because she is evil and deserves nothing for herself. Thus she forefeits all claims of her own, and asks only forgiveness for her sin of existence. The self-punitiveness of guilt, like the obsessional jealousy of Freud’s patient, is a special language used by the woman who lacks the words and ideas with which to examine her life. And she lacks them because of the social tyranny which never permitted her to consider that there might be other life plans than the one she carried out. Such interpretation suggests an existential view that human life is motivated by the search for meaning, not for ways to express antisocial urges. In the light of contemporary data, this view better fits the patient’s case, without the invocation of unconscious urges which are not susceptible to proof or disproof (Becker, 1963).
If such depressions are artifacts of culture, not a fateful concomitant of aging tissues and ebbing hormones endogenous to the woman, then one would expect differences in reactions among women whose cultural role prescriptions varied. One study addressed the question, Which life style is most rewarding for the middle years, that of a traditional woman whose children are all about her, or that of a modern woman who can choose career, family, or both? The subjects in the study were women from five ethnic groups living in Israel and representing a continuum from traditional to modern: Israeli Muslim Arabs; Persian, Turkish, and North African Jews; and European Jews. These groups were chosen because, though they had a common heritage of tradition, especially traditions shaping the lives of women, they differed in the extent to which they had retained or repudiated the traditions. The traditional woman was subordinate to the male, illiterate, devout, custom bound, and the mother of many children. Progressing through the transitional societies to the modern, the woman had more nearly equal rights, a higher educational level, fewer religious controls, and a smaller, planned family. The groups differed significantly with regard to their perception and evaluation of the changes of middle life, and these differences related to the traditional-modern continuum. The modern women of European background were the most successfully adjusted. Coping actively with the changes of middle age, they welcomed the cessation of fertility and saw their marriages changing for the better. Next were the Arab women, of the most traditional, patriarchal group. Accepting the changes of middle age with equanimity, they saw their status and emotional health improving as they grew older. The most negative reactions of all came from the women in the transitional groups, who had not yet adapted to modernity but could not look forward either to the status of traditional roles for women, especially the role of matriarch. Thus both the traditional and the liberated woman adapted better in a psychological sense to midlife changes than did the woman who was neither. She paid the highest psychic price for her cultural dislocation (Dowty, 1972).
The theory and research on reactions to the climacterium, though they approach the problem from different positions and study widely varying samples have enough commonality of results to permit the development of w summary model presented in Table 13.1, which identifies the elements in society favoring a female pattern of values conducive to negative reactions.
Table 13.1 Model for negative reactions during climacterium
| The society | The woman |
| Socializes girls to wife-mother role. | Aspires to wife-mother role as ultimate fulfillment. |
| Youth oriented, values females as sex objects. | Self-esteem based on sexual attractiveness and maintenance of youthful beauty. |
| Denies or discourages other or additional roles for women. | Leaves job in first pregnancy. No career involvement of her own. Promotes and supports husband’s career. |
| Child-centered, nuclear family. | Dedicated mother. Children are her primary concern. |
| Values passivity, humility, and selfsacrifice in women. | Subjugates her own needs to family’s. Puts self-interest last. |
| Values masculine, competitive model of achievement. | Identifies vicariously with achievements of husband and child. |
| Male oriented. Women seen as inferior. | Sees self and other women as inferior. Ready to blame self, feel guilty. |
| Transitional. Both traditional and modern life styles in evidence. | Matriarchal role not available. Has neither desire nor necessary skills for “liberated” role. |
| Double standard of aging for men and women. | Fears aging with its loss of status, loneliness, isolation. |
Just as women outlive their reproductive lives, most of them in Western societies also outlive their maternal roles. As women live longer and have fewer children, they can look forward to two or three decades of postparental life. Studies of the reactions of normal women whose children have left home are rare, perhaps because this is a relatively new phase in the family-life cycle. In a study of the quality of postparental life, results were obtained which are markedly different from those described earlier dealing with maternal role loss. A door-to-door survey identified thirty-three couples between the ages of forty and sixty-five who had had one to four children, none of whom was still living at home. Forty-nine of the spouses were interviewed with questions designed to bring out evaluations of their present life situation, such as “How is your life different now from what it was when the children were at home?” and “How did you feel when the last of the children left home?” Clear evaluation of the postparental stage as better than any preceding stage of the family cycle appeared in twenty-two of the forty-nine responses, while negative evaluations occurred only three times. Almost twice as many wives as husbands saw their present lives without the children as better than before; on the other hand, wives were responsible for all three of the negative responses as well. Women with positive views saw this period as a time of freedom and time for the self, as in these typical responses:
There’s not as much physical labor. There’s not as much cooking and there’s not as much mending, and, well, I remarked not long ago that for the first time since I can remember my evenings are free. And we had to be very economical to get the three children through college. We’re over the hurdle now; we’ve completed it. Last fall was the first time in 27 years that I haven’t gotten a child ready to go to school. That was very relaxing (Deutscher, 1968, p. 265).
Other responses referred to improved relationships in the marriage and to feelings of accomplishment—of a job well done. The rare unfavorable evaluations centered about the advent of the menopause and aging, definition of oneself as a failure, either in work or child-rearing, and inability to fill a life left empty by the children’s departure.
Though women who sit in their empty nests and mourn may attract the most attention, many others, perhaps a majority, have little difficulty in adapting to the reduced responsibilities and new freedoms of postparenthood. In fact, the empty nest syndrome as a typical experience for middle-aged women is no longer salient. A study of subjective reports of well-being in a national sample of the population found that men and women whose children are grown and who are still married are very positive about their lives. “The empty nest appears to have a reputation it does not deserve” (Campbell, 1976, p. 121).
Other studies confirm that having children at home is a source of stress for some midlife women. Women who came of age in the postwar years when large families were the norm may still have one or more teenage children at home when they themselves are in their forties or fifties. When such women were asked to rate the difficulty of raising children at various ages, from toddlers to late adolescents, the difficulty scores went up dramatically with age of the child. Also, the larger the family, the more difficult child-rearing was reported to be. In fact, the most significant predictor of difficulty of rearing adolescent children was family size. Family size was also related to high levels of medication use by the women and lower ratings of competence in family roles. The author points out that family size as a source of stress may be less salient for future cohorts of middle-aged women, since women today are having fewer children and therefore will begin their postparental years at younger ages (Rossi, 1980).
Finally, we have two reports that, in today’s society, the middle years may be the best in a woman’s life (Bird, 1979). First, researchers were able to reinterview almost half the urban white adult subjects of the 1954 Midtown Manhattan Study that attempted to assess the mental health of that population. Results were analyzed to range from “well” to “impaired.” In the 1954 study, 21 percent of the women aged forty to forty-nine were impaired compared to only 9 percent of the men. Two decades later, only 8 percent of the women now in their forties were impaired, compared to 9 percent of the men. The pattern was similar for men and women in their fifties. A second study was based on a national health survey administered to a cross section of the adult U.S. population in the early 1960s and repeated with a similar sample in the mid-1970s. This study supported the first. Women over forty in the 1970s were less likely to report symptoms of psychological distress than were their counterparts who were that age in the early 1960s. The data were unchanged for the men. Interestingly, the improved picture for the older women was reversed for the younger ones in the two samples. Thirty percent of women in their thirties in the 1970s reported symptoms of mental distress, compared to only 23 percent of women in that age group in the 1960s.
What could account for this seeming shift in the best years of a woman’s life? Most women in their forties and fifties have experienced marriage and motherhood and no longer have young children at home. In today’s social climate they have more opportunities to explore their relative freedom than were available to their sisters of earlier times. Having “fulfilled” themselves in the traditional way, many may now take a new lease on life by pursuing educational and work-related goals, thus enriching the second half of life. By contrast, younger women today often report confusion as they perceive the alternative life styles now open to them. If they are married and have young children, they are less free to do other interesting things. If not married, or childless, and spending much of their energy on self-development in a career, they may still have yearnings for the more traditional tasks of women in familial roles. For them, more choices may mean more conflict; it remains to be seen whether today’s younger women will be mentally healthier when it’s their turn to be middle-aged (Bird, 1979).
In summary, while women may indeed respond to the body changes of the climacterium and may experience symptoms related to hormonal changes, the psychological reactions that they develop are less definitively tied to biological events than they are to the conditions of their lives. Fears of aging, loss of salient roles, and feelings of uselessness are more important to women’s existential experience of themselves at this time than is the menopause itself. Women whose self-esteem is intact, whose lives continue to be interesting and rewarding, and whose work, whatever its nature, helps them to feel that they are making a continuing contribution to the society, are the least likely to have negative reactions to the change of life.
Sexuality and Aging
The sexuality and sexual activity of the older woman are affected by a variety of physical and psychological conditions, as well as by the exigencies of her personal life style and her environment. The menopause and other changes associated with the climacterium in themselves do not produce any discontinuity in sexual desire or behavior. Though interest in sex is commonly assumed to decline with age for both sexes and generally does on a statistical basis, beliefs and expectations regarding this decline are often unrealistic and greatly exaggerated. Attitudes toward sexuality in older people are generally negative in our society, ranging from the view that the aging man and woman become essentially asexual, to the emotional reaction that any erotic interest on their part is offensive, unnatural, and disgusting. Jokes about love-hungry spinsters and dirty old men are plentiful and reveal popular stereotypes in some common themes: salacious interest in the older man who wants to perform sexually but cannot; desire for sexual attention in the older woman who is unable to find a partner because she is no longer attractive.[66] While these images may be painfully true for some, they are by no means universally valid, and perhaps they say at least as much about the prevalent values and anxieties as they do about reality.
Changes in sexual physiology occur with aging in both sexes. Some of these are in common, and are related to the general changes of aging discussed earlier. Strength and energy are reduced, for example, and body responses are generally slowed and attenuated. Basically, however, both men and women continue to respond as before, though frequency and intensity are reduced. Both remain capable of orgasm. Though exceptions to this basic principle exist, they are produced by factors other than normal physiology; that is, the loss of orgasmic capacity is not an inevitable concomitant of aging.
In addition to the thinning of the vaginal walls and reduction in lubrication mentioned earlier, postmenopausal women experience other changes in sexual physiology. The orgasmic platform develops less fully, and orgasmic contractions become fewer and less intense. 1 he uterus diminishes in size, and sometimes uterine contractions in orgasm are reported as quite painful. The labia become thinner, although the minor lips continue to respond with vasocongestion. Clitoral response seems to remain unchanged into old age, though resolution is swift. Most physical difficulties in having sexual intercourse are related to changes in the vaginal walls and mucosa. The thinning out and dryness can make intercourse uncomfortable, even painful. Some women experience irritation of the bladder and urethra after intercourse, resulting in burning sensations during urination. This condition is caused in older women by the partial atrophy of the vaginal walls, with resulting inadequate protection of the bladder. These problems are signs of postmenopausal hormone deficiency and can be substantially corrected or prevented by topical application of hormone cream as prescribed by a physician.
In males, the major concern is potency, the ability to achieve and maintain penile erection. While attaining erection tends to take longer, the older male can often maintain it longer, either from greater experience or from changes in physiological functioning. In any event, this change has the potential of enhancing his performance and effectiveness as a sexual partner from the woman’s view. Other changes involve chiefly attenuation of responses: fewer orgasmic contractions, less vigorous ejaculation, less marked change in the scrotum and testes, and a shorter resolution stage.
The effects of biological changes, including sex-hormone withdrawal, have only an indirect effect on sexual drive and behavior (Masters and Johnson, 1968). If the change in endocrine level were responsible for fluctuations in sexual activity in menopausal and postmenopausal women, we would see much more uniformity in such behavior. As it is, women vary widely in their responses to endocrine depletion as it affects sexual activity. Menopausal discomforts such as flushing, headaches, and nervous tension may diminish the woman’s interest in sex, but this is an indirect result of the endocrine imbalance. Since estrogen level is not directly responsible for the strength of the sex drive, hormone-replacement therapy does not increase libido. In fact, the use of estrogen replacement therapy (ERT) to correct certain menopausal symptoms has been sharply criticized, owing to reports of its connection with cancer of the uterus and blood clotting disorders, and also to the lack of demonstration of its efficacy. ERT appears to be helpful in reducing the unpleasantness of the hot flashes reported by many women in the menopausal years, as well as vaginal dryness. The former is a minor nuisance for most women, and the latter, as noted before, can be alleviated by topical treatment. Given the demonstrated risk of ERT, the medical profession has become more conservative in its use, and many physicians have abandoned it altogether.
By far the most important factors influencing sexual behavior in older women are the availability of a partner and the opportunity for regular sexual expression. Given these conditions, many women experience in their forties and fifties an increased interest in their sexuality for a number of possible reasons. Helene Deutsch thought that the approach of menopause signaled for some women a “closing of the gates,” arousing a desire for one more pregnancy as evidence of their femininity. For others, the cessation of the menses brings a freedom from fear of pregnancy so that the woman for the first time can abandon herself to the enjoyment of sex without apprehension. This release from “pregnancy phobia” is probably one of the most plausible explanations for increased sexual interest in postmenopausal women who did not have effective birth-control methods available to them during their reproductive years. Since young women of today have much less reason to fear unwanted pregnancy, their level of sexual activity may not show this later-life increase which has been reported by many observers.
The married woman in this age group may have other fortuitous circumstances which enhance her sexual expression. The problems which beset a young marriage, such as finances, in-laws, and friction in adjusting to the marital relationship, may all be in the past. The draining demands of having and rearing children no longer exhaust and preoccupy her, leaving more time and energy for the renewal of interest in herself and her mate. A revival of sexual interest may be one aspect of a more general awakening to the varied possibility of a mature life.
Thus the healthy, well-adjusted woman who is happily married may experience little or no change in her pattern of sexual activity.; in fact, she may find that her sex life has improved with the advent of middle age. But for very large numbers of women the picture is not so bright. The woman who found sex uninteresting and unsatisfying during her reproductive years may use the menopause as an excuse to terminate sexual relations, to rid her life permanently of the embarrassment and frustration which sex has meant to her. Related to this reaction are underlying puritanical beliefs that sex is basically sinful unless it is in the service of reproduction.
“Sexual liberation” programs have been developed for older couples with basically sound marriages to get rid of inhibitions and to increase their repertoire of sexual behavior. These programs focus on attitude restructuring and relationship enhancement. The therapist encourages sexual curiosity and exploration and gives exercises designed to replicate the fun of dating, such as candlelight dinners, love notes, and making love by the fireplace. These programs report some success in changing attitudes and behavior within weeks. Couples seem to communicate better, to increase intimacy, and to enjoy without guilt the sexual pleasures usually restricted to youth (Sviland, 1976).
Most studies support the idea that women have a more stable sex drive than men have and that it is less susceptible to the effects of aging. Although many men remain potent and sexually active into their eighty’s, impotence is a common problem past middle age. Studies of sexual inadequacy revealed that 83 percent of the impotent males were past forty years of age, and 75 percent were past fifty. There are a number of responsible factors for male impotence, chief among them the ego-shattering “fear of failure” which sometimes leads men to seek newer or younger partners in a search for reassurance of their virility. In any case, since women typically marry men who are older than they are, it is inevitable that some who are still as interested in sex as ever will find themselves with a husband who has withdrawn from sexual activity or is directing it elsewhere. Also, husbands in this age group may have physical problems or disabilities associated with advancing age which may make sex impossible for them (Masters and Johnson, 1968).
Because the ratio of men to women declines drastically with age, many older women are without partners. In the fifty-five—to—sixty-four age group, there are about eighty men to every one hundred women; in the next decade, the number of men to each one hundred women is about seventy-two; and after seventy-five, it drops to sixty-three (Puner, 1974). Widows outnumber widowers four to one, and only one-third of women over sixty-five in this country are married, compared to two-thirds of the men.
The older woman who is without a partner for whatever reason has a much more difficult time finding one, if she wishes to, than a comparable male does. There is a “double standard of aging.” One aspect of the “double standard” is that society accepts the idea of a man being involved with a younger woman. But society is less likely to accept the reverse. Another factor at play here is that our society worships power and youth, thus enabling the aging male, by virtue of his male status, to retain one of these “attractions.” When a woman is in her late teens or early twenties she attracts men of about her age or slightly older, marries, and raises a family. Some years later, if her husband decides to have an affair, he usually does so with a much younger woman. In the event of divorce, his chances of remarriage are excellent, but hers, at age forty or fifty, are not. Men in her age group are either married or seeking younger women. She has become sexually ineligible, whereas a male at the same age may be in no way less attractive than he was at twenty-five. But whether the reason is lack of a partner, inhibition and shame, or embarrassment over her aging body, the older woman is less likely to have an active sex life than is a man of comparable age.
Widowhood
Widowhood is rapidly becoming almost ubiquitous as a final stage in the marital histories of American women. The facts that many women marry men older than they are, live longer, and are less likely to remarry than are widowed males all help to produce the result that two out of three women over sixty-five in this country are unmarried, and most of these are widows. If a woman under fifty-five is married to a man five years younger than she, there is a 54 percent chance that she will eventually be widowed. If he is five years older, the chance increases to 64 percent. Lastly, there is an 80 percent chance if he is ten years older (Metropolitan Life Insurance Company, 1969).
A detailed analysis of widowhood based upon a sample of 301 Chicago area widows aged fifty and over illuminated the problems faced by urban widows by focusing on the determinants of their reengagement with social relations after their initial period of widowhood. The short-term needs of widowed women are summarized as follows:
-
Grief work. The bereaved one should be free to express her sorrow, loneliness, and other feelings activated by the death of a significant person. Family members and friends should allow her to move through the phases from shock to final acceptance and readiness to rebuild her life.
-
Companionship. The widows appreciated someone “just being there.” Since widowhood usually occurs after children are grown, the widow has lost the one person around whom her life was regulated. Loneliness becomes a pervasive problem as the woman learns to live alone for the first time in her life. Friends may stay away because of attitudes toward death or because they do not feel comfortable in the presence of grief and bereavement. The widow herself may feel ambivalent, expecting too much from friends on the one hand, or refusing all offers of companionship on the other, out of pride or suspicion that she is being offered charity.
-
Solution of problems. The people around her may want to give her too much advice, or to rush her into decisions, such as selling the house or moving into a retirement community. Only immediate crises should be dealt with, since the chances of making wrong decisions are great, and her view may well change after the period of grieving is past. No one should make her decisions for her, since they may be ill informed or lacking in understanding of her real needs. Furthermore, a take-over attitude on the part of others can have the effect of fostering dependency and undermining her confidence in herself and her ability to solve her own problems—a self-confidence which may be low to begin with and, most of all, in need of bolstering through the experience of successfully making decisions for herself.
-
Re-engagement into social involvement. The extent to which the widow engages or re-engages in social relations and activities reflects her location in the modern social system. Her educational level and her financial and occupational status influence the widow’s involvement in her community, her relations with friends and neighbors, and her membership in voluntary groups. Three types of widows are described in terms of the degree of their re-engagement and its relation to the woman’s past life situation. The first is adapted by socialization and education to modern society; she is selfinitiating, capable of re-examining her life style and goals after her husband’s death, and of choosing which aspects of her old roles she will maintain and which she will give up. She is conscious of the need to adjust behavior and relations to her new status, and she initiates changes and retains control of her life, rather than passively reacting to poorly understood external events. The second type of urban widow, living in an ethnic “village” in a traditional life style for which her socialization prepared her, may change very little. Her kin relations, close peer group, and neighborhood system may continue to involve her much as they did before, especially if her world is essentially sex-segregated, as is the case among many groups of lower-class urbanites. The third type of widow is the social isolate who lacks the ability to engage effectively with modern society. Hampered by lack of mobility, finances, or bad health, and socialized into a passive stance with regard to affecting her environment, she cannot develop new social roles as old ones disappear, hence she tends to withdraw into isolation, rarely leaving her home and unwilling or unable to initiate any contact with other persons or groups.
A basic difference between the two extremes of the active, engaged woman and the social isolate was education. A low level of education meant that the woman was likely to have married a man of similar status, and that the family income was always minimal. Marginal to the social system, lacking skills for re-engagement into society, she is dependent for her involvement upon chance and the actions of others. “The best position is that of the widow who was socialized into the modern social system and has enough financial and health resources to participate” (Lopata, 1973a, p. 270).
In another analysis of the data, the popular belief that black women are surrounded by kin and thus by implication would be less likely than white women to suffer from loneliness and isolation was considered. To the contrary, it was found that most of the black women were not part of an enduring kinship structure. Two-thirds of both groups had no children living with them, and about that same proportion reported little or no contact with siblings. Regarding attitudes of the two groups, the white women had more positive memories of their husbands than did their black counterparts, more often responding that he was a good man, that their sex relations were good, and that the marriage was above average. The black women were less likely to agree that decision making was hardest for a widow to learn but were more likely to believe that widows are often sexually propositioned, that other women are jealous of them, and that people take advantage of them. And they were twice as likely to feel sorry for their married friends. Thus the evidence suggests that these black women, most of them migrants from the South and poorly educated, had more negative feelings toward their late husbands and toward marriage in general than did their white sisters. But older widows, both black and white, lead lonely lives (Lopata, 1973b).
The popular wisdom would suggest that widows, freed finally from their caretaking roles and having lost the intimacy and companionship supposedly shared with their husbands, would turn to other women for support and company. Friendship is idealized in American culture, but in the lives of today’s adult and older women its place is equivocal. Consider society’s view of the roles and meanings of friendship among widows. For adult married women, crosssex friendships are taboo, since they are endowed with sexual overtones. Close same-sex friendships may also be problematic, since they may interfere with the marital role. In addition, women are supposed to stay unentangled outside their families so that they can play the role of helpmate and follow their husbands wherever their careers take them.
When husbands die, it may be difficult for widows to change their styles and move closer to other women for friendship and support. One study showed that few widows were closely involved with friends. Some had had no friends when their husbands were alive and continued friendless in widowhood. Some who had had friends when their husbands were living were able to keep them into widowhood. Since American social life is built around couples, however, some widows reported fewer social contacts, being left out of their married friends’ social events, or feeling like a ‘’fifth wheel” if invited (Lopata, 1977).
The number of friends that a widow had and their importance in her life were related to education and income level. The more disadvantaged a widow was, the less likely she was to have even one friend. Some friendless widows were not unhappy with this state, having a history of social isolation except for family and relatives. Others wanted friends but did not have the resources or social skills to go about making them. One writer has surmised that, if the feminist movement moves down through the American class system, women will be more likely to turn to and value other women and will feel less stigmatized for being without a man (Lopata, 1977).
Other sources of support and intimacy for widowed women include relatives, associates at work, and peers in voluntary activities. Even service providers such as physicians and store clerks may provide a few moments of attention and thus alleviate the feeling of being all alone. Some less obvious relationships that may be of comfort to some are a continuation of the sense of the spouse’s presence, talking to his photograph, imagining him giving advice, and identifying with some of his characteristics; a relationship with God, which may appear as a strengthening of religious belief systems, or increased church attendance; or an engagement in interaction with the self, taking the self as the object of compassion, nurturance, and care. Widows who adopt this last mode of meeting some of their intimacy needs are described as energetic and able to learn from new experience. Their self-esteem is high, and they take much joy in life (Barrett, 1981).
Sometimes the bereavement of the widow brings forth “gifts” that she can offer to make the relationship with others reciprocal. Married women with widow friends, for example, are more prepared for widowhood than are those without. Also, previous losses may be better integrated by talking with someone who is presently experiencing a loss. Sometimes the occurrence of death brings a surge of emotional feeling that is growth-enhancing (Barrett, 1981). The letter of one young widow to friends after the death of her husband is an example of transcendence of loss:
To all of you, I would say (as I’m sure Mark would wish me to)—live out your love for one another now. Don’t assume the future; don’t assume all kinds of healing time for the bruised places in your relationships with others. Don’t be afraid to touch and share deeply and openly all the tragic and joyful dimensions of life (Cassem, 1975, p. 16).
After Widowhood: An Example
In thinking about and attempting to characterize the later lives of women, as with any developmental period, it is easy to forget that one is generalizing from information gathered on groups of individuals who are alike in some ways and unique in many others. The personal account of the woman presented here does not refute the research; but it does offer a suggestion of the individuality lost in statistical data, and an assertion of the personal spirit whose dimensions transcend the formal rules of scientific inquiry.
Angelina’s story, Angry hi Retirement (Hughes, 1974), tells of the drastic changes in her life after her husband, Armando, died; of her struggle to maintain her dignity and pride; and of her small victories as she battled the enemies of the old: loneliness, helplessness, and dependency. During their fifty years of marriage they had built their own house, with a rose garden and fountains like those in Armando’s native Italy. Armando worked for a newspaper; Angelina cared for the two children and the house, worked in her church, and did some part-time translating. After their son died and their daughter moved away, they stayed in their home among their friends and lived on their modest retirement income.
Angelina was completely unprepared for Armando’s death. Well-meaning friends insisted that her house was too big for her and that she needed a place where she would be taken care of. She felt “tired and weak,” pushed into making decisions. Decisions had always been Armando’s responsibility; now, it was easier to let others make them. The house was sold, and in a few weeks she moved into a “retirement home,” which required that she relinquish all her financial assets in exchange for lifetime residency in a small room with communal bath and twenty dollars per week allowance. The room was cluttered with her personal possessions, and the closet space was inadequate. But why should she worry about clothes, when one of the first questions asked her was where she intended to be buried? Should she tell them she came here to live?
She had to fight to keep drapes, a small rug, and her bookcase, which interfered with “housekeeping.” “I can still feel the anger rage inside me. It was hard for me to keep my chin up and maintain my pride. In my own home I was queen, but here I felt like a child” (p. 58). Her helplessness in the face of the power of the staff overwhelmed her. They controlled whether she got an extra piece of toast, a clean towel; they could put her out, indigent, at any time. Worst of all, they controlled how she, and the others, felt about themselves.
She found herself in “crafts” making pincushions and mice out of grey foam rubber. She knitted a cape which was sold for $2.50 at the bazaar. Was this the price of her time and energy? When she questioned what happened to the money made from the production of the residents, she was rebuffed. Old ladies were not supposed to ask questions. But Angelina resisted the deadening conformity which was forced by fear on the other women. She persuaded the administrator to locate a record player to be put in the parlor. “Where there is music, there is life.” She recruited other residents to go out with her on her daily walks, even in cold weather. She started poetry reading sessions, and planned for concerts. But there were always the rules regulating their days. She had to ask permission to stay up past ten o’clock to watch the news: “I must go ahead and live!”
A year later, Angelina was feeling less rebellious. Trying so hard to be heard had depleted her energy; she felt choked and unable to express herself. But she still wanted to contribute, to feel a part of her “home.” “The music in the parlor is beautiful. We love it. The monotony has lessened. We talk and the music plays softly. Maybe there will be more than pincushions” (p. 59).
Angelina’s story is distinguished only by her persistent sense of self and her resistance to relinquishing her freedom. Because the outlines of it are common enough, it reflects rather clearly attempts on the part of Angelina and others to meet her perceived needs immediately following her bereavement. She was unprepared for coping with the problems attendant upon the loss of her husband of over half a century. Instead of allowing her time to work through her grief and to reach a stage of readiness to think about the future, those around her advised and persuaded her to make decisions which she later regretted. She had no time to build confidence in herself by surveying her options and making her own choices. By the time she was ready to “re-engage,” she was in an institution for those who have little to do except wait for death. Even there, she tried to maintain her self-esteem and to assert some degree of control over her life and to keep alive hope for the future. Her story demonstrates the interaction of circumstances and personal qualities which determines the course of a life in the later years, after the death of a spouse.
Throughout this book we have discussed the effects on women of certain modal and developmental experiences in their lives. In general we have seen that women’s psychological reactions to these events—menarche and menstruation, marriage, pregnancy, childbirth, work roles outside the home, sexuality, and aging—have been inextricably bound up in the social context within which they occur. Widowhood is no exception. In fact, while loss and loneliness are real, their impact on the person and her subsequent adaptation are dependent both upon her own inner resources and strength and resilience of personality, and also, especially for the old and vulnerable, upon her place in the society, her material resources, and the quality of the help and emotional support she receives from others.
Personality and Aging
We have spoken frequently of the social context within which behavior occurs and its importance for the development of patterns of behavior. When the social context changes, and when the passage of time brings physical changes as well as life-style changes, we would expect that some aspects of the person and her characteristic, unique behavior would undergo change also. At the same time, we would expect the healthy person still to be herself, not radically different at sixty from the way she was at forty.
Longitudinal studies of persons across the life span reveal both consistency and change in the characteristic behavior of persons as they grow older. A major study sampled 700 women and men between the ages of forty and ninety who lived in their own homes. Interviews and tests over a seven-year period revealed consistencies across time for individuals, as well as age-related changes.
A central finding was that some aspects of persons were relatively stable across time. These dealt with “adaptive, goal-directed, and purposive qualities of personality,” that is, general adaptation, cognitive competence, and characteristic style of interaction with others. Such characteristics as emotional stability and intelligence, and personality traits such as hostility or passivity remain generally consistent across time. This was true in spite of role, status, and other changes related to aging. To this extent, “Behavior in a normal old person is more consistent and more predictable than in a younger one.... As individuals age, they become increasingly themselves, and, on the other hand, ... the personality structure stands more clearly revealed in an old than in a younger person” (Neugarten, 1964, p. 198).
Other studies based on these data found changes in the subjects that were age-related. That is, some general changes characterized the sample as a whole as a function of aging. These include a decline in ego energy, a shift in ego style, and shifts in sex-role perception. The first change was a consistent decline with age of the amount of emotional energy the person had to invest in the outer world. With this decline went a certain withdrawal of responsiveness to outside stimuli, an abandonment of self-assertiveness, and an avoidance of challenge (Rosen and Neugarten, 1964). The second change related to the decrease in ego energy was a shift in ego style from active mastery to passive and inappropriate mastery styles. These three types of ego style were seen as stages on a continuum from the most vigorous and effective type of functioning, through passivity, to stress-laden, maladaptive functioning. These two age-related changes, or directional shifts, characterized both the females and the males in the sample (Gutmann, 1964).
The third age-related change was in the perceptions of the sexroles of older women and older men. Subjects ranging in age from forty to seventy were shown a picture of four persons, a young man and woman and an older man and woman. Most saw it as a two-generational family. The descriptions of the older man and woman given by the older persons in the sample, those aged fifty-five to seventy, differed significantly from the descriptions of the younger ones, aged forty to fifty-four. The shift was in the direction of a sex-role reversal, with the older respondents perceiving the old man as more submissive, and the old woman as more authoritative, compared to the perceptions of the younger group. For both men and women in the older group, it was almost always the old woman, not the old man, who was seen as aggressive, dominant, and impulsive (Neugarten and Gutmann, 1968). While one cannot infer actual role shift from these data, it was suggested that actual personality changes are implicated, with women becoming more tolerant of their own aggressiveness and impulsivity, and men of their own nurturant and affiliative impulses. As each becomes more detached from the outside world and its influences with a diminished need for mastery over the self and its impulses, the differences between them seem to diminish.
Attitudes toward Aging
The notion that age and aging mean something different for women than they do for men has been suggested earlier in this chapter. The sexual and social devaluation of women who are beyond the age of youthful beauty, who no longer fit the girl model so adulated in our society, is part of the experience of most women past thirty-five or so, though that realization is more important to some women than to others, depending upon their other values, sources of self-esteem, and supportive relationships. The true pervasiveness of the horror of being no longer young is difficult to assess. No doubt some part of it is cultivated by the advertising media to promote the multimillion-dollar industries which depend upon women’s fear of being seen as old or unattractive to sell products. The ubiquity of the value of appearing young is such that one cannot know to what extent it is an artifact of prevailing pressures, or even how much it will diminish as women become less dependent upon the adulation of others as a sign of their merit. In any case, the phenomenon of an aging appearance affects women more than men in ways that are remarkably different psychologically.
When a group of women aged thirty-three to fifty-six were asked what age they would “most like to be” and to what age they would like to live, none wanted to be older than they were, and half wanted to be under thirty. On the average, they expressed the wish to live to be at least seventy-five, with a range from fifty-five to eighty-five. Those who wanted to be much younger than they were, and those with short longevity preferences, were women with high levels of stress in their present lives, such as marital tension, large families, economic problems, or recent increases in symptoms of aging in themselves. Those whose lives were going well had no desire to be younger than they were (Rossi, 1980). The inference is that contentment with one’s life generalizes to its various parameters: if one is happy with one’s situation and with oneself, one is less motivated to want to change anything, even something that is negatively valued in the society, such as an aging persona.
Women’s attitudes toward aging are also affected by their perceptions of their own mothers. Some women see their elderly mothers as role models for growing older. Having a mother who is active and in good health helps one to feel optimistic about one’s own future as an older woman. One professional, single woman in her late forties said about her eighty-one-year-old mother:
My mother is in a very nice situation, and it wouldn’t be something I would have anticipated a little earlier about getting old.... I think it’s the fact that she lives in a very nice place, she’s been very active there and seems to like her life better and better. So I do not feel so pessimistic about getting older. It gives you a positive outlook!” (Baruch et al., 1983, pp. 206–7).
In some societies, people gain in status and prestige as they grow older. In our society, valuing as it does youth and achievement, persons who are no longer young and achieving are no longer accorded status and attention. There are a few indications that the values of our society are shifting slightly in the direction of a greater appreciation for mature women. In the April 24, 1978, issue of Time magazine there appeared an essay titled “In Praise of Older Women.” The author pointed out that most of the era’s heroines were in their thirties and forties: Jane Fonda, Audrey Hepburn, Princess Grace, and others. The author credited feminism and its attendant social changes with helping women to be more self-confident, more independent, and less concerned about the evaluation of others. Today’s woman is less likely to be enslaved by the whims of the fashion industry or to panic if she is still unmarried as she approaches thirty.
Another factor that will become increasingly important in changing attitudes about aging is the general aging of the population as fevver babies are born, and as the “babyboom” cohort, now in its forties, moves across successive decades. It will be interesting to see how the meaning of aging changes as older people become more visible and, because of their numbers, more powerful.
A futurist perspective on women and aging predicts that women who will be forty-five and over in the first quarter of the twenty-first century will have greater access to prestige and status, as well as improved opportunities for meeting needs for affection and support, than do their sisters oi today. If contemporary trends continue, women of the future will have had greater labor force participation, with better chances of occupational prestige, economic independence, and a stronger repertoire of socially valued competencies (such as those that men have today), than do middle-aged and older women today. Also, tomorrow’s older woman will have been brought up in a freer climate of ways to live, with more experience in transitory living/loving relationships, including living with partners outside conventional marriage, divorce, and more sexual experience. Since these represent experience with adapting to multiple relationships, they can provide training in coping with loss and in learning to be more self-reliant and self-directed. Older women of the future will be less inhibited, placing a higher premium on sexuality. Not only will the frequency of their sexual activity be higher, but the range of their potential sex partners may broaden to include same-sex as well as a broader age range of males. Assuming the continuation of current trends, the prospects look brighter for our daughters and granddaughters as they move into the second half of their lives in the century to come (Abu-Laban, 1981).
Women need not wait for society’s attitudes toward aging and older women to change. Women must find in themselves the alternative to the pain of feeling rejected and worthless. Returning once more to the model of the self-actualized personality, we can hypothesize that the self-actualized woman will be less affected by others’ perception and evaluation of her appearance, that her self-esteem will be more independent of such appraisals, that she will more likely be, in Whitman’s words, well-possessed of herself. As women develop greater strength, independence, self-sufficiency, and pride in themselves as women, as their identities become less contingent upon their relations to others, as they become freer to let themselves be, then the specter of middle age and aging will be divested of the special meanings that it has for women. It seems, then, that we must help ourselves, each other, and our children to develop our potential as humans and to learn to love ourselves better for how we are and what we do than for the ephemeral qualities of our youth. Then, as Helene Deutsch said, perhaps we can see our aging “not as an inversion but as a harmonious consequence” (1973, p. 216).
Epilogue
The psychology of women through the life cycle is better understood today than ever before in human history. Even so, because of the enormous diversity even in our own society, to say nothing of other cultures whose ways are different, we must make generalizations with caution. We leave the subject with many questions still unasked, let alone answered.
We now have the awareness, the consciousness, necessary to look at our history, at the ways we have been explained in the past, at the common events of our lives, and at the impact upon us of social and cultural beliefs, attitudes, and practices. Such observation and analysis can provide us with the questions that need to be asked, questions whose answers lie in the research of the future.
The past few years have seen the growth of a feminist scholarship that is especially sensitive to issues and problems in the area of the psychology of women.
Feminist scholarship has its roots in the women’s liberation movement, thus its concerns are in some ways different from those of mainstream psychology. In 1979 Mary Brown Parlee in a review article on the psychology of women described four kinds of feminist work currently underway in the held: (1) critiques of traditional research on women; (2) empirical research from a feminist perspective; (3) theoretical contributions to psychology; and (4) theoretical contributions to problem-centered research. These kinds of scholarly effort continue to enrich our knowledge of the psychology of women today. A brief description of each with examples from the research of the 1980s will convey a sense of both the variety and the quality of feminist-inspired work that has changed the face of psychology.
Critiques of traditional research in psychology are intended to critically reevaluate and reexamine the data, to see what conclusions, on balance, they support, and to “set the record straight.” This is an especially vital function when past research has been used to make policy decisions affecting women. An example is Ruth Bleier’s Science and Gender (1984), a critique of biological theories about women as explanations for their universal subordination to men. Bleier calls such appeals to anatomy as destiny “patriarchal science,” and accuses patriarchal science of providing the intellectual structure that supports the subordination of women that is required by patriarchal institutions. Whenever traditional bodies of research have been used to support the differential treatment of women, to constrict their lives in any way, they are open to review and critique by feminist scholars.
Feminist psychologists have been especially active in generating new research and addressing questions that come out of a feminist awareness. An example is a study of intimacy motivation in women and men, which found that for women but not for men sharing of personal concerns is experienced as a source of strength and growth. Intimate sharing was normative for the women, whereas only those men with very high self-esteem could afford to imagine themselves violating the important male norm of self-reliance by exposing themselves in intimate sharing with others (Mark and Alper, 1985). Such studies give important insights into male-female differences, insights that can illumine hitherto hidden sources of misunderstanding and conflict.
New theoretical perspectives have been developed that have greatly enriched our understanding of women’s behavior. Noteworthy is Carol Gilligan’s (1982) theoretical work on women’s moral development, a research area typically neglected in the moral research literature, which had earlier found that women were “different” and dismissed their differences as evidence of inferiority.
Lastly, feminist scholars have contributed theory and research to problem areas that are peripheral to mainstream psychology as it is currently constituted, problems such as pornography and aggression against women (Henley, 1985). As Parlee points out, these are problems that cannot be adequately simulated in the laboratory; their study thus requires the use of different methodologies from those preferred by traditional laboratory psychologists. Women researchers are looking to their own experience to generate hypotheses in such areas as, for example, male-female relationships, motherhood, and the politics of housework. Some are urging a return to more naturalistic forms of observation, such as the study of letters and journals. Human behavior does not occur independently of its setting in everyday life; one cannot hope to understand the behavior of an individual without knowledge of the situational context within which it occurs (Wallston, 1979). This is of special importance to the psychology of women since, as we noted in the beginning of this book, no understanding of the behavior of women is possible without attention to its history and its social and cultural context.
For all of us, this is the best time ever to understand and to experience our identities as women. We are living longer and healthier lives; we are receiving better educations and career opportunities; we have more and freer choices of ways to live; and we are more liberated than ever before from our dependencies and from the exigencies of our bodies. All of these changes portend interesting possibilities for those of us who are growing up female in today’s world.
[Back Matter]
References
ABRAMOWITZ, S. I., ABRAMOWITZ, C. V., JACKSON, C., and GOMES, B. The politics of clinical judgment: What nonliberal examiners infer about women who don’t stifle themselves. Journal of Consulting and Clinical Psychology 41 (1973): 385–91.
abu-laban, s. m. Women and aging: A futurist perspective. Psychology of Women Quarterly 6 (1981): 85—98.
adams, E., and briscoe, m. l., eds. Up against the wall, mother.... Beverly Hills, Calif.: Glencoe, 1971.
addelson, K. p. Words and lives. Signs: Journal of Women in Culture and Society 7 (1981): 187–99.
adler, a. Understanding human nature. New York: Greenberg, 1927.
adler, F. Sisters in crime. New York: McGraw-Hill, 1975.
aguirre, b. E. Why do they return? Abused wives in shelters. Social Work 3 (1985): 350–54.
albert, e. m. The roles of women: A question of values. In Farber, S. M., and Wilson, R. H. L., eds., The potential of woman. New York: McGraw-Hill, 1963.
albin, r. s. Psychological studies of rape. Signs: Journal of Women in Culture and Society 3 (1977): 423—35.
allen, p. Free choice: A perspective on the small group in women’s liberation. Washington, N.J.: Times Change Press, 1970.
allport, G. w. Pattern and growth in personality. New York: Holt, Rinehart and Winston, 1961.
allport, g. w. Letters from Jenny. New York: Harcourt Brace Jovanovich. 1965.
allport, G. w.; vernon, P. e. A test for personal values. Journal of Abnormal and Social Psychology 26 (1931): 231—48.
allport, g. w.; vernon, p.e.; and lindzey, g. Study of values manual. Boston: Houghton Mifflin, 1960.
American psychiatric association. Diagnostic and statistical manual, 1968, 1980.
annas, j. Mill and the subjection of women. Philosophy 52 (1977): 179—94. asher, j. Sex bias found in therapy. APA Monitor (April 1975): 1, 5.
astin, h. s. The woman doctorate in America. New York: Russell Sage Foundation, 1969.
auden, w. H., and pearson, n. h. Poets of the English language. New York: Viking, 1950.
auerback, a. e. Understanding sexual deviations. Postgraduate Medicine 43 (1968): 169–73.
bakan, d. The duality of human existence. Chicago: Rand McNally, 1966.
baker, s. w. Biological influences on human sex and gender. Signs: Journal of Women in Culture and Society 6 (1980): 80—96.
Balkan, s., berger, r. j., and schmidt, j. Crime, deviance and the American way: a political economic approach. Belmont, Calif.: Wadsworth, 1980.
ballou, m. and gabalac, n. w. A feminist position on mental health. Springfield, Ill.: Charles C Thomas, 1985.
Bandura, a. Influence of models’ reinforcement contingencies on the acquisition of imitative responses. Journal of Personality and Social Psychology 1 (1965): 589–95.
bandura, a. Social learning theory of identificatory processes. In Goslin, D. A., ed., Handbook of socialization theory and research. Chicago: Rand McNally, 1969.
bandura, a., grusec, j. e., and menlove, F. L. Observational learning as a function of symbolization and incentive set. Child Development 37 (1966): 499–506.
bandura, a., ross, D., and ross, s. a. Transmission of aggression through imitation of aggressive models. Journal of Abnormal and Social Psychology 63 (1961): 575–82.
barash, d. The whispering within. New York: Harper and Row, 1979.
bardwick, j. Psychology of women. New York: Harper, 1971.
bardwick, j. Psychological factors in the acceptance and use of oral contraceptives. In Fawcett, J. T., ed., Psychological perspectives on population. New York: Basic Books, 1973.
barglow, p., gunther, m. s., Johnson, a., and meltzer, h. j. Hysterectomy and tubal ligation: a psychiatric comparison. Obstetrics and Gynecology 25 (1965): 520–27.
barness, l. a. Breast milk for all. Nerv England Journal of Medicine 297 (1977): 939–49.
barnett, r. c. and baruch, g. k. Women in the middle years: a critique of research and theory. Psychology of Women Quarterly 3 (1979): 187–97.
barrett, c. j. Intimacy in widowhood. Psychology of Women Quarterly 5 (1981): 473–87.
barry, h., bacon, M. K., and child, i. L. A cross-cultural survey of some sex differences in socialization. Journal of Abnormal and Social Psychology 55 (1957): 327–32.
bart, p. Depression in middle-aged women. In Gornick, V., and Moran, B. K., eds., Woman in sexist society. New York: Basic Books, 1971.
bart, p. b. and grossman, M. Menopause. In Notman, M. T. and Nadelson, C. C., eds., The woman patient: medical and psychological interfaces. New York: Plenum, 1978.
BARUCH, G., BARNETT, r. , and rivers, c. Lifeprints: New patterns of love and work for today’s women. New York: New American Library, 1983.
baruch, G. k. Sex-role attitudes of fifth-grade girls. In Stacey, J.: Beraud, S.; and Daniels, J., eds., And Jill came tumbling after: Sexism in American education. New York: Dell, 1974.
bates, j. e., and zawadzki, E. s. Criminal abortion. Springfield, 111.: Gharles C Thomas, 1964.
Baumrind, d. From each according to her ability. Schoo! Review 80 (1972): 161–97.
beach, f. a., ed. Sex and behavior. New York: Wiley, 1965.
beach, f. a. Hormonal effects on socio-sexual behavior in dogs. In Gibian, H., and Plotz, E. J., eds., Colloquium der Gesellschaft für Biologische Chemie. New York: Springer, 1970.
beckf.r, e. Social science and psychiatry: The coming challenge. The Antioch Review 23 (1963): 353–65.
becker. e. The revolution in psychiatry. Glencoe, III.: The Free Press, 1964.
beecher, c., and stowe, h. b. The American woman’s home: Or, principles of domestic science. New York: J. B. Ford, 1869.
bell, a. p. and Weinberg, m. s. Homosexualities: a study of diversity among men and women. New York: Simon and Schuster, 1978.
bell, a. p., weinberg, m. s., and hammersmith, s. k. Sexual preference: Its development in men and women. Bloomington, Ind.: Indiana University Press, 1981.
bell, j. n. Rescuing the battered wife. Human Behavior, June, 1977.
bell, Q. Virginia Woolf: A biography. New York: Harcourt Brace Jovanovich, 1972.
bell, r. q. Relations between behavior manifestations in the human neonate. Child Development ?>\ (1960): 463–77.
bell, r. q., and Costello, n. s. Three tests for sex differences in tactile sensitivity in the newborn. Biologia Neonaturum 7 (1964): 335—47.
bello, f. The magic that made Polaroid. Fortune 59 (1959): 124–29.
bem, s. l. The measurement of psychological androgyny. Journal of Consulting and Clinical Psychology 42 (1974): 155—162.
benbow, c. p. and Stanley, j. c. Sex differences in mathematical reasoning ability: More facts. Science, Dec. 2, 1983, 1029—31.
benedek, t. f. Sexual functions in women and their disturbance. In Ariete, S., ed., American handbook of psychiatry, vol. 1. New York: Basic Books, 1959.
benditt, j. m. Current contraceptive research. Family Planning Perspectives 12 (1980): 149–55.
berger, d. g. and wenger, m. G. The ideology of virginity. Journal of Marriage and the Family, November, 1973, 666—76.
bermant, g. Behavior therapy approaches to modification of sexual preference: Biological perspective and critique. In Bardwick, J., cd., Readings on the psychology of women. New York: Harper & Row, 1972.
Bernard, j. The paradox of the happy marriage. In Gornick, V., and Moran, B. K., eds., Woman in sexist society. New York: Basic Books, 1971. (a)
Bernard, j. Women and the public interest: An essay on policy and protest. New York: Aldine-Atherton, 1971. (b)
Bernard, j. The future of motherhood. New York: Dial, 1974.
Bernard, j. Sex differences: An overview. New York: MSS Modular Publications, Inc., Moduls 26, 1974, 1 — 18.
berry, j. w. Temne and Eskimo perceptual skills. International Journal of Psychology 1 (1966): 207–29.
bettelheim, b. The commitment required of a woman entering a scientific profession in present-day American society. In Mattfield, J. A., and Van Akan, C. G., eds., Women and the scientific professions. Cambridge, Mass.: M.I.T. Press, 1965.
bibring, G. l. Some specific psychological tasks in pregnancy and motherhood. In Hammer, S., ed., Women: Body and culture. New York: Harper & Row, 1975.
bird, c. The best years of a woman’s life. Psychology Today, June, 1979, 20— 26.
birley, j. l. T. Early diagnosis of schizophrenia. British Medical Journal no. 5625 (1968): 232–34.
birren, j. e. The psychology of aging. Englewood Cliffs, N.J.: Prentice-Hall, 1964.
bishop, s. and weinzweig, m. Philosophy and women. Belmont, Calif.: Wadsworth, 1979.
blackwell, j. e. The black community. Second Edition. New York: Harper and Row, 1985.
bleier, r. Science and gender. New York: Pergamon Press, 1984.
blinick, g. Menstrual function and pregnancy in narcotics addicts treated with methadone. Nature (London) 219 (1968): 180.
bloch, d. a. Sex crimes and criminals. American Journal of Nursing 53 (1953): 440–43.
block, h. a., and niederhoffer, a. The gang: A study in adolescent behavior. New York: Philosophical Library, 1958.
block, j. h. Conceptions of sex role: Some cross-cultural and longitudinal perspectives. American Psychologist 28 (1973): 512—26.
block, J. h. Debatable conclusions about sex differences. Contemporary Psychology 21 (1976): 517–22.
blume, j. Are you there God? It’s me, Margaret. New York: Bradburg, 1970.
blumstein, p. and schwartz, p. American couples. New York: William Morrow, 1983.
bock, w. e. Farmer’s daughter effect: The case of the Negro female professional. Phylon 30 (1969): 17–26.
boles, d. b. X-linkage of spatial ability: A critical review. Child Development 51 (1980): 625–35.
bolter, s. The psychiatrist’s role in therapeutic abortions; The unwitting accomplice. American Journal of Psychiatry 119 (1962): 312—16.
boskind-white, m. and white, w. c. Bulimarexia: The binge I purge cycle. New York: Norton, 1983.
boston women’s health coi.LECTivE. The new our bodies, our selves. New York: Simon and Schuster, 1984.
bowker, l. h., gross, h. s., and klein, m. w. Female participation in delinquent gang activities. Adolescence 15 (1980): 509—19.
bowlby, j. Grief and mourning in infancy and early childhood. In The psychoanalytic study of the child, vol. 15. New York: International Universities Press, 1960.
bowlby, j. Attachment. New York: Basic Books, 1969.
BRAINE, M. D. S., HEIMER, C. B., WORTIS, H., aild FREEDMAN, A. M. Factors associated with impairment of the early development of prematures. Monographs of the Society for Research in Child Development 31 (1966): serial No. 106.
brecher, e. m. The sex researchers. San Francisco: Specific Press, 1979.
breines, w. and Gordon, l. The new scholarship on family violence. Signs: Journal of Women in Culture and Society 8 (1983): 490—531.
breit, e. b. and ferrandino, m. m. Social dimensions of the menstrual taboo and the effects on female sexuality. In Williams, J. H., ed., Psychology of women: selected readings. New York: Norton, 1979.
brockett, l. p. Woman: Her rights, wrongs, privileges and responsibilities. Freeport, N.Y.: Books for Libraries Press, 1869.
brodsky, a. m. A decade of feminist influence on psychotherapy. Psychology of Women Quarterly 4 (1980): 331—44.
brodsky, c. m. The pharmacotherapy system. Psychosomatics 11 (1971): 24— 30.
brody, j. e. As breast-feeding advantages mount up, women switch over. St. Petersburg Times, June 16, 1977.
BROVERMAN, I. K., BROVERMAN, D. M., CLARKSON, F. E., ROSENKRANTZ, P. S., and vogel, s. r. Sex-role stereotypes and clinical judgments of mental health. Journal of Counsulting and Clinical Psychology 34 (1970): 1–7.
BROVERMAN, I. K., VOGEL, S. R., BROVERMAN, D. M., CLARKSON, F. E., and ROSENKRANTZ, p. s. Sex-role stereotypes: A current appraisal. Journal of Social Issues 28 (1972): 59–78.
brown, d. g. Sex-role development in a changing culture. Psychological Bulletin 4 (1958): 232–42.
brown, d. g., and lynn, d. b. Human sexual development: An outline of components and concepts. Journal of Marriage and the Family 28 (1966): 155–62.
brown, G. w., bhrolchain, m. n., and Harris, t. Social class and psychiatric disturbance among women in an urban population. Sociology 9 (1975): 225–54.
brown, j. c. Immodest acts. New York: Oxford, 1986.
brown, l. r. In the human interest. New York: Norton, 1974.
brown, w. a., and shereshefsky, p. Seven women: A prospective study of postpartum psychiatric disorders. Psychiatry, 35 (1972).
brownmiller, s. The mass psychology of rape. In Ruth, S., ed., Issues in feminism. Boston: Houghton Mifflin, 1980.
brownmiller, s. Against our will: Men, women, and rape. New York: Simon and Schuster, 1975.
bryson, r., bryson, j. b., and Johnson, m. f. Family size, satisfaction, and productivity in dual-career couples. Psychology of Women Quarterly 3 (1978): 67–77.
bullough, v. l. The subordinate sex: A history of attitudes toward women. Urbana, Ill.: University of Illinois Press, 1973.
burgess, a. w. and holstrom, L. Rape trauma syndrome and post traumatic stress response. In A. W. Burgess, ed., Rape and sexual assault: A research handbook. New York: Garland, 1985.
burlew, a. k. The experience of black females in traditional and nontraditional professions. Psychology of Women Quarterly 6 (1982): 312–26.
cade, T., ed., The black woman. New York: New American Library, Signet, 1970.
Calderone, m. a., ed. Manual of family planning and contraceptive practice. Baltimore: Williams & Wilkins, 1970.
Calvert, r. Criminal and civil liability in husband-wife assaults. In Steinmetz, S. and Straus, M., eds., Violence in the family. New York: Dodd, Mead, 1975.
Cameron, m. Family relationships. In No longer young. Work Group Reports from the 26th Annual Conference on Aging, Institute of Gerontology, University of Michigan and Wayne State University, 1974.
Campbell, a. Subjective measures of well-being. American Psychologist 31 (1976): 117–24.
Campbell, j. The masks of God: Primitive mythology. New York: Viking, 1959.
caplan, p. j. Beyond the box score: a boundary condition for sex differences in aggression and achievement striving. Progress in Experimental Personality Research 9 (1979): 41—87.
caplan, p. j., macpherson, G. m., and tobin, p. Do sex-related differences in spatial abilities exist? A multilevel critique with new data. American Psychologist 40 (1985): 786—99.
carlson, e. R., and Carlson, r. Male and female subjects in personality research. Journal of Abnormal and Social Psychology 61 (1961): 482—83.
carlson, r. Where is the person in personality research? Psychological Bulletin 3 (1971): 203–19.
carlson, R. Understanding women: Implications for personality theory and research. Journal of Social Issues 28 (1972): 17—32.
cartwright, l. k. Personality differences in male and female medical students. Psychiatry m Medicine 3 (1972): 213—18.
cash, w. j. The mind of the South. New York: Random House, 1960.
cassem, n. Bereavement as indispensable to growth. In B. Schoenberg et al., eds., Bereavement: Its psychosocial aspects. New York: Columbia University Press, 1975.
castle, c. s. A statistical study of eminent women. New York: Science Press, 1913.
chadwick, m. The psychology of menstruation. Washington, D. C.: Nervous and Mental Diseases Publishing Co., 1932.
chamov, a., harlow, h. F., and mitchell, G. d. Sex differences in the infant-directed behavior of preadolescent rhesus monkeys. Child Development 38 (1967): 329–35.
chasseguet-smirgel, j., ed., Female, sexuality. Ann Arbor, Mich.: University of Michigan Press, 1970.
chen, p. Translator’s introduction: Birth planning in China. Family Planning Perspectives 11 (1979): 348—54.
chesler, p. Patient and patriarch: Women in the psychotherapeutic relationship. In Gornick, V., and Moran, B. K., eds., Women in sexist society. New York: Basic Books, 1971.
chesler, p. Women and madness. Garden City, N.Y.: Doubleday, 1972.
chesney-lind, m. Juvenile delinquency: The sexualization of female crime. Psychology Today 8 (1974): 43—46.
ching, c. c. The one-child family in China: The need for psychosocial research. Studies in Family Planning 13 (1982): 208—12.
chodorow, n. The reproduction of mothering: psychoanalysis and the sociology of gender. Berkeley: University of California Press, 1978.
CLARKSON, F. E., VOGEL, S. R., ROVERMAN, I. K., BROVERMAN, D. M., and Rosenkrantz, p. s. Family size and sex-role stereotypes. Science 167 (1970): 390–92.
clemens, l. g., shryne, j., and gorski, r. a. Androgen and development of progesterone responsiveness in male and female rats. Physiology and Behavior, 1970, 5, 673—78.
coffin, p. The young unmarrieds. In DeLora, J. S., and DeLora, J. R., eds., Intimate life styles. Pacific Palisades, Calif.: Goodyear, 1972.
cohen, d. and wilkie, f. Sex-related differences in cognition among the elderly. In Wittid, M. A. and Petersen, A. C., eds., Sex-related differences in cognitive functioning. New York: Academic Press, 1979.
COHEN, M. L., GAROFALO, R., BOUCHER, R., and SEGHORN, T. The psychology of rapists. Seminars in Psychiatry 3 (1971): 307—27.
Constantine, l. l., and Constantine, j. m. Group and multilateral marriage: Definitional notes, glossary, and annotated bibliography. Family Process 10 (1971): 157–76.
Constantine, l. l., and Constantine, j. m. Sexual aspects of multilateral relations. In Smith, J. R., and Smith, L. G., eds., Beyond monogamy. Baltimore: The Johns Hopkins University Press, 1974.
Constantinople, a. Sex-role acquisition: In search of the elephant. Sex Roles 5 (1979): 121–33.
cook, b. w. “Women alone stir my imagination”: Lesbianism and the cultural tradition. Signs: Journal of Women in Culture and Society 4 (1979): 718–39.
cook, e. p. Psychological androgyny. New York: Pergamon, 1985.
cooperstock, r. Sex differences in the use of mood-modifying drugs: An explanatory model. Journal of Health and Social Behavior 12 (1971): 238–44.
cowan, g., warren, l. w., and young, j. l. Medical perceptions of menopausal symptoms. Psychology of Women Quarterly 9 (1985): 3–14.
crocker, p. l. An analysis of university definitions of sexual harassment. Signs: Journal of Women in Culture and Society 8 (1983): 696–707.
crovitz, e. and steinmann, A. A decade later: Black-white attitudes toward
women’s familial roles. Psychology of Women Quarterly 5 (1980): 170—76.
CUTLER, R., HEIMER, C. B., WORTIS, H., and FREEDMAN, A. M. The effects of prenatal and neonatal complications on the development of premature children at two-and-one-half-years of age. Journal of Genetic Psychology 107 (1965): 261–76.
dalton, k. Effects of menstruation on schoolgirls’ weekly work. British Medical Journal 1 (1960): 326—28.
dalton, k. Discussion on depression: Emotion or illness. Practitioner, 206 (1971): 681–83.
daly, m. The church and the second sex. New York: Harper & Row, 1975.
Daniels, p. Dream vs. drift in women’s careers: The question of generativity. In B. L. Forisher and B. H. Goldman, eds., Outsiders on the inside: Women and organizations. Englewood Cliffs, N.J.: Prentice-Hall, 1981.
danza, r. Menarche: Its effects on mother-daughter and father-daughter interactions. In S. Golub, ed., Menarche. Lexington, Mass.: D.C. Health, 1983.
david, c. A masculine mythology of femininity. In Chasseguet-Smirgel, J., ed., Female sexuality. Ann Arbor, Mich.: University Michigan Press, 1970.
david, h. p. Psychological studies in abortion. In Fawcett, J. T., ed., Psychological perspectives on population. New York: Basic Books, 1973.
davidson, c. v. and abramowitz, s. i. Sex bias in clinical judgment: later empirical returns. Psychology of Women Quarterly 4 (1980): 377—95.
davis, K. Factors in the sex life of twenty-two hundred women. New York: Harper and Row, 1929.
deaux, k. From individual differences to social categories: Analysis of a decade’s research on gender. American Psychologist 39 (1984): 105–16.
de beauvoir, s. The second sex. New York: Knopf, 1953.
de beauvoir, s. Joie de vivre. Harper’s Magazine, January 1972, 33—40.
deegan, d. y. The stereotype of the single woman tn American novels. New York: Kings Crown Press, 1951.
delaney, j., lupton, m. j., and toth, e. The curse: a cultural history of menstruation. New York: Dutton, 1976.
delora, j. s., and delora, j. r. eds., Intimate life styles: Marriage and its alternatives. Pacific Palisades, Calif.: Goodyear, 1972.
de rougemont, d. Love in the western world. New York: Pantheon, 1956.
deutsch, f. A footnote to Freud’s “Fragment of an analysis of a case of hysteria.” The Psychoanalytic Quarterly 25 (1957): 159–67.
deutsch, h. The significance of masochism in the mental life of women. International Journal of Psychoanalysis 11 (1930): 48—60.
deutsch, h. The psychology of women: A psychoanalytic interpretation, vol. 1. New York: Grune & Stratton, 1944.
deutsch, h. The psychology of women: A psychoanalytic interpretation, vol. 2. New York: Grune & Stratton, 1945.
deutsch, h. On female homosexuality (1933). In Ruitenbeek, H., ed., Psychoanalysis and female sexuality. New Haven, Conn.: College and University Press, 1966.
deutsch, h. Confrontations with myself. New York: Norton, 1973.
deutscher, i. The quality of postparental life. In Neugarten, B., cd., Middle age and aging. Chicago: University of Chicago Press, 1968.
de vore, i., ed., Primate behavior: Field studies of monkeys and apes. New York: Holt, Rinehart and Winston, 1965.
dewey, J. Human nature and conduct. New York: Modern Library, 1930.
diamond, I. Pornography and repression: A reconsideration. Signs: Journal of Women in Culture and Society 5 (1980): 686—701. dick-read, g. Childbirth without fear. New York: Harper & Brothers, 1944.
Dickinson, r. l. Alias of human sexual anatomy (1933) 2d ed. Baltimore: Williams & Wilkins, 1949.
Dickinson, r. l., and beam, L. A thousand marriages. Baltimore: Williams & Wilkins, 1932.
Dickinson, r. l. and beam, l. The single woman. Baltimore: Williams & Wilkins, 1934.
diner, h. Mothers and Amazons: The first feminine history of culture. Garden City, N.Y.: Anchor, 1973.
Dipietro, j.a. Rough and tumble play: A function of gender. Developmental Psychology 17 (1981): 50—58.
DIXON, r. b. Women’s rights and fertility. Reports on Population I Family Planning. The Population Council, 245 Park Avenue, New York, N.Y. January, 1975.
doherty, m. a. Sexual bias in personality theory. The Counseling Psychologist 4 (1973): 67–74.
douvan, e. New sources of conflict in females at adolescence. In Bardwick, J. M.; Douvan, E.; Horner, M. S.; and Gutmann, D. Feminine personality and conflict. Belmont, Calif.: Brooks/Cole, 1970.
dowty, n. To be a woman in Israel. School Review 80 (1972): 319—32.
Duffy, E. Activation and behavior. New York: Wiley, 1962.
durant, w. The story of philosophy. New York: Simon and Schuster, 1953.
eagen, a. b. The new pill: Should you take it? MS, October 1985.
eckholm, e. and newland, k. Health: The family planning factor. World watch Paper 10. Worldwatch Institute, Washington, D. C., 1977.
ehrhardt, a. a. and meyer-bahlburg, h. F. L. Effects of prenatal sex hormones on gender-related behavior. Science 211 (1981): 1312—18.
eitner, l. The erotic in art. In Katchadourian, H. A. and Lunde, D. T., eds., Fundamentals of human sexuality. New York: Holt, Rinehart and Winston, 1975.
ellis, H. Sexual inversion in women. Alienist and Neurologist 16 (1895): 141 — 58.
ellis, h. Studies in the psychology of sex. New York: Random House, 1936.
emlen, a. c., and perry, j. B., jr. Child-care arrangements. In Hoffman, L. W., and Nye, F. I., eds., The working mother. San Francisco: Jossey-Bass, 1974.
English, j. Philosophy. Signs: Journal of Women in Culture and Society 3 (1978): 823–31.
Enoch, m. d., trethowan, w. h., and barker, j. c. The couvade syndrome. In Enoch, M. P., ed., Some uncommon psychiatric syndromes. Bristol: John Wright and Sons, 1967.
erhardt, a., Greenberg, N., and money, j. Female gender identity and absence of fetal hormones: Turner’s syndrome. Johns Hopkins Medical Journal 125 (1970): 237–48.
erikson, e. h. Chilhood and society. New York: Norton, 1963.
erikson, e. h. Womanhood and the inner space. In Identity: youth and crisis. New York: Norton, 1968.
erikson, e. h. Identity: Youth and crisis. New York: Norton, 1968.
ERIKSON, E. h. Once more the inner space. In Life history and the historical moment. New York: Norton, 1975.
erickson, m. t. Relationship between psychological attitudes during pregnancy and complications of pregnancy, labor, and delivery. Proceedings of the 73rd Annual Convention of the American Psychological Association, 1965, 213–14.
eron, l. d. Prescription for reduction of aggression. American Psychologist 35 (1980): 244–52.
estellachild, v. Hippie communes. In DeLora, J. S., and DeLora, J. R., eds., Intimate life styles: Marriage and its alternatives. Pacific Palisades, Calif.: Goodyear, 1972.
fabrikant, b. The psychotherapist and the female patient: Perceptions, misconceptions and change. In Franks, V., and Burtle, V., eds., Women in therapy. New York: Brunner / Mazel, 1974.
faderman, L. Surpassing the love of men. New York: William Morrow, 1981.
fancher, R. e. Psychoanalytic psychology New York: Norton, 1973.
feinman, c. Sex role stereotypes and justice for women. Crime and Delinquency 25 (1979): 87–94.
female offender resource center. American Bar Association, Washington, D.C., 1976.
fenichel, o. The psychoanalytic theory of neuroses. New York: Norton, 1945.
fennema, e. h. and Sherman, j. Sex-related differences in mathematics achievement and related factors: A further study. Journal for Research in Mathematics Education 9 (1978): 189—203.
ferguson, a. Patriarchy, sexual identity, and the sexual revolution. Signs: Journal of Women in Culture and Society 7 (1981): 158—72.
ferguson, a. Sex war: The debate between radical and libertarian feminists.
Signs: Journal of Women in Culture and Society 10 (1984): 106—12.
ferguson, a., zita, j. n., and addelson, k. p. On “Compulsory heterosexuality and lesbian existence”: Defining the issues. Signs: Journal of Women in Culture and Society 7 (1981): 158—99.
fesbach, n. d. Sex differences in children’s modes of aggressive responses — toward outsiders. Merrill Palmer Quarterly 15 (1969): 249—58.
fesbach, s. Aggression. In Mussen, P. F., ed., Carmichael’s manual of child psychology. New York: Wiley, 1970.
fidell, L. s. Put her down on drugs: Prescribed drug usage in women. Paper read at the Western Psychological Association Meeting, Anaheim, Calif., April 2, 1973.
fidell, l. s. Sex role stereotypes and the American physician. Psychology of Women Quarterly 4 (1980): 313—30.
figes, e. Patriarchal attitudes. London: Faber and Faber, 1970.
FiNGERER, m. e. Psychological sequelae of abortion: Anxiety and depression. Journal of Community Psychology 1 (1973): 221–25.
fish, s. l. A phenomenology of women. Unpublished Doctoral Dissertation, Southern Illinois University, 1975.
fisher, s. The female orgasm. New York: Basic Books, 1973.
fishman, l. t. Aspiration and delinquency: The case of Negro girls. Unpublished master’s thesis, University of Chicago, 1966.
ford, c. s., and beach, f. a. Patterns of sexual behavior. New York: Harper, 1951.
forrest, j. d. and henshaw, s. K. What U.S. women think and do about contraception. Family Planning Perspectives 15 (1983): 157—66.
fox, l. h., tobin, d., and brody, l. Sex-role socialization and achievement in mathematics. In Wittig, M. A. and Petersen, A. C., eds., Sex-related differences in cognitive functioning. New York: Academic Press, 1979.
franks, v., and burtle, v. Women in therapy. New York: Brunner/ Mazel, 1974.
franzwa, h. h. Female roles in women’s magazine fiction. In Unger, R. K., and Denmark, F. L., eds., Woman: Dependent or independent variable New York: Psychological Dimensions, 1975.
Frazer, j. g. The golden bough. New York: Macmillan, 1951.
freedman, e. b. and thorne, b. Introduction to “The feminist sexuality debates.” Signs: Journal of Women m Culture and Society 10 (1984): 102—5.
freedman, r. Beauty bound. Lexington, Mass.: Heath, 1986.
FRiEDAN, b. The feminine mystique. New York: Norton, 1963.
friedan, b. The second stage. New York: Summit Books, 1981.
Freud, s. Femininity (1933). In Strachey, J., tr. and ed.. New introductory lectures on psychoanalysis. New York: Norton, 1965.
freud, s. An outline of psycho-analysis (1939), edited and translated by J. Strachey. New York: Norton, 1970.
freud, s. “Civilized” sexual morality and modern nervous illness (1908). In Strachey, J., tr. and ed., The complete psychological works, vol. IX. New York: Norton, 1976a.
freud, s. Female sexuality (1931). In Strachey, J., tr. and ed., The complete psychological works, vol. XXL New York: Norton, 1976b.
freud. s. Fragment of an analysis of a case of hysteria (1905). In Strachey, J., tr. and ed., The complete psychological works, vol. VIL New York: Norton, 1976c.
freud, s. The infantile genital organization (1923). In Strachey, J., tr. and cd., The complete psychological works, vol. XIX. New York: Norton, 1976d.
freud, s. The psychogenesis of a case of homosexuality in a woman (1920). In Strachey, J., tr. and ed., The complete psychological works, vol. XVIII. New York: Norton, I976e.
freud, s. The question of lay analysis (1926). In Strachey, J., tr. and ed., The complete psychological works, vol. XX. New York: Norton, 1976f.
freud, s. The sexual aberrations (1905). In Strachey, J., tr. and ed., The complete psychological works, vol. VIL New York: Norton, 1976g.
freud, s. Some psychical consequences of the anatomical distinction between the sexes (1925). In Strachey, J., tr. and ed., The complete psychological works, vol. XIX. New York: Norton, 1976h.
freud, s. Three essays on the theory of sexuality (1905). In Strachey, J., tr. and ed., The complete psychological works, vol. VIL New York: Norton, 1976Ì.
freud. s., and breuer, j. Studies in hysteria (1895). New York: Avon Books, 1966.
Friday, n. My mother ! myself. New York: Delacorte, 1977.
Frisch. R. e. Fatness, menarche, and fertility. In Golub, S., ed., Menarche. Lexington, Mass.: D.C. Heath, 1983.
frodi, a., macauley, j., and thome, p. r. Are women always less aggressive than men? A review of the experimental literature. Psychological Bulletin. 84 (1977): 634–60.
fromm-reichman, f., and gunst, v. K. On the denial of women’s sexual pleasure (1950). In Miller, J. B., ed., Psychoanalysis and women. New York: Brunner / Mazcl, 1973.
Fuchs, e. The second season: life, love, and sex for woman in the middle years. Garden City, N.Y.: Anchor / Doubleday, 1978.
furtmüller, c., Alfred Adler: A biographical essay. In Ansbacher, H. L. and Ansbacher, R. R., eds., Superiority and social interest. Evanston, Ill.: Northwestern University Press, 1964.
galdston, i. Other aspects (psychiatric) of the abortion problem. In Calderone, M., ed.. Abortion in the U.S. New York: Hoeber-Harper, 1958.
GARAI, J. e., Sex differences in mental health. Genetic Psychology Monographs 81 (1970): 123–42.
garai, j. e., and Scheinfeld, a. Sex differences in mental and behavioral traits. Genetic Psychology Monographs 77 (1968): 162—299.
gelles, r. j. The violent home. Beverly Hills: Sage, 1974.
gerson, m-j. The lure of motherhood. Psychology of Women Quarterly 5 (1980): 207–18.
gerson, m-j, alpert, j. l. and richardson, m. s. Mothering: The view from psychological research. Signs: Journal of Women in Culture and Society 9 (1984): 434–53.
giallombardo, R. Society of women: A study of a women’s prison. New York: Wiley, 1966.
giallombardo, r. The social world of imprisoned girls. New York: Wiley, 1974. gibson, l. Experts fret as boys dominate computer training. The Tampa Tribune, July 5, 1985.
gilbert, s. m. and gubar, s. The Norton anthology of literature by women. New York: Norton, 1985.
gilkes, c. t. Successful rebellious professionals: The black woman’s professional identity and community commitment. Psychology of Women Quarterly 6 (1982): 289–311.
Gillespie, d. l. Who has the power? The marital struggle. In Freeman, J., ed., Women: A feminist perspective. Palo Alto, Calif: Mayfield, 1975.
gilligan, c. In a different voice. Cambridge: Harvard University Press, 1982.
Gilligan, c. In a different voice: women’s conceptions of self and morality. Harvard Educational Review 47 (1977): 481—517.
glazer-malbin, n. Housework. Signs: Journal of Women in Culture and Society 1 (1976): 905–22.
Goldberg, s., and lewis, m. Play behavior in the year-old infant: Early sex differences. Child Development 40 (1969): 21—31.
Goldfarb, w. Childhood psychosis. In Mussen, P. H., ed., Carmichael’s manual of child psychology. New York: Wiley, 1970.
GOLDFOOT, D., WALLEN, K., NEFF, D. A., MCBRA1R, M. C., and GOY, R. W. Social influences upon the display of sexually dimorphic behavior in rhesus monkeys: isosexual rearing. Archives of Sexual Behavior 13 (1984): 395— 412.
Goldstein, l. Sexual harassment on the job: when the working relationship gets out of hand. The Floridan, St. Petersburg Times, March 9, 1980.
golub, s. The decision to breast-feed: personality and experiential influences. Psychology: A Journal of Human Behavior 15 (1978): 17—27.
golub, s. The effect of premenstrual depression and anxiety on personality and cognitive function. Summary of Unpublished Doctoral Dissertation, Fordham University, 1973.
golub, s. The magnitude of premenstrual anxiety and depression. Psychosomatic Medicine 38 (1976): 4—12.
golub, s. and Harrington, d. m. Premenstrual and menstrual mood changes in adolescent women. Journal of Personality and Social Psychology 41 (1981): 961–65.
Goodman, m. and Goodman, s. Over the hill. In Miller, L., ed., Fourth International Congress of Social Psychiatry: Abstracts of Papers. Jerusalem: AHVA Cooperative, 1972.
Gordon, r. e., and Gordon, K. k. Factors in postpartum emotional adjustment. American Journal of Orthopsychiatry 37 (1967): 359—60.
GOVE, w. R. Sex, marital status, and suicide. Journal of Health and Social Behavior 13 (1972): 204–13.
GOVE, w. r. Mental illness and psychiatric treatment among women. Psychology of Women Quarterly 4 (1980): 345—62.
gove, w. r., and tudor, j. f. Adult sex roles and mental illness. American Journal of Sociology 78 (1973): 812—35.
goy, r. w., and mcewen, b. s. Sexual differentiation of the brain. Cambridge, Mass.: The MIT Press, 1980.
grady, k. i., and young, w. c. Role of the developing rat testis in differentiation of the neural tissues mediating mating behavior. Journal of Comparative and Physiological Psychology 59 (1965): 176—82.
graebner, d. b. A decade of sexism in readers. Reading Teacher 26 (1972), no. 1: 52–58.
graham, h. The social image of pregnancy: pregnancy as spirit possession. Sociological Review 24 (1976): 291—308.
green, m. r. ed., Interpersonal psychoanalysis: The selected papers of Clara Thompson. New York: Basic Books, 1964.
Greenspan, m. a. A new approach to women and therapy. New York: McGrawHill, 1983.
greer, g. Seduction is a four-letter word. In Schults, L. G., ed., Rape victimology. Springfield, Ill.: Charles C Thomas, 1975.
grimes, d. a. Second-trimester abortions in the United States. Family Planning Perspectives 16 (1984): 260—66.
groth, a.n., and burgess, a. w. Rape: a sexual deviation. American Journal of Orthopsychiatry 47 (1977): 400—406.
grunbaum, a. The foundations of psychoanalysis. Berkeley, Calif.: University of California Press, 1984.
gump, j. p Sex-role attitudes and psychological well-being. Journal of Social Issues 28 (1972): 79–92.
gump, j. p. and rivers, l. w. A consideration of race in efforts to end sex bias. In Diamond, E. E., ed., Issues of sex bias and sex fairness in career interest measurement. Washington, D.C.: Department of Health, Education, and Welfare, National Institute of Education, Spring 1975.
gutmann, d. l. An exploration of ego configurations in middle and late life. In Neugarten, B. L, et al., eds., Personality in middle and late life. New York: Atherton, 1964.
hall, c. s., and lindzey, g. Theories of personality. New York: Wiley, 1970.
hall, e. t., jr. The silent language. New York: Doubleday, 1959.
hall, r. The well of loneliness (1928). New York: Pocket Books, 1950.
haller, j. s., and haller, r. m. The physician and sexuality in Victorian America.
Urbana, Ill.: University of Illinois Press, 1974.
Hamburg, d. a., and lunde, d. t. Sex hormones in the development of sex differences in human behavior. In Maccoby, E. E., ed., The development of sex differences. Stanford, Calif.: Stanford University Press, 1966.
hare-mustin, r. t. An appraisal of the relationship between women and psychotherapy. American Psychologist 38 (1983): 593–601.
harlow, h. The heterosexual affectional system in monkeys. American Psychologist 17 (1962): 1—9.
harlow, h., and harlow, m. The young monkeys. In Readings in psychology today. Del Mar, Calif.: Communications / Research/ Machines, 1967.
harper, r. a. Psychoanalysis and psychotherapy. Englewood Cliffs, N.J.: Prentice-Hall, 1959.
HATCHER, R. a., STEWART, G. K., STEWART, F., GUEST, R., STRATTON, P., and WRIGHT, A. H. Contraceptive technology 1978–1979. New York: Irvington Publishers, 1978.
HATFIELD, j. s.; ferguson, l. r.; and alpert, r. Mother-child interaction and the socialization process. Child Development 38 (1967): 365–414.
hayler, b. Abortion. Signs: Journal of Women in Culture and Society 5 (1979)307–23.
hayner, n. Attitudes toward conjugal visits for prisoners. Federal Probation 36 (1972): 43–49.
heatherington, E. m. A developmental study of the effects of sex of the dominant parent on sex-role preference, identification, and imitation in children. Journal of Personality and Social Psychology 2 (1965): 188–94.
hedgepeth, w. Maybe it’ll be different here. In DeLora, D. S., and DeLora, J. R., eds., Intimate life styles. Pacific Palisades, Calif.: Goodyear, 1972.
heffernan, E. Making it in prison: The square, the cool, and the life. New York: Wiley, 1972.
hefner, r., rebecca, m., and oleshansky, b. Development of sex-role transcendance. Human Development 18 (1975): 143—58.
heilbrun, a. b. Sex role identity in adolescent females: A theoretical paradox. Adolescence 3 (1968): 79–88. (a)
heilbrun, a. B. Sex-role, instrumental-expressive behavior, and psychopathology in females. Journal of Abnormal Psychology 73 (1968): 2, 131–36. (b)
Henley, n. M. Psychology and gender. Signs: Journal of Women in Culture and Society 11 (1985): 101–19.
hennig, m. Family dynamics and the successful woman executive. In Knudsin, R., ed., Women and success. New York: William Morrow, 1973.
hier, d. b. and kaplan, j. Are sex differences in cerebral organization clinically significant? Behavioral and Brain Sciences 3 (1980): 238—39.
Higham, e. Sexuality in the infant and neonate: birth to two years. In Wolman, B. J., and Money, J., eds., Handbook of human sexuality. Englewood Cliffs, NJ.: 1980.
hilberman, e. The impact of rape. In Notman, M. T. and Nadelson, C. C., eds., The woman patient: medical and psychological interfaces. New York: Plenum, 1978.
hill, k. t., and sarason, s. b. The relation of test anxiety and defensiveness to test and school performance over the elementary school years. Monographs of the Society for Research in Child Development 31 (1966): no. 104.
hill, r. Economic policies and black progress: Myths and realities. Washington, D.C.: National Urban League Research Department, 1981.
himes. n. The medical history of contraception. New York: Gamut Press, 1963.
hite, s. The Hite report. New York: Macmillan, 1976.
hoffman, l. w. Mother’s enjoyment of work and effects on the child. In Nye, F. L, and Hoffman, L. W., eds., The employed mother in America. Chicago: Rand McNally, 1963.
hoffman, l. w. Early childhood experiences and women’s achievement motives. Journal of Social Issues 28 (1972): 129—55.
hoffman, l. w., and hoffman, m. l. The value of children to parents. In Fawcett, J. T., ed., Psychological perspectives on population. New York: Basic Books, 1973.
hoffman, l. w., and nye, f. i. Working mothers. San Francisco: Jossey-Bass, 1974.
hogan, d. f., astone, n. M., and kitagawa, e. M. Social and environmental factors influencing contraceptive use among black adolescents. Family Planning Perspectives 17 (1985): 165—69.
hogeland, r. w., ed., Women and womanhood in America. Lexington, Mass. Heath, 1973.
Hollingworth, l. s. Comparison of the sexes in mental traits. Psychological Bulletin 16 (1919): 371–73.
Hollingworth, L. s. Comparison of the sexes in mental traits. Psychological Bulletin 15 (1918): 427–32.
Hollingworth, l. s. Functional periodicity. New York: Teachers College, Columbia University, 1914a.
Hollingworth, l. s. Sex differences in mental traits. Psychological Bulletin 13 (1916): 377–84.
Hollingworth, l. s. Variability as related to sex differences in achievement. American Journal of Sociology 19 (1914b): 510—30.
Hollingworth, l. s. Social devices for impelling wommen to bear and rear children. American Journal of Sociology 22 (1916): 19—29.
horgan, c. M. A comparison of utilization and expenditure patterns for ambulatory mental health services in the specialty mental health and the general sector. Paper presented at the meeting of the American Public Health Association, Montreal, Canada, November 1982.
horner, m. s. Femininity and successful achievement: A basic inconsistency. In Bardwick, J. M.; Douvan, E.; Horner, M. S.; and Gutmann, D., eds., Feminine personality and conflict. Belmont, Calif.: Brooks/Cole, 1970.
horner, m. s. Toward an understanding of achievement-related conflicts in women. In Stacey, J.; Gereaud, S.; and Daniels, J., eds. And Jill came tumbling after: Sexism in American education. New York: Dell, 1974.
horney, k. The neurotic personality of our time. New York: Norton, 1937.
horney, k. Neurosis and human growth. New York: Norton, 1950.
horney, k. Feminine psychology, New York: Norton, 1973.
horney, k. The problem of feminine masochism (1935). In Horney, K.., Feminine psychology. New York: Norton, 1973.
horney, k. The overvaluation of love (1934). In Horney, K., Feminine psychology. New York: Norton, 1973.
horney, k. The flight from womanhood (1926). In Horney, K., Feminine psychology. New York: Norton, 1973.
houseknecht, s. k. Timing of the decision to remain voluntarily childless: evidence for continuous socialization. Psychology of Women Quarterly 4 (1979): 81–96.
Howard, e. m., and Howard, j. l. Women in institutions: Treatment in prisons and mental hospitals. In Franks, V., and Burtle, V., eds., Women in therapy. New York: Brunner / Mazel, 1974.
Howard, s. The silver cord. New York: Charles Scribner’s Sons, 1927.
howell, m. c. What medical schools teach about women. New England Journal of Medicine 291 (1974): 304–7.
hrdy, s. b. The woman that never evolved. Cambridge: Harvard University Press, 1981.
hughes, e. Angry in retirement. Human Behavior 3 (1974): 9, 56—59.
hunt, m. Sexual behavior in the seventies. Chicago: Playboy Press, 1974.
hunt, M. Sexual behavior in the 1970’s. Playboy 20, no. 10 (October 1973): 84–88, 197–207.
hunt, m. Sexual behavior in the 1970’s. Playboy 20, no. 11 (November 1973): 74–75.
hunt, m. Sexual behavior in the 1970’s. Playboy 20, no. 12 (December 1973): 90–91, 256.
hunt, M. Sexual behavior in the 1970’s. Playboy 21, no. 1 (January 1974): 60–61, 686–87.
hunt, m. Sexual behavior in the 1970’s. Playboy 21, no. 2 (February 197): 54–55, 176–77.
hursch, c. j. and selkin, j. Rape prevention research project. Annual Report, Violence Research Unit, Department of Health and Hospitals, Denver, 1974.
hyde, j. s. How large are cognitive gender differences? American Psychologist 36 (1981): 892–901.
iglitzin, l. b. A child’s eye view of sex roles. Paper presented at American Political Science Association Annual Meeting, Washington, D.C., 1972. ingiulla, w., adezati, L., forleo, r., and ingrassia, f. Menopause and male climacteric: Some physiological and clinical aspects. Giornale de Gerontologia 35 (1966): 5–60.
jacklin, c. n., maccoby, e. e., and dick, a. e. Barrier behavior and toy preference: Sex differences (and their absence) in the year-old child. Child Development 44 (1973): 196–200.
jackson, j. j. Black women and higher education (unpublished paper, 1973). Cited in Lewis, D. K. A response to inequality: Black women, racism, and sexism. In The Signs Reader, Abel, E., and Abel, E. K., eds., Chicago: University of Chicago Press, 1983.
jacobson, w. d. Power and interpersonal relations. Belmont, Calif.: Wadsworth, 1972.
jakobovits, i. Jewish views on abortion. In Walbert, D. F., and Butler, J. D., eds., Abortion, society, and the law. Cleveland: Press of Case Western Reserve, 1973.
james, w. Principles of psychology. New York: Henry Holt, 1890.
james, w. h. The effect of maternal psychological stress on the foetus. British
Journal of Psychiatry 1 15 (1969): 811–25.
janeway, e. Man’s world, luoman’s place. New York: Dell, 1971.
janeway, e. On “Female sexuality”. In Strouse, J., ed., Women and analysis.
New York: Grossman, 1974.
jelliffe, d. B. and Jelliffe, e. F. p. Current concepts in nutrition. Breast is
best: modern meanings. New England Journal of Medicine 297 (1977): 912–15.
JERSILD, a. T., and holmes, F. B. Children’s fears. Child Development Monographs 20 (1935).
John, k. e. Behind bars. Washington Post Magazine, January 15, 1984.
Johnson, m. Mental illness and psychiatric treatment among women: a response. Psychology of Women Quarterly 4 (1980): 363—71.
jones, e. The life and work of Sigmund Freud, vol. 1. New York: Basic Books, 1953.
jones, e. The life and work of Sigmund Freud, vol. 2. New York: Basic Books, 1955.
jones, e. The life and. work of Sigmund Freud, vol. 3. New York: Basic Books, 1957.
Jong, e. Fear of flying. New York: Holt, Rinehart and Winston, 1973.
joslyn, w.d. Androgen-induced social dominance in infant female rhesus monkeys. Journal of Child Psychology and Psychiatry 14 (1973): 137—45.
Jost, a. A new look at the mechanism controlling sex differentiation in mammals. Johns Hopkins Medical Journal 130 (1972): 38–53.
jourard, s. m. Disclosing man to himself. Princeton, N.J.: Van Nostrand, 1968.
kagan, j. Change and continuity in infancy. New York: Wiley, 1971.
kagan, j. The emergence of sex differences. School Review 80 (1972): 217—27.
kagan, j., and kogan, n. Individuality and cognitive performance. In Mus-
sen, P. H., ed., Carmichael’s manual of child psychology. New York: Wiley, 1970.
kagan, j., and moss, h. a. Birth to maturity: A study in psychological development. New York: Wiley, 1962.
Kaplan, h. s. Disorders of sexual desire. New York: Brunner / Mazel, 1979.
Kaplan, h. s. The new sex therapy. New York: Brunner / Mazel, 1974.
karmel, m. Thank you, Dr. Lamaze. Philadelphia: Lippincott, 1959.
kasper, A. s. TSS: a killer for how long? New Directions for Women, November / December, 1980.
kasten, k. Toward a psychology of being: A masculine mystique. Journal of Humanistic Psychology 12 (1972): 23—43
katchadourian, h. and lunde, D. Fundamentals of human sexuality. 2d ed. New York: Holt Rinehart & Winston, 1975.
katz, j. Gay American history: Lesbians and gay men in the USA. New York: Thomas Y. Crowell, 1976.
katz, s. and mazur, m. a. Understanding the rape victim. New York, 1979. kaufman, s. a. The ageless woman. New York: Dell, 1967.
kearney, h. r. Feminist challenges to the social structure and sex roles. Psychology of Women Quarterly 4 (1979): 16—31.
kelman, h. Karen Horney on feminine psychology. American Journal of Psychoanalysis 27 (1967): 163—83.
kimball, m. m. Women and science: A critique of biological theories. International Journal of Womens Studies 4 (1981): 318—88.
kimmel, d. c. Adulthood and aging. New York; Wiley, 1974.
kimura, d. Functional asymmetry of the brain in dichotic listening. Cortex 3 (1967): 163–78.
kinsey, a. c., pomeroy, w. b., and martin, c. e. Sexual behavior in the human male. Philadelphia: W. B. Saunders, 1948.
kinsey, a. c., pomeroy, w. b., martin, c. e., and gebhard, p. h. Sexual behavior in the human female. Philadelphia: W. B. Saunders, 1953.
kirk, h. d. Differential sex preference in family formation. Canadian Review of Sociology and Anthropology 1 (1964): 31—48.
kirsh, b. Consciousness-raising groups as therapy for women. In Franks, V., and Burtle, V., eds., Women in therapy. New York: Brunner / Mazel, 1974.
kisker, e. e. Teenagers talk about sex, pregnancy, and contraception. Family Planning Perspectives 17 (1985): 83—90.
kitzinger, s. Women as mothers: how they see themselves in different cultures. New York: Random House, 1978.
klaich, d. Women + woman: attitudes toward lesbianism. New York: Morrow Quill Paperbacks, 1979.
KLAUS, M. H., JERAULD, R., KREGER, N. C., MC ALPINE, W., STEFFA, M., and KENNELL, j. h. Maternal attachment: importance of the first post-partum days. New England Journal of Medicine 286 (1972): 460—63.
klaus, m. and kennell, j. Maternal-infant bonding. St. Louis: C. V. Mosby Co., 1976.
kleiman, d. “Career-minded Women Don’t Want to Sacrifice Motherhood,” St. Petersburg Times, February 1, 1981.
klein, v. The feminine character, 2d ed. Urbana: University of Illinois Press, 1971.
kluckhohn, c., and Murray, H. a. Personality in nature, society, and culture, 1st ed. New York: Knopf, 1949.
knopf, i. j. Childhood psychopathology. Englewood Cliffs, N.J.: Prentice-Hall, 1984.
knox, c., and kimura, d. Cerebral processing of nonverbal sounds in boys and girls. Neuropsychologia 8 (1970): 227–37.
koff, e. Through the looking glass of menarche: What the adolescent girl sees. In Golub, S., ed., Menarche. Lexington, Mass.: D.C. Heath, 1983.
kohlberg, l. The development of children’s orientation toward a moral order: I. Sequence in the development of human thought. Vita Humana 6 (1963): 11–33.
kohlberg, l. The philosophy of moral development. Vol I. New York: Harper and Row, 1981.
kohlberg, l. Revisions in the theory and practice of moral development. In Damon, W., ed., Moral development (New directions for child development, No. 2). San Francisco: Jossey-Bass, 1978.
kohlberg, l. a. A cognitive-development analysis of children’s sex-role concepts and attitudes. In Maccoby, E. E., ed., The development of sex differences. Stanford University Press, 1966.
konopka, G. The adolescent girl in conflict. Englewood Cliffs, NJ.: PrenticeHall, 1966.
konopka, G. Young girls: A portrait of adolescence. Englewood Cliffs, N.J.: Prentice-Hall, 1976.
koontz, e. Statement before the D.C. Commission on the Status of Women. November 4, 1971.
koten, j. Aged and alone. The Wall Street Journal, October 17, 1978.
krafft-ebing, r. von. Psychopathia sexualis. New York: Rebman, 1906.
kravetz, d. Consciousness-raising and self-help. In Brodsky, A. M. and Hare-Mustin, R., eds., Women and psychotherapy. New York: Guilford, 1980.
kreuz, l. e., and rose, r. m. Assessment of aggressive behavior and plasma testosterone in a young criminal population. Psychosomatic Medicine 34 (1972): 321–32.
krieger, s. Lesbian identity and community: Recent social science literature. Signs: Journal of Women in Culture and Society 8 (1982): 91—108.
krieger, s. The mirror dance: Identity in a womens community. Philadelphia: Temple University Press, 1983.
kuhn, t. s. The structure of scientific revolutions. Chicago: The University of Chicago Press, 1970.
kummer, h. Two variations in the social organizations of baboons. In Jay, P. C., ed., Primates—studies in adaptation and variability. New York: Holt, Rinehart and Winston, 1968.
kushner, h. i. Women and suicide in historical perspective. Signs: Journal of Women in Culture and Society 10 (1985): 537—52.
kutner, s. j. A survey of fear of pregnancy and depression. Journal of Psychology 79 (1971): 263–72.
ladner, j. a. Tomorrow’s tomorrow: the black woman. Garden City, N.Y.: Anchor Books, 1972.
lamb, m. e. and lamb, j. The nature and importance of father-infant relationships. Family Coordinator 25 (1976): 379—85.
lamb, m. e., owen, m. t., and chase-lansdale, l. The father-daughter relationship: past, present, and future. In Kopp, C. B., ed., Becoming female. New York: Plenum, 1979.
lambert, h. h. Biology and equality: a perspective on sex differences. Signs: Journal of Women in Culture and Society 4 (1978): 97—117.
lambert, w. e.; yackley, a.; and Hein, r. n. Child training values of English Canadian and French Canadian parents. Canadian Journal of Behavioral Science 3 (1971): 217—36.
lampl-de groot, j. The evolution of the Oedipus complex in women (1928). In Ruitenbeek, H., ed., Psychoanalysis and female sexuality. New Haven, Conn.: College and University Press, 1966.
lear, m. w. Save the spouses rather than the marriage. The New York Times Magazine, August 13, 1972.
leboyer, f. Birth without violence. New York: Knopf, 1975.
lederer, l. Take back the night. New York: William Morrow, 1980.
leifer, m. Pregnancy. Signs: Journal of Women in Culture and Society 5 (1980): 754–65.
lekachman, r. On economic equality. Signs: Journal of Women in Culture and Society 1 (1975): 93–102.
lemkau, j. p. Personality and background characteristics of women in male-dominated occupations: a review. Psychology of Women Quarterly 4 (1979): 221–40.
lennane, k. j., and lennane, r. j. Alleged psychogenic disorders in women— A possible manifestation of sexual prejudice. The New England Journal of Medicine 288 (1973): 288–92.
Leonard, e. b. Women, crime, and society. New York: Longman, 1982.
lerner, g. Black women in white America: A documentary history. New York: Vintage Books, 1973.
lerner, i. m. and libby w. J. Heredity, evolution and society. San Francisco: W. H. Freeman, 1976.
leventhal, g. Female criminality—is “women’s lib” to blame? Psychological Reports 41 (1977): 1179–82.
levinson, d. G., The Seasons of a Man’s Life, New York: Knopf, 1978.
levi-strauss, c. The elementary structures of kinship. London: Eyre and Spottiswoode, 1969.
levy, j. Lateral specialization of the human brain: Behavioral manifestations and possible evolutionary basis. In Kiger, J. A., ed., The biology of behavior. Corvallis, Ore.: Oregon University Press, 1972.
levy j. m., hembro, j., and alter, r. Psycho-behavioral correlates of first trimester abortion. Paper presented at the Seventh Annual Conference of the American Society for Psychosomatic Obstetrics and Gynecology, San Antonio, Texas, 1979.
Lewis, d. k. A response to inequality: Black women, racism, and sexism. In The Signs Reader, Abel, E. and Abel, E. K., eds. Chicago: University of Chicago Press, 1983.
lewis, m. Parents and children: Sex-role development. School Review 80 (1972): 229–40.
lewis, o. Manly-hearted women among the north Piegan. American Anthropologist 43 (1941): 173—87.
lindzey, g.; loehlin, j.; manosevitz, M.; and thiessen, d. Behavioral genetics. In Mussen, P. H., and Zweig, M. R. R., eds., Annual review of psychology. Palo Alto, Calif.: Annual Reviews, Inc., 1971.
Lincoln, r. Teenage pregnancy and childbearing: Why the differences between countries? Family Planning Perspectives 15 (1983): 104.
linn, l. Physician characteristics and attitudes toward legitimate use of psychotherapeutic drugs. Journal of Health and Social Behavior 12 (1971): 132–40.
lipman-blumen, j. How ideology shapes women’s lives. Scientific American 226 (1972): 34–42.
lippsett, l. and levy, n. Electrotactual threshold in the neonate. Child Development 30 (1959): 547—54.
loesch, j. g., and Greenberg, n. h. Some specific areas of conflict observed during pregnancy: A comparative study of married and unmarried pregnant women. American J ournal of Orthopsychiatry 32 (1962): 624–36.
lombroso, c., and ferrero, w. The female offender. New York: AppletonCentury-Crofts, 1916.
London, p., and rosenhan, d. Personality dynamics. In Farnsworth, P. R.; McNemar, O.; and McNemar, Q., eds., Annual Review of Psychology. Palo Alto, Calif.: Annual Reviews, Inc., 1964.
longino, h. e. Pornography, oppression, and freedom: A closer look. In Lederer., ed., Take back the night. New York: William Morrow, 1980.
longino, h. and doell, r. Body, bias, and behavior: A comparative analysis reasoning in two areas of biological science. Signs: Journal of Women in Culture and Society 9 (1983): 206—27.
lopata, h. z. The meaning of friendship in widowhood. In Troll, L. E., Israel, J., and Israel, K., eds., Looking ahead: A womans guide to the problems and joys of growing older. Englewood Cliffs, N.J.: Prentice-Hall, 1977.
lopata, h. z. Occupation: Housewife. New York: Oxford University Press, 1971. lopata, h. z. Widowhood in an American city. Cambridge, Mass.: Schenkman, 1973. (a)
lopata, h. z. Social relations of black and white widowed women in a north
ern metropolis. American Journal of Sociology 78 (1973): 1003—10. (b) lowenthal, m. f. Psychosocial variations along the adult life course: frontiers for research and policy. The Gerontologist 15 (1975): 6–12.
luker, k. Abortion and the politics of motherhood. Berkeley, Calif.: University of California Press, 1984a.
luker, k. The war between the women. Family Planning Perspectives 16 (1984b): 105–10.
lunde, d. t. Sex hormones, mood, and behavior. Paper presented at the 6th Annual Symposium, Society of Medical Psychoanalysis, New York, 1973.
luther, m. The table talk of Martin Luther. London: George Bell and Sons, 1890.
lynn, d. b. Daughters and parents: Past, present, and future. Monterey, Cal.: Brooks/Cole, 1979.
lynn, d. b. A note on sex differences in the development of masculine and feminine identification. Psychological Review 66 (1959): 126–35.
lynn, d. b. The process of learning parental and sex-role identification. In Schaeffer, D. L., ed., Sex differences in personality: Readings. Belmont, Calif.: Brooks/Cole, 1971.
maccoby, e. e., and jacklin, c. The psychology of sex differences. Stanford, Calif.: Stanford University Press, 1974.
macfarlane, a. The psychology of childbirth. Cambridge, Mass.: Harvard University Press, 1977.
macleish, k., and launois, j. Stone age cavemen of Mindanao. National Geographic 142 (1973): 219–48.
magrab, p. r. Mothers and daughters. In Kopp, C. B., ed., Becoming female. New York: Plenum, 1979.
mainardi, p. The politics of housework. In DeLora, J. S., and Delora, J. R., eds., Intimate life styles: Marriage and its alternatives. Pacific Palisades, Calif: Goodyear, 1972.
mamay, p. d. and simpson, r. l. Three female roles in television commercials. Sex Roles 7 (1981): 1223–32.
mann, h. The female review: The life of Deborah Sampson (1797). New York: Arno Press, 1972.
margolin, g. and patterson, g. r. Differential consequences provided by mothers and fathers for their sons and daughters. Developmental Psychology 11 (1975): 537–38.
mark, e. w. and alper, T. g. Women, men, and intimacy motivation. Psychology of Women Quarterly 9 (1985): 81—88.
marshall, d. s., and suggs, R. C., eds. Human sexual behavior. New York: Basic Books, 1971.
martin, d. What keeps a woman captive in a violent relationship? In Moore, D. M., ed., Battered women. Beverly Hills: Sage, 1979.
martin, d. and lyon, p. Lesbian / woman. New York: Bantam, 1972.
martin, l. Inadequate criteria for hypothesis testing in cerebral asymmetry research. Behavioral and Brain Sciences 3 (1990): 243.
maslow, a. Self-esteem (dominance feeling) and sexuality in women. Journal of Social Psychology 16 (1942): 259–94.
maslow, a. Motivation and personality. New York: Harper & Row, 1954. maslow, a. The further reaches of human nature. New York: Viking, 1971. masson, j. m. Freud and the seduction theory. The Atlantic, February 1984. masters, w., and Johnson, v. Human sexual response. Boston: Little, Brown, 1966.
masters, w., and Johnson, v. Human sexual response: The aging female and the aging male. In Neugarten, B., ed., Middle age and aging. Chicago: University of Chicago Press, 1968.
masters, w., and Johnson, v. Human sexual inadequacy. Boston: Little, Brown, 1970.
may, r. Mans search for himself. New York: Norton, 1953.
may, r. Sex differences in fantasy patterns. Journal of Projective Techniques 30 (1966): 576–86.
mayer, j. Better-educated mothers lead trend toward breast feeding. Houston Post, August 20, 1972.
maynard, j. Looking back: A chronicle of growing up old in the sixties. In Goodfriend, J. D. and Christie, C. M., eds., Lives of American women. Boston: Little, Brown, 1981.
mccaldon, r. j. Rape. Canadian Journal of Corrections 9 (1967): 37—59. mccary, j. l. Human sexuality. New York: Van Nostrand, 1973.
mcclearn, g. e. Genetic influences on behavior and development. In Mussen, P. H., ed., Carmichael’s manual of child psychology. New York: John Wiley and Sons, 1970.
mcclintock, m. k. Menstrual synchrony and suppression. Nature 229 (1971): 244–45.
mcdermott, m. j. Rape Victimization in 26 American cities. U.S. Department of Justice. Criminal Justice Research Center, Albany, N.Y., 1979.
mcguinness, d. Strategies, demands, and lateralized sex differences. Behavioral and Brain Sciences 3 (1980): 244.
mcintyre, a. Sex differences in children’s aggression. Proceedings of the 80th Annual Convention of the American Psychological Association 7 (1972): 93— 94.
mckain, w. c., Retirement marriage. Storrs, Conn.: Storrs Agriculture Experiment Station, University of Connecticut, 1969.
mcleod, b. Sexual swings. Psychology Today, September 1984.
mead, m. Coming of age in Samoa. New York: William Morrow, 1932.
mead, m. Sex and temperament in three primitive societies. New York: William Morrow, 1935.
mead, m. Blackberry winter. New York: William Morrow, 1972.
mead, m. On Freud’s view of female psychology. In Strouse, J., ed., Women and analysis. New York: Grossman, 1974.
mead, m. and heyman, k. Family. New York: Macmillan, 1965.
means, c. c. ,A historian’s view. In Hall, R. E., ed., Abortion in a changing world. New York: Columbia University Press, 1970.
medea, a. and Thompson, k. Against rape: A survival manual for women. New York: Farrar, Straus, and Giraux. 1974.
mednick, m. t. s., and weissman, h. j. The. psychology of women—selected topics. In Rosenzweig, M. R., and Porter, L. W., eds., Annual Review of Psychology. Palo Alto, Calif: Annual Reviews, Inc., 1975.
mednick, m. t. s.; tangri, s. j.; and hoffman, l. w. Women and achievement: Social and motivational analyses. Washington, D.C.: Hemisphere, 1975.
metropolitan life insurance company. Chances of dependency. Statistical Bulletin, 50 (January 1969): 10–11.
mill, j. s. On the subjection of women (1869). In Rossi, A., ed., The feminist papers. New York: Columbia University Press, 1973.
miller, j. b. Psychoanalysis and women. New York: Brunner / Mazel, 1973.
miller, p. y. and fowlkes, M. R. Social and behavioral constructions of female sexuality. Signs: Journal of Women in Culture and Society 5 (1980): 783–800.
Millett, k. Sexual politics. New York: Avon, 1971.
minton, c., kagan, j., and levine, j. a. Maternal control and obedience in the two-year-old. Child Development 42 (1971): 1873—94.
minturn, l. and Hitchcock, j. T. The Rajputs of Khalapur, India. In Whiting, B. B., ed., Six cultures. New York: Wiley, 1963.
mischel, w. Sex typing and socialization. In Mussen, P. H., ed., Carmichael’s manual of child psychology. New York: Wiley, 1970.
Mitchell, j. Women: The longest revolution. New Left Review, Nov./Dec. 1966, 1 1–37.
Mitchell, j. On Freud and the distinction between the sexes. In Strouse, J., ed., Women and analysis. New York: Grossman, 1974. (a)
Mitchell, j. Psychoanalysis and feminism. New York: Pantheon, 1974. (b) money, j. Psychosexual differentiation. In Money, J., ed., Sex research: New developments. New York; Holt, Rinehart and Winston, 1965.
money, j. Determinants of human sexual identity and behavior. In Sager, C. J., and Kaplan, H. S., eds., Progress in group and family therapy. New York: Brunner / Mazel, 1972 (a)
money, j. Identification and complementation in the differentiation of gender identity. Danish Medical Bulletin 19 (1972): 265—68. (b)
money, j. Love and love sickness: The science of sex, gender difference and pair-bonding. Baltimore: Johns Hopkins University Press, 1980.
money, j., and Ehrhardt, a. Man and woman, boy and girl. Baltimore: The Johns Hopkins University Press, 1972.
monroe, r. Schools of psychoanalytic thought. New York: Dryden, 1955.
moore, d. Battered women. Beverly Hills: Sage, 1979.
moore, m. Aggression themes in a binocular rivalry situation. Journal of Personality and Social Psychology 3 (1966): 685—88.
moos, r. h. Typology of menstrual cycle symptoms. American Journal of Obstetrics and Gynecology 103 (1969): 390—402.
moran, r. The singles in the seventies. In DeLora, J. S., and DeLora, J. R., eds., Intimate life styles: Marriage and its alternatives. Pacific Palisades, Galif.: Goodyear, 1972.
Morgan, r. Going too far. New York: Random House, 1977.
morin, s. f. Heterosexual bias in psychological research on lesbianism and male homosexuality. American Psychologist 32 (1977): 629–37.
MORTON, J. H., ADDISON, H., ADDISON, R. G., HUNT, L., and SULLIVAN, J. J. A
clinical study of premenstrual tension. American Journal of Obstetrics and Gynecology 65 (1953): 1182–91.
moss, H. a. Sex, age, and state as determinants of mother-infant interaction. Merrill Palmer Quarterly 13 (1967): 19—36.
moss, z. (pseud.). It hurts to be alive and obsolete: The aging woman. In Morgan, R., ed., Sisterhood is powerful: An anthology of writings from the womens liberation movement. New York: Vintage Press, 1970.
Montague, a. Smoking, pregnancy, and sex. Sexology, November 1963, 220—22.
Moulton, j. Philosophy. Signs: Journal of Women in Culture and Society 2 (1976): 422–33.
moynihan, d. p. The Negro family: The case for national action. Office of Policy Planning and Research, U.S. Department of Labor, Washington, D.C., 1965.
mueller, e. Attitudes toward the economics of family size and their relation to fertility. Unpublished manuscript, University of Michigan. Cited in Hoffman, L. W., and Hoffman, M. L. The value of children to parents. In Fawcett, J. T., ed., Psychological perspectives on population. New York: Basic Books, 1973.
muncy, r. l. Sex and marriage in utopian communities: 19th century America. Bloomington, Ind.: Indiana University Press, 1973.
murai, n. and sato, t. Psychological study on pregnancy-relationship of maternal emotional characteristics to body weight gain of newborn infants. Journal of the Japanese Psychosomatic Society 11 (1971): 25—29.
Murray, s. r. and mednick, m. t. s. Black women’s achievement orientation: motivational and cognitive factors. Psychology of Women Quarterly 1 (1977): 247–59. ‘ ’
murstein, b. I. Love, sex, and marriage through the ages. New York: Springer, 1974.
müssen, p. H., and rutherford, e. Parent-child relations and parental personality in relation to young children’s sex-role preferences. Child Development 34 (1963): 589—607.
nahum, l. h. Amniocentesis in prediction of chromosomal and behavioral abnormalities. Connecticut Medicine 34 (1970): 10, 12.
nash, s. c. Sex role as a mediator of intellectual functioning. In Wittig, M. A. and Petersen, A. C., eds., Sex-related differences in cognitive functioning. New York: Academic Press, 1979.
Navratilova, m. Martina. New York: Knopf, 1985.
neugarten, b. l. Summary and implications. In Neugarten, B. L., et al., eds., Personality in middle and late life. New York: Atherton, 1964.
neugarten, b. l. Education and the life cycle. School Review 80 (1972): 20916.
neugarten, b. l. A new look at menopause. In Tavris, C., ed., The female experience. Del Mar, Calif.: Communications / Research / Machines, 1973.
neugarten, b. l., et al., eds., Personality in middle and late life. New York: Atherton, 1964.
neugarten, b. l. and Gutmann, D. l. Age-sex roles and personality in middle age: a thematic apperception study. In Neugarten, B. L., ed., Middle age and aging. Chicago: University of Chicago Press, 1968.
newland, K. Women, men and the division of labor. Worldwatch Paper 37, Worldwatch Institute, Washington, D.C.
newson, j., and newson, e. Four years old in an urban community. Harmond-worth, England: Pelican Books, 1968.
newton, m. Breast-feeding. Psychology Today 2 (1968): 34, 68–70.
newton, n., and newton, m. Childbirth in crosscultural perspective. In Howells, J. G., ed., Modern perspectives in psycho-obstetrics. New York: Brunner / Mazel, 1972.
nietzsche, f. n. Thus spake Zarathustra. New York: Russell and Russell, 1964. nilsson, a., and alnigren, p. Para-natal emotional adjustment—A prospective investigation of 165 women. Pt. II. Acta Psychiatrica Scandinavian 220 (1970): 65–151.
nortman, d. Parental age as a factor in pregnancy outcome and child development. Reports on Population/Family Planning. The Population Council, 245 Park Avenue, New York, N.Y., August, 1974.
oakley, a. The sociology of housework. New York: Pantheon, 1974.
oberstone, h. k. and sukoneck, h. Psychological adjustment and life style of single lesbians and single heterosexual women. Psychology of Women Quarterly 1 (1976): 172–88.
O’BRIEN, J. S., OKADA, S., FILLERUP, D. L., VEATH, M. L., ADORNATO, B., BRENNER, p. h., and leroy, j. G. Tay-Sachs disease: Prenatal diagnosis. Science 172 (1971): 61–67.
oetzel, r. m. Classified summary of research in sex differences. In Maccoby, E. E., ed., The development of sex differences. Stanford, Calif.: Stanford University Press, 1966.
ohno, s. The role of H-Y antigen in primary sex determination. Journal of the American Medical Association 239 (1978): 217—20.
Oliver, w. a. Childbirth expectancies and experiences as a function of locus of control and Lamaze training. (Doctoral dissertation, Ohio State University, 1972). University Microfilms No. 72–27074. Dissertation Abstracts International, Ann Arbor, Michigan.
o’neill, g., and o’neill, n. Open marriage. New York: Avon, 1972.
Overstreet, e. w. Female sterilization. In Calderone, M., ed., Manual of family planning and contraceptive practice. Baltimore: Williams & Wilkins, 1970.
palm, r. and abrahamsen, d. A Rorschach study of the wives of sex offenders. Journal of Nervous and Mental Diseases 119 (1954): 167—72.
parke, r., o’leary, s., and west, s. Mother-father-newborn interaction: Effects of maternal medication, labor, and sex of infant. Proceedings of the 80th Annual Convention of the American Psychological Association, 1972.
parks, m. China waging all-out campaign against female infanticide. The St. Petersburg Times, June 8, 1983.
parlee, m. b. The premenstrual syndrome. Psychological Bulletin 80 (1973): 454–65.
parlee, m. b. Psychology and women. Signs: Journal of Women in Culture and Society 5 (1979): 121–33.
parsons, t. Essays in sociological theory, pure and applied, 2d ed. Glencoe, Ill.: The Free Press, 1954.
parsons, t., and bales, r. e. Family socialization and interaction process. Glencoe, Ill.: The Free Press, 1955.
paterson, e. j. How the legal system responds to battered women. In Moore, D., ed., Battered women. Beverly Hills: Sage, 1979.
pauley, f. r. Sex differences and legal school entrance age. Journal of Educational Research 45 (1951): 1—9.
payak, b. Understanding the female offender. Federal Probation 27 (1963): 7–12.
Pendergrass, v. e. Women as clinicians in private practice. American Psychologist 29 (1974): 533–35.
peplau, l. a., cochran, s., rook, k. and padesky, c. Loving women: Attachment and autonomy in lesbian relationships. Journal of Social Issues 34 (1978): 7–27.
Perlmutter, j. f. Drug addiction in pregnant women. American Journal of Obstetrics and Gynecology 99 (1967): 569—72.
Perlmutter, j. f. A gynecological approach to menopause. In Notman, M. T. and Nadelson, C. C., eds., The woman patient: medical and psychological interfaces. New York: Plenum, 1978.
petersen, a. c. Hormones and cognitive functioning in normal development. In Wittig, M. A. and Peterson, A. C., eds., Sex-related differences in cognitive functioning. New York: Academic Press, 1979.
Phillips, d., and segal, b. Sexual status and psychiatric symptoms. American Sociological Review 34 (1969): 58—72.
piaget, j. The moral judgment of the child (1932). New York: Free Press, 1965. pierce, c. Philosophy. Signs: Journal of Women in Culture and Society 1 (1975): 487–503.
pleck, j. h. Working wives I working husbands. Beverly Hills, Calif.: Sage Publications, 1985.
Poffenberger, a. t. Leta Stetter Hollingworth: 1886—1939. American Journal of Psychology 53 (1940): 299–301.
pohlman, e. h. Influencing people to want fewer children. Paper presented at the American Psychological Association Convention, Miami, Florida, September 1970.
pollack, o. The criminality of women. Philadelphia: University of Pennsylvania Press, 1950.
poi.oma, m. m. The married professional woman: An empirical examination of three myths. (Doctoral Dissertation, Case Western Reserve University, 1971). University Microfilms No. 71–19042. Dissertation Abstracts International, Ann Arbor, Michigan.
poloma, m. m., and garland, t. n. The myth of the egalitarian family: Familial roles and the professionally employed wife. In Theodore, A., ed., The’professional woman. Cambridge, Mass.: Schenkman, 1971.
Population council annual report. New York: The Population Council, 1973.
Population council annual report. New York: The Population Council, 1980.
Population Research Office, Anhui University. A survey of one-child families in Anhui Province, China. Studies in Family Planning 13 (1982): 216— 21.
porter, c. w., jr., and waife, r. s. Intrauterine devices: Current perspectives. Second edition. Chestnut Hill, Mass.: The Pathfinder Fund, 1982.
porteus, s., and babcock, m. e. Temperament and race. Boston: Gorham Press, 1926.
powell, g. j. Growing up black and female. In Kopp, C. B., ed., Becoming female. New York: Plenum, 1979.
prather, j., and fidf.ll, l. Put her down and drug her up. Paper presented at American Sociological Association Meeting, New Orleans, Louisiana, August, 1972.
prather, j. e. and fidell, l. s. Sex differences in the content and style of medical advertisements. Social Science and Medicine 9 (1975): 23–26.
prendergast, p., zdep, s. m., and Sepulveda, p. Self image among a national probability sample of girls. Child Study Journal 4, (1974): 103–14.
presser, h. b. Puerto Rico: Recent trends in fertility and sterilization. Family Planning Perspective 12 (1980): 102—6.
preston, l. Valley of the forgotten women. Washington Post Magazine, January 15, 1984.
price, r. r. The forgotten female offender. Crime and Delinquency 23 (1977): 101–8.
pringle, m. l. k., butler, n. r., and davie, r. Eleven thousand seven-year olds. London: Longmans, 1966.
puner, m. Will you still love me? Human Behavior 3 (1974): 6, 42–48.
radloff, l., Sex differences in depression: the effects of occupation and marital status. Sex Roles 1 (1979): 249–65
rainwater, l. Family design: Marital sexuality, family size, and contraception. Chicago: Aldine, 1965.
Ramey, j. W. Communes, group marriage and the upper-middle class. In Smith, J. R., and Smith, L. G., eds., Beyond Monogamy. Baltimore: The Johns Hopkins University Press, 1974.
rand, l. m., and miller, a. l. A developmental cross-sectioning of women’s careers and marriage attitudes and life plans. Journal of Vocational Behavior 2 (1972): 317–31.
rebelsky, f. and hanks, c. Fathers’ verbal interactions with infants in the first three months of life. Child Development 42 (1971): 63–68.
renne, k. s. Childlessness, health, and marital satisfaction. Social Biology 23 (1976): 183–97.
rheingold, j. c. The fear of being a woman. New York: Grune and Stratton, 1964.
rich, a. Compulsory heterosexuality and lesbian existence. Signs: Journal of Women in Culture and Society 5 (1980): 631—60.
rich, a. Of woman born: motherhood as experience and institution. New York: Norton, 1976.
riesman, d., glazer, N., and Denny, r. The lonely crowd. Garden City, N.Y.: Doubleday, 1953.
riopelle, a. j., and Rogers, c. m. Age change in chimpanzees. In Shrier, A. M.: Harlow, H. F.; and Stollnitz, F., eds., Behavior of non-human primates. New York: Academic Press, 1965.
ritter, c. a. Why pre-natal care. American Journal of Gynecology 70 (1919): 531.
rivenbark, w. h., in. Self disclosure among adolescents. Psychological Reports 28 (1971): 35–42.
Rogers, K. The troublesome helpmate: A history of misogyny in literature. Seattle: University of Washington Press, 1966.
Rogers, K.o.For her own protection. Law and Society Review 7 (1972): 223—46.
rosaldo, m. z. The use and abuse of anthropology: reflections on feminism and cross cultural understanding. Signs: Journal of Women in Culture and Society 5 (1979): 389–417.
rose, r. m., Gordon, t. p., and bernstein, i. s. Plasma testosterone levels in the male rhesus: Influences of sexual and social stimuli. Science 178 (1972): 643–45.
rosen, d. h. Lesbianism: A study of female homosexuality. Springfield, Ill.: Charles C Thomas, 1974.
rosen, j. l. and neugarten, b. l. Ego functions in the middle and late years: A thematic apperception study. In Neuarten, B. L., et al., eds., Personality in middle and late life. New York: Atherton, 1964.
ROSENBERG, K. M., DENENBERG, V. H., ZARROW, M. X., and BONNIE, L. F. Effects of neonatal castration and testosterone on the rat’s pup-killing behavior and activity. Psysiology and Behavior 7 (1971): 363–68.
Rosenblatt, j. s. The development of maternal responsiveness in the rat. American Journal of Orthopsychiatry 30 (1969): 36—56.
ross, e. “The love crisis”: couples advice books of the late 1970s. Signs: Journal of Women in Culture and Society 6 (1980): 109—22.
rossi, a. A biosocial perspective on parenting. Daedalus 106 (1977): 1—22. rossi, a. s. The biosocial side of parenthood. Human Nature, June 1978.
rossi, A. Equality between the sexes: An immodest proposal. Daedalus 93 (1964): 607–52.
rossi, a. The feminist papers: From Adams to de Beauvoir. New York: Columbia University Press, 1973.
rossi, a. s. Life-span theories and women’s lives. Signs: Journal of Women in Culture and Society 6 (1980): 4—32.
roth, p. Portnoy’s complaint. New York: Random House, 1967.
rothbart, m. k. Birth order and mother-child interaction in an achievement situation. Journal of Personality and Social Psychology 17 (1971): 113—20.
rothbart, m. k., and maccoby, e. e. Parents’ differential reactions to sons and daughters. Journal of Personality and Social Psychology 4(1966): 237—43 rousseau, j. j. Emile. New York: Basic Books, 1979.
rowe, i. l. Prescriptions of psychotropic drugs by general practitioners. Medical Journal of Australia 1 (1973): 642—44.
roy, p. Adolescent roles: Rural-urban differentials. In Nye, F. 1., and Hoffman, L. W., eds., The employed mother in America. Chicago: Rand McNally, 1963.
rubin, j. z., Provenzano, f. j., and luria, z. The eye of the beholder: Parents’ views on sex of newborns. American Journal of Orthopsychiatry 44 (1974): 512–19.
rubin, r. t., reinisch, j. m., and Haskett, r. f. Postnatal gonadal steroid effects on human behavior. Science 211 (1981): 1318—24.
rugoff, M. Prudery and passion. New York: Putnam, 1971.
russell, d. e. h. Questions we get asked most often. In Lederer, L., ed., Take back the night. New York: William Morrow, 1980.
russo, n. F., ed. A national agenda to address womens mental health needs. Washington, D.C.: American Psychological Association, 1985.
russo, n. f. Overview: sex roles, fertility, and the motherhood mandate. Psychology of Women Quarterly 4 (1979): 7–15.
russo, n. f. and o’connf.ll, a. n. Models from our past: psychology’s foremothers. Psychology of Women Quarterly 5 (1980): 11—54.
safilios-rothschild, c. Sexuality, power, and freedom among “older” women. In Troll, L. E., Israel, J., and Israel, K., eds., Looking ahead: A woman’s guide to the problems and joys of growing older. Englewood Cliffs, N.J.: Prentice-Hall, 1977.
sanford, n. Personality: Its place in psychology. In Koch, S., ed., Psychology: A study of a science. New York: McGraw-Hill, 1963.
sarvis, B., and rodman, h. The abortion controversy. New York: Columbia University Press, 1973.
saucier, j. f. Correlates of the long postpartum taboo: A cross-cultural study. Current Anthropology 13 (1972): 238—49.
scarf, M. Unfinished business: pressure points in the lives of women. New York: Doubleday, 1980.
schaar, k. Suicide rate high among women psychologists. APA Monitor 5 (1974): 1, 10.
schafer, a. and gray, m. Sex and mathematics. Science 211 (1981): 113.
Schildkraut, j. j. The catecholamine hypothesis of affective disorders: A review of supporting evidence, American Journal of Psychiatry 122 (1965): 509–22.
schulz, d. a. The changing family: Its function and future. Englewood Cliffs, N.J.: Prentice-Hall, 1972.
scott, k. Birth at home. The St. Petersburg Times, June 6, 1977.
scully, d., and bart, p. A funny thing happened on the way to the orifice: Women in gynecology textbooks. American Journal of Sociology 78 (1973): 1045–50.
sears, p. s., and feldman, d. h. Teacher interactions with boys and with girls. In Stacey, J.; Bereaud, S.: and Daniels, J., eds., And Jill came tumbling after: Sexism in American education. New York: Dell, 1974.
sears, r. r., maccoby, e. e., and levin, h. Patterns of child rearing. Stanford, Calif.: Stanford University Press, 1976.
sears, r. r., raul, L., and alpert, r. Identification and child-rearing. Stanford, Calif.: Stanford University Press, 1965.
SHAH, f. and zelnik, m. Sexuality in adolescence. In Wolman, B. J. and Money, J., eds., Handbook of human sexuality. Englewood Cliffs, N.J.: Prentice-Hall, 1980.
shainess, n. Feminine identity and mothering. In Masserman, J. H., ed., Science and Psychoanalysis, vol. 7. New York: Grune and Stratton, 1964.
shanan, j., brzezinski, h., shilman, f., and sharon, m. Active coping behavior, anxiety, and cortical steroid excretion in the prediction of transient amenorrhea. Behavioral Science 10 (1965): 461—65.
shephard, b. D. and Shephard, c. a. The complete guide to womens health. Tampa, Fla.: Manner, 1982.
shepherd, w., and peterson, j. Are there sex differences in infancy? JSAS Catalog of Selected Documents in Psychology 3 (1973): 121.
sherfey, m. j. The nature and evolution of female sexuality. New York: Random House, 1972.
sherman, j. mathematics, spatial visualization, and related factors: Changes in girls and boys, grades 8—11. Journal of Educational Psychology 72 (1980): 476–82.
sherman, j. On the psychology of women. Springfield, III.,: Charles C Thomas, 1971.
sherman, j. Sex-related cognitive differences: An essay on theory and evidence. Springfield, Ill.: Charles C Thomas, 1978.
sherman, j. a. and fennema, e. Distribution of spatial visualization and mathematical problem solving scores: a test of Stafford’s X-linked hypothesis. Psychology of Women Quarterly 3 (1978): 157—67.
shields, s. a. The variability hypothesis and sex differences in intelligence. Unpublished manuscript, 1974. (Available from Department of Psychology, Pennsylvania State University, State College, Pennsylvania.)
shields, s. a. Functionalism, Darwinism, and the psychology of women. American Psychologist 30 (1975): 739—754.
shostak, m. Nisa: The life and words of a !Kung woman. Cambridge, Mass.: Harvard University Press, 1981.
shulman, a. A marriage agreement. In Perrucci, C. C., and Targ, D. B., eds., Marriage and the family. New York: David McKay, 1974.
shusterman, l. r. The psychological factors of the abortion experience. Psychology of Women Quarterly 1 (1976): 79—106.
sidel, r. Women and child care in China. Baltimore: Penguin, 1973.
silka, l. and kiesler, s. Couples who choose to remain childless. Family Planning Perspective 9 (1977): 16—25.
silvers, w. k. and wachtel, s. s. H-Y antigen: Behavior and function. Science 195 (1977): 956–60.
simpson, e. l. Moral development research: A case of scientific cultural bias. Human Development 17 (1974): 81 — 106.
singer, i., and singer, j. Types of female orgasm. Journal of Sex Research 8 (1972): 255–67.
singer, j. e., westphal, m., and niswander, k. r. Sex differences in the incidence of neonatal abnormalities and abnormal performance in early childhood. Child Development 39 (1968): 103—122.
sjovall, e. Coitus interruptus. In Calderone, M., ed., Manual of Family planning and contraceptive practice. Baltimore: Williams 8c Wilkins, 1970.
skultans, v. The symbolic Significance of menstruation and the menopause. Man 5 (1970): 639–51. ’
smith, e. j. The black female adolescent: A review of the educational, career, and psychological literature. Psychology of Women Quarterly 6 (1982): 261–88.
smith, j. R., and smith, l. g., eds. Beyond monogamy. Baltimore: The Johns Hopkins University Press, 1974.
smith-rosenberg, c. The female world of love and ritual: Relations between women in nineteenth-century America. Signs: Journal of Women in Culture and Society 1 (1975): 1—29.
Sutherland, s. and scherl, d. Patterns of response among victims of rape. American Journal of Orthopsychiatry 40 (1970): 503—11.
solberg, d. a., butler, j., and wagner, n. n. Sexual behavior in pregnancy. New England Journal of Medicine 288 (1973): 1098—1103.
sontag, s. The double standard of aging. Saturday Review 55 (1972): 39, 29–38.
sorenson, r. c. Adolescent sexuality in contemporary America, (The Sorenson Report). New York: World Publishing, 1973.
spielberger, c. d., lushene, r. e., and mcadoo, w. g. Theory and measurement of anxiety states. In Cattell, R. B., ed., Handbook of Modern Personality Theory. Chicago: Aldine, 1970.
spitz, r., and wolf, k. m. Anaclitic depression: An inquiry into the genesis of psychiatric conditions in early childhood. In The psychoanalytic study of the child, vol. 2. New York: International Universities Press, 1946.
spranger, e. Types of men, trans. Pigors, P. J. W. Halle: Niemeyer, 1928.
squires, s. Sex survey reaction is more telling than “the act.” The Tampa Tribune, January 26, 1985.
st. john-parsons, d. Continuous dual-career families: a case study. Psychology of Women Quarterly 3 (1978): 30—42.
stacey, j., bereaud, s., and Daniels, j. And Jill came tumbling after: Sexism in American education. New York: Dell, 1974.
Stafford, r. e. Hereditary and environmental components of quantitative reasoning. Review of Educational Research 42 (1972): 183—201.
stafford-ci.ark, d. What Freud really said. New York: Schocken, 1965.
staples, R.Themyth of the black matriarchy. The Black Scholar 1 (1970): 8–16.
stein, a. h., and bailey, m. m. The socialization of achievement orientation in females. Psychological Bulletin 80 (1973): 345—66.
STEKLIS, H. D., BRAMMER, G. L., RALEIGH, M. J., and MCGUIRE, M. T. Serum testosterone, male dominance, and aggression in captive groups of vervet monkeys. Hormones and Behavior 19 (1985): 154–63.
sterling, d. h. The experience of bcing-me for black adolescent females: A phenomenological investigation of black identity. Dissertation Abstracts International 35 (1975): 5039A—40A.
stevenson, ii. w., halve, g. a., hill, k. t., and moely, b. e. Determinants of children’s preference for adults. Child Development 38 (1967): 1–14.
stimpson, c. Zero degree deviancy: The lesbian novel in English. Critical Inquiry 8 (1981): 363–79.
stoller, r. j. The “bedrock” of masculinity and femininity: Bisexuality. Archives of General Psychiatry 26 (1972): 207–12.
STOLLER, r. j. Facts and fancies: An examination of Freud’s concept of bisexuality. In Strouse, J., ed., Women and analysis. New York: Grossman, 1974.
stricker, g. Implications of research for psychotherapeutic treatment of women. American Psychologist 32 (1977): 14—22.
striegel-moore, r. h., silberstien, l. r., and rodin, j. Toward an understanding of risk factorsfor bulimia. American Psychologist 41 (1986): 246–63.
strouse, j., ed. Women and analysis. New York: Grossman, 1974.
Studies in family planning. New York: The Population Council, 1980.
SUTHERLAND, h., and stewart, i. A critical analysis of the pre-menstrual syndrome, Lancet 1 (1965): 1180–93.
Sutherland, s. l. The unambitious female: women’s low professional aspirations. Signs: Journal of Women in Culture and Society 3 1978): 774–94.
sviland, m.a.p. Helping elderly couples attain sexual liberation and growth. S1ECUS Report, July, 1976.
Swanson, h. h. Effects of castration at birth in hamsters of both sexes on luteinization of ovarian implants, oestrous cycles and sexual behavior. Journal of Reproduction and Fertility 21 (1970): 183–86.
Szasz, t. s. The myth of mental illness. New York: Hoeber-Harper, 1961.
Szasz, t. s. The manufacture of madness. New York: Harper & Row, 1970.
tanner, j. m. Fetus into man. Cambridge, Mass.: Harvard University Press, 1978.
tanzer, d. Natural childbirth: Pain or peak experience. In Tavris, C., ed., The female experience. Del Mar, Calif.: Communications / Research / Machines, 1973.
TASK FORCE on sex bias and sex role stereotyping. American Psychologist 33 (1978): 1122–23.
taube, c. a., burns, b. j., and kessler, L. Patients of psychiatrists and psychologists in office-based practice: 1980. American Psychologist 39 (1984): 1435–47.
Taussig, f. j. Abortion, spontaneous and induced. St. Louis: C. V. Mosby Co., 1936.
tavris, c. and sadd, s. The Redbook report on female sexuality. Nw York: Delacorte Press, 1977.
Taylor, c. w., and barron, f. A look ahead. In Taylor, C. W., and Barron, F., eds., Scientific creativity: Its recognition and development. New York: Wiley, 1963.
Temur, s. Socio-economic determinants of differential fertility in Turkey, The Second European Population Conference, Strasbourg, 1971.
terman, l. M., and Oden, m. h. Genetic studies of genius, vol. 4. Stanford, Calif.: Stanford University Press, 1947.
terman, L. M., and Oden, m. h. Genetic studies of genius, vol. 5. Stanford, Calif.: Stanford University Press, 1959.
Thompson, c. Cultural pressures in the psychology of women (1942). In Green, M. R., ed., Interpersonal psychoanalysis: The selected papers of Clara Thompson. New York: Basic Books, 1964.
Thompson, c. Some effects of the derogatory attitude toward female sexuality (1950). In Green, M. R., ed., Interpersonal psychoanalysis: The selected papers of Clara Thompson. New York: Basic Books, 1964.
Thompson, c. Sullivan and psychoanalysis (1952). In Green, M. R., ed., Interpersonal psychoanalysis: The selected papers of Clara Thompson. New York: Basic Books, 1964.
Thompson, c. Working women (1953). In Green, M. R., ed., Interpersonal psychoanalysis: The selected papers of Clara Thompson. New York: Basic Books, 1964.
Thompson, c. Problems of womanhood: In Green, M. R., ed., Interpersonal psychoanalysis: The selected papers of Clara Thompson. New York: Basic Books, 1964.
Thorndike, e. L. Sex in education. The Bookman 23 (1906): 211–14.
tidball, m. e. Women’s colleges and women achievers revisited. Signs: Journal of Women in Culture and Society 5 (1980): 504–17.
tobin, p. The effects of practice and training on sex differences in performance of a spatial task. Unpublished master’s thesis, University of Toronto, 1982.
TREADWAY, C. R., KANE, J. F., JR., JARRAHI-ZADEH, A., and LIPTON, M. A. A psychoendocrine study of pregnancy and the puerperium. In Unger, R. K., and Denmark, F. L., eds., Woman: Dependent or independent variable? New York: Psychological Dimensions, 1975.
tresemer, d. w. Fear of success. New York: Plenum, 1977.
turkington, c. Ideology affects approach taken to alleviate PMS. APA Monitor, January 1984.
tylden, e. Hyperemesis and physiological vomiting. Journal of Psychosomatic Research 12 (1968): 85—93.
uddenberg, n., almgren, p. e., and nilsson, a. Preference for sex of the child among pregnant women. Journal of Biosocial Science 3 (1971): 267— 80. ’
uits, c. Self image and roles. In No longer young. Work Group Reports from the 26th Annual Conference on Aging. Institute of Gerontology, University of Michigan and Wayne State University, 1974.
united press international. Nearly 9-million Chinese women had abortions in 1984, expert says. St Petersburg Times, November 24, 1985.
van de castle, r. l., and kinder, p. Dream content during pregnancy. Psychophysiology 4 (1968), 375.
Vandenberg, s. g. Primary mental abilities or general intelligence? Evidence from twin studies. In Thoday, J. M., and Parkes, A. S. Genetic and environmental influences on behavior. New York: Plenum Press, 1968.
vandenberg, s. g. and kuse, a. r. Spatial ability: a critical review of the sex-linked major gene hypothesis. In Wittig, M. A. and Petersen, A. C., eds., Sex-related differences in cognitive functioning. New York: Academic Press, 1979.
van de velde, T. Ideal marriage, its physiology and technique. Browne, S., trans. (1926). New York: Random House, 1930.
van dusen, r. a. and sheldon, e. b. The changing status of American women: a life cycle perspective. American Psychologist 31 (1976): 106—16.
vedder, c. b., and king, P. G. Problems of homosexuality in prisons. Springfield, Ill.: Charles C Thomas, 1967.
vessey, M. p. Oral contraceptives and stroke. New England Journal of Medicine 288 (1973): 906–7.
veysey, l. Communal sex and communal survival. Psychology Today 8 (1974): 73–78.
vicinus, m. Distance and desire: English boarding-school friendships. Signs: Journal of Women in Culture and Society 9 (1984): 600—22.
vida, g. Our right to love: A lesbian source book. New York: Prentice-Hall, 1978.
vogel, i. When I grow up. New York: Western Publishing, 1968.
voth, h. m. Love affair between doctor and patient. American Journal of Psychotherapy 26 (1972): 394—400.
waber, d. p. Cognitive abilities and sex-related variations in the maturation of cerebral cortical functions. In Wittig, M. A. and Petersen, A. C., eds., Sex-related differences in cognitive functioning. New York: Academic Press, 1979.
WADE, M. E., MCCARTHY, P., ABERNATHY, J. R., HARRIS, G. S., DANZER, H. C., and uricchio, w. a. A randomized prospective study of the use-effectiveness of two methods of natural family planning: an interim report. American Journal of Obstetrics and Gynecology 134 (1979): 628.
Wakefield, w. m. Awareness, affection, and perceived similarity in the parent-child relationship. Journal of Genetic Psychology 111 (1970): 91—97.
walberg, h. j. Physics, femininity, and creativity. Developmental Psychology, 1 (1969): 47–54.
waldron, i. Why do women live longer than men? Social Science and Medicine 10 (1976): 349–62.
waldrop, m. f., and Halverson, c. F., jr. Intensive and extensive peer behavior: Longitudinal and cross-sectional analyses. Unpublished manuscript, Child Research Branch, National Institute of Mental Health, Washington, D.C., 1973.
walker, a. In search of our mothers’ gardens. New York: Harcourt Brace Jovanovich, 1983.
walker, a. Quoted in Women on women. American Scholar 41 (1972): 599— 627.
walker, l. e. a. Battered women, psychology, and public policy. American Psychologist 39 (1984): 1178–82.
walker, l. e. How battering happens and how to stop it. In Moore, D., ed., Battered women. Beverly Hills: Sage, 1979.
walker, l. Sex differences in the development of moral reasoning: A critical review. Child Development 54 (1983): 1103—41.
Walters, r: g. Primers for prudery. Englewood Cliffs, N.J.: Prentice-Hall, 1974. ward, d. a., jackson, m., and ward, r. e. Crimes of violence by women. In Mulvihill, D., ed., Crimes of violence. Washington, D.C.: United States Government Printing Office, 1969.
ward, 1. l. Female sexual behavior in male rats treated prenatally with an anti-angrogen. Psyiology and Behavior Vol. 8, 1972, p. 53–56.
ward, w. d. Variance of sex-role preference among boys and girls. Psychological Reports 23 (1968): 467—70.
ward, w. d. Process of sex-role development. Developmental Psychology 1 (1969): 163–68.
warrington, e. k., james, m., and kinsbourne, m. Drawing disability in relation to laterality of cerebral lesion. Brain 89 (1966): 53—82.
wallston, b. s. What are the questions in psychology of women? A feminist approach to research. Presented at the annual meeting of the American Psychological Association, New York City, 1979.
watson, j. b. Psychology from the standpoint of a behaviorist, 2d ed. Philadelphia: Lippincott, 1924.
watson, j. s. Operant conditioning of visual fixation in infants under visual and auditory reinforcement. Developmental Psychology 1 (1969): 408–16.
webster, b. s. Helen Deutsch: A new look. Signs: Journal of Women in Culture and Society 10 (1985): 553—71.
weideger, p. Menstruation and menopause. New York: Dell, 1977.
Weingarten, k. The employment pattern of professional couples and their distribution of involvement in the family. Psychology of Women Quarterly 3 (1978): 43–52.
WEINRAUB, M., CLEMENS, L. P., SOCKLOFF, A., ETHRIDGE, T., GRACELY, E., and myers, b. The development of sex-role stereotypes in the third year: Relationships to gender labeling, gender identity, sex-typed toy preference, and family characteristics. Child Development 55 (1984): 1493—1503.
weisheit, r. a. Women and crime: Issues and perspectives. Sex Roles 11 (1984): 567–81.
weisskopf, m. China’s crusade against children. Washington Post National Weekly Edition, January 28, 1985.
weisskopf, s. c. Maternal sexuality and asexual motherhood. Signs: Journal of Women in Culture and Society 5 (1980): 766—82.
weissman, m. and klerman, G. Sex differences in the epidemiology of depression. Archives of General Psychiatry 34 (1977): 98—11 1.
weitzman, l. j. Sex role socialization. Palo Alto, Cal.: Mayfield, 1979.
weitzman, L. j.; eifler, d.; hokada, e.; and ross, c. Sex role socialization in picture books for preschool children. American Journal of Sociology 77 (1972): 1125–50.
welch, m. r. and page, b. m. Sex differences in childhood socialization patterns in African societies. Sex Roles 7 (1981): 1163—73.
welter, b. The cult of true womanhood, 1820—1860. In Hogeland, R. W., ed., Women and womanhood in America. Lexington, Mass.: Heath, 1973.
wertz, r. w. and wertz, d. c. Lying-in: A history of childbirth in America. New York: Schocken, 1979.
west, j. A child’s day. In Schneiderman, B. K., ed., By and about women. New York: Harcourt Brace Jovanovich, 1973.
westhoff, c. f., calot, G., and foster, a. d. Teenage fertility in developed nations. Family Planning Perspectives 15 (1983): 105—10.
westoff, l. A., and westoff, c. f. From now to zero; Fertility, contraception, and abortion in America. Boston, Mass.: Little, Brown, 1971.
whiting, A. w. m., and child, I. L. Child training and personality. New Haven, Conn.: Yale University Press, 1953.
whiting, b. b., and pope, c. p. A cross-cultural analysis of sex differences in the behavior of children aged three through eleven. Journal of Social Psychology 91 (1973): 171–88.
whittack, f. a., and Edwards, j. e. Pregnancy and attempted suicide. Comprehensive Psychiatry 9 (1968): 1—21.
whitman, w. Leaves of Grass. New York: Modern Library (Random House), 1944.
wideman, m. v. and singer, j. e. Psychological trends in obstetrical practice in American hospitals. Unpublished manuscript, Uniformed Services University of the Health Sciences, Bethesda, Md., 1983.
wideman, m. v. and singer, j. e. The role of psychological mechanisms in preparation for childbirth. American Psychologist 39 (1984): 1357—71.
williams, j. h. Sexual role identification and level of functioning in girls. Joumal of Personality 41 (1973): 1, 1—8.
williams, l. r. Beliefs and attitudes of young girls regarding menstruation. In Golub, S., ed., Menarche. Lexington, Mass.: D.C. Heath, 1983.
williams, v. l. and fish, m. Women’s prison families. In Johnston, N. and Savitz, L. D., eds., Justice and corrections. Somerset NJ.: John Wiley and Sons, 1978.
williamson, n. e. Sex preferences, sex control, and the status of women. Signs: Journal of Women in Culture and Society 1 (1976): 847—62.
willie, c. Marginality and social Tange. Behavior Today, February 25, 1974.
wilson, e. o. Sociobiology: The new synthesis. Cambridge, Mass.: Harvard University Press, 1975.
wingeth, c., and kapp, f. t. The relationship of the manifest content of dreams to duration of childbirth in primiparae. Psychosomatic Medicine 34 (1972): 313–20.
winick, c. The beige epoch: Depolarization of sex roles in America. Medical Aspects of Human Sexuality 3 (1969): 73—74, 78, 80.
wolberg, l. r. The technique of psychotherapy, 2d ed., vols. 1 and 2. New York: Grune &c Stratton, 1967.
WOLFE, l. The sexual profile of that Cosmopolitan girl. Cosmopolitan, September, 1980.
wolff, c. Love between women. London: Duckworth, 1971.
wolff, p. h. A difference that may make no difference. Behavioral and Brain Sciences 3 (1980): 250—51.
wooley, h. t. Psychological literature: A review of the recent literature on the psychology of sex. Psychological Bulletin 1 (1910): 335–42.
woolf, v. Orlando (1928). New York: Harcourt Brace, 1956.
woolf, v. A room of one’s own. London: Hogarth Press, 1931.
woolley, h. t. The psychology of sex. Psychological Bulletin 11 (1914): 353-
Wolman, b. b. Clinical psychology and the philosophy of science. In Wolman, B. B., ed. Handbook of clinical psychology. New York: McGraw-Hill, 1965.
Women on words and images. Dick and Jane as victims: Sex stereotyping in children’s readers. Princeton, N.J.: Princeton University Press, 1972.
wood, c., and suitters, b. The fight for acceptance. Aylesbury, England: Medical and Technical Publishing Company, 1972.
World Health Organization Task Force on Psychosocial Research in Family Planning. Hormonal contraception for men: Acceptability and effects on sexuality. Studies in Family Planning 13 (1982): 328–42.
World Medicine 8 (1973): 55.
Wright, c. t., meadow, a., Abramowitz, s. i., and davidson, c. v. Psychiatric diagnosis as a function of assessor profession and sex. Psychology of Women Quarterly 5 (1980): 240—54.
wylie, p. Generation of vipers. New York: Holt, Rinehart and Winston, 1942.
yarden, p. e., and suranyi, i. The early development of institutionalized children of schizophrenic mothers. Disease of the Nervous System 20 (1968): 380–84.
yorburg, B. Sexual identity: Sex roles and social change. New York: Wiley, 1974. yorke, p. c., and Thomson, d. Anne (1665—1714). Encyclopaedia Britannica.
Chicago: William Benton, 1958.
young, w. c., goy, r. w., and phoenix, c. H. Hormones and sexual behavior. In Money, J., ed., Sex research: New developments. New York: Holt, Rinehart and Winston, 1965.
ziLBOORG, g. Masculine and feminine: Some biological and cultural aspects. In Miller, J. B., Psychoanalysis and women. New York: Brunner / Mazel, 1973.
ziLBOORG, g., and henry, g. w. A history of medical psychology. New York: Norton, 1941.
Zita, J. n. Historical amnesia and the lesbian continuum. Signs: Journal of Women in Culture and Society 7 (1981): 172—87.
ZUCKERMAN, M., NÜRNBERGER, J., GARDINER, S., VANDIVEER, J., BARRET, B., and den breeijen, a. Psychological correlates of somatic complaints in pregnancy and difficulty in childbirth. Journal of Consulting Psychology 27 (1963): 324–29.
zunich, m. Children’s reactions to failure. Journal of Genetic Psychology 104 (1964): 19–24.
Index
abortion;
black women and, 381
chromosomal disorders and, 311
controversy on, 296–99 defined, 290, 292–93 feminism and, 258 history of, 290–92 methods of, 293–94
People’s Republic of China and, 302 psychological effects of, 294–96
Abortion and the Politics of Motherhood (Lu
ker), 296–99
Abraham, Karl, 72
Abrahamsen, D., 429
Abramowitz, S. 1., 458, 469
abstinence, as birth control method, 271—74
Abu-Laban, S. M„ 503
achievement:
birth order and, 215
black women and, 386—88
fear-of-success syndrome and, 211–14 sex differences and, 204—6
single sex environment and, 215—16
socialization and, 206—11
Adams, E., 12zz
Addelson, K. P., 391
Adler, Alfred, 38, 70, 81–85, 96
Adler, F.,421
Adolescent Girl in Conflict, The (Konopka), 412
adolescents:
contraception and, 289—90
delinquency of, 416–19
parental identification and, 185–86
pregnancy of, 288–89, 381
sex experience of, 249, 252, 290
adrenal glands, 108, 113
advertising, 463, 501
affective disorders, 446
Against Our Will (Brownmiller), 442
aggression:
Arapesh tribe and, 91
defined, 165
environmental influences and, 169–71 female victimization and, 425–26 gender differences and, 165–71 hormonal effects on, 112, 167—69 leadership and, 225—26 predisposition toward, 26 social inhibition of, 53
aging:
biological aspects of, 477–79, 490–92 cultural attitudes toward, 476—77, 486, 501–3
double standard of, 493
personality and, 499—501
psychological reactions to, 479—90 sexuality and, 490—94
Albert the Great, 280
Albin, R.S., 428, 429
Alderson prison, 422, 424
Allport, G.W., 25, 220–22
Alnigren, P., 332
Alper, T. G., 510
amenorrhea, 124
American Psychological Association, 468, 471
American Woman’s Home, The (Beecher and Stowe), 342
amniocentesis, 311
analogue studies, 458, 468—69
anal stage of psychosexual development, 32 Andrews, Mrs. (case history), 54–55 androgen insensitivity syndrome, 106–8 androgens:
fetal secretion of, 103–4, 106–9, 111 puberty and, 120–21
see also sex hormones; specific sex hormones anesthesia during childbirth, 313, 316, 319 Angry in Retirement (Hughes), 498—99 animals, sex hormones studies of, 110–13 Anna O. (case history), 30–31
Annas, J., 16
Anne, Queen of England, 205
anorexia nervosa, 124, 447, 453
Anthony, Susan B., 348
anxiety:
castration, 34
defined, 156—57
see also fearfulness
anxiety disorders, 446
Apgar scores, 191
Arapesh tribal society, 91, 92, 94
Are You There God? It’s Me, Margaret
(Blume), 201
Aristotle, 13–14, 15, 291
asceticism, 229, 231
Asher, J., 468
Astin, H. S„ 215
Atlas of Human Sexual Anatomy (Dickinson), 233–34
attachment behavior, 143—44, 160
Augustine, Saint, 9
Austen, Jane, 270
autosomes, 100
Babcock, M. E., 18
Bahr, S. J., 376
Bailey, M. M., 210
Baker, S. W„ 109, 110, 114
Bales, R. E„ 372
Balkan, S., 421
Ballou, M., 470
Barash, D„ 131, 132
Bardwick, J., 208, 254, 284
Barglow, P., 279
Barness, L. A., 335
Barnett, R. C., 479, 480
Barney, Natalie, 400
Barrett, C. J., 497
Barron, F., 223
Bart, P., 243, 484
Bart, P. B„ 480
Baruch, Grace, 352
on aging, 479, 502
on childlessness, 351, 366—67
on working women, 360, 361–62, 480
Basic Human Anatomy and Physiology (Dien
hart), 235, 238
Bates, J. E., 291
battering, 432—39
incidence of, 432–33
societal context of, 433—35
victims of, 436—39, 474
Baumrind, D., 198, 216, 217
Beach, F. A., 110, 111, 228n
Beam, Lura, 233
Beauvoir, Simone de, 1, 2, 3, 7
Becker, E., 484–86
Beecher, Catherine, 342
Beecher, Henry Ward, 5
Bell, A. P„ 409, 410
Bell, J. N„ 436–38
Bell, Quentin, 399
Bell, R. Q., 139
Bello, F., 204n
Bem, S. L., 459
Benbow, C. P., 148
Benditt, J. M., 285
Benedek, T. F., 481
Benson, R. C., 123
Berger, D. G., 229
Berger, R. J., 421
Bermant, G., 118
Bernard, Jessie, 206, 365, 455–56
Berry, J. W„ 153
Besant, Annie, 281
Bettelheim, Bruno, 19
Bibring, G. L., 329
Billings method of birth control, 273—74
biological determinism:
Adler’s rejection of, 81, 84
aggression and, 415
cognitive abilities and, 150—53
Horney and, 72
middle age and, 480
psychoanalysis and, 69
sociobiology and, 132–33
biology:
aging and, 477—79, 490–92
behavior and, 109–10
mental disorders and, 452—53
psychological impact of, 22–23, 40
Bird, C., 489
Birley, J. L. T., 450, 452
Birren, J. E., 478
birth, see childbirth
birth control, 269–304
Catholicism and, 307
China and,299—304
contraception and, 280—88
Erikson on, 67–68
health and, 271
population growth and, 305—6
sexual abstinence and, 271–74
social values and, 270–71
sterilization for, 274—79
teenagers and, 288–90
birth rate, 306, 339
bisexuality, anatomical, 36
Bishop, S., 14, 15
Blackberry Winter (Mead), 90
Blackfoot tribe, 93–94
Blackwell, J. E., 380, 381, 386
black women:
achievement by, 386–88
depression and, 483–84
education of, 385—86
family and, 380–83
racism toward, 377—79
socialization of, 383–85
white vs., 377, 378, 385
widowhood and, 495–96
women’s movement and, 378
Bleier, Ruth, 149
on biological determinism, 97, 99, 110, 134, 509
on hormonal influences, 111, 112, 115
on sociobiology, 132–33
Block, H. A., 417
Block, J. H„ 146, 193
Blume, Judy, 201
Blumstein, P., 410, 411
Boas, Franz, 90
Boccaccio, Giovanni, 4, 394
Bock, W. E., 385
body image, eating disorders and, 449, 454
Boles, D. B„ 150
Bolter, S-, 294
books for children, 195–97
Boskind-White, M., 454
Boston Women’s Health Collective, 201
Bowker, L. H., 418
Bowlby, J., 160, 350
brain:
hormonal effects on, 111–12, 114
lateralization of, 151–52
size of, 17–18
Braine, M. D. S., 138
Brantôme, Seigneur de, 394 breast-feeding, 326, 333—35
Brecher, E. M., 230, 232n, 234, 255
Breines, W., 432
Breit, E. B„ 200
Breuer, Josef, 30—31, 45, 47
Anna O. and, 30–31
seduction theory and, 46
Briscoe, M. L., 12n
Brockett, L. P., 11
Brodsky, C. M., 462, 469
Brody, J. E., 334
Broverman, T. K., 457, 461
Brown, D. G., 182
Brown, G. W., 480
Brown, Judith, 393—95
Brown, W. A., 332
Brownmiller, Susan, 426, 442
Bryson, R., 374 bulimia, 446–47, 453–54
Bullough, V. L., 5, 10, 11, 12
Burgess, A. W., 430, 431
Burlew, A. K„ 387, 388
Burtle, V., 465n
Butler, Eleanor, 396–97
Butler, N. R„ 145
Cade, T., 376
Caesarian delivery, 313, 318
Calvert, R„ 433
Calvin, John, 230
Campbell, A., 479, 488
Campbell, J., 2
cancer, 282, 462
Canterbury Tales (Chaucer), 9
Caplan, P.J., 146, 149, 151,209
career:
black women and, 386–88
commitment to, 370–71
family vs., 210
see also working women
Cartwright, L. K., 223
Casanova, Giovanni Giacomo, 280–81
Cash, W. J., 10
Cassem, N., 497
Castle, C. S., 204
castration anxiety, 34
cathartic method (hypnosis), 30–31
Celestina, La, 281
celibacy, 227, 230
central nervous system:
aging and, 478
infant development of, 137
Chadwick, M., 199
Chamov, A., 162
Charcot, Jean, 30, 81
Chasseguet -Smirgel, J., 55
chastity, see asceticism; virginity
Chaucer, Geoffrey, 9
Chen, P., 300
Chesler, P., 42, 64n
Chesney-Lind, M., 419
Child, 1. L., 169
childbirth, 312–20
alternative experiences in, 319—20
cross-cultural views on, 313–14
delivery room practices in, 315–16
history of, 312–13
labor and,314—15
medical intervention and, 313
postpartum period and, 330–33
preparation for, 316–19
Childbirth Without Fear (Dick-Read), 317
Childhood and Society (Erikson), 57, 58, 61, 65
Childhood Psychopathology (Knopf), 414 childlessness, 351, 353, 365–67
childrearing:
parental authority patterns in, 216–17
sex-typing and, 92–95, 117–18, 191–94
social class and, 141
children:
books for, 195–97
cognitive abilities in, 145–50
desirability of, 306—8
learning processes of, 175–81
nervous disorders in, 448
physical development in, 145–50
problematic behavior in, 413–15
sex-role differentiation and, 23–24
sexual abuse of, 47, 50, 427
sexuality in, 47, 247–49
working mothers and, 371—72, 373—74, 375
China, People’s Republic of, birth control in, 299–304
Ching, C. C„ 300, 301
Chisholm, Shirley, 378
chivalry, 9–10
Chodorow, Nancy, 164–65
Christianity, sexual abstinence and, 229, 231, 272
chromosomal disorders, 101–2, 311
chromosomes, 100–102
cigarettes, pregnancy and, 322
“‘Civilized’ Sexual Morality and Modern Nervous Illness” (Freud), 40
climacterium, 127–28,452–53
see also menopause clitoral sexuality: psychosexual development and, 33, 35, 36–37, 74
vaginal vs., 243–45 clitoris, 104, 236 Coffin, P„ 357 cognitive development:
biological factors in, 150–53 childhood and, 145—50 defined,139
environmental influence on, 153—56 infancy and, 139–41 social class and, 141
cognitive-developmental theory, 175, 178–80
Cohen, D., 478
Cohen, M. L„ 429
coitus, see intercourse, sexual coitus interruptus, 274
Collected Poems of Elinor Wylie (Wylie), 476 Coming of Age in Samoa (Mead), 90—91 Commission on Obscenity and Pornography, 442, 443 communes, 362—64
“Compulsory Heterosexuality and Lesbian Experience” (Rich), 390
computer programming, gender differences and, 197—98
condoms, 280, 287–88
Confrontations with Myself (Deutsch), 56 congenital adrenal hyperplasia (CAH), 108, 112–16
consciousness-raising (CR) groups, 472—74
Constantine, J. M., 363
Constantine, L. L., 363
Constantinople, A., 179 contraception, 280–88 defined, 280 history of, 280—81 men and, 285—86, 287—88 oral, 281—84
People’s Republic of China and, 300, 302 teenage use of, 289—90
Cook, Blanche, 390, 399–400, 459
Cooperstock, R., 462 corpus luteum, 123 corrective action, 470 cortisol, 108
Costello, N. S., 139
couvade syndrome, 322, 323
Cowan, G., 481, 482
Craik, Dinah, 187
CR (consciousness-raising) groups, 472—74 crime, female: increase of, 420—21 male vs., 416, 419—20 menstrual cycle and, 125 socialization and, 419–20 women’s movement and, 421
Criminality of Women, The (Pollack), 419 criminal justice system:
battering and, 434–35, 438–39 girls and, 418–19
see also prison
Crocker, P. L., 440n
Crovitz, E., 381
crying, gender differences in, 142—43
“Cultural Pressures in the Psychology of Women” (Thompson), 78—79
Cutler, R„ 138
Dalton, K., 125, 126
D & E (dilation and evacuation), 293—94
Daniels, Pamela, 370—71
Danza, R„ 202
daughters:
fathersand, 188—90
mothersand, 187—88, 329
parentalpreferencesand, 186—87
Daughters of Bilitis, 401
David, C., 43
David, H. P„ 292, 293
Davidson, C. V., 458, 469
Davie, R„ 145
Davis, K„ 405
Deaux, K„ 172
Defoe, Daniel, 281
Delaney, J., 201
delinquency, juvenile, 416—19
delivery room practices, 315—16
dependency:
attachment behavior vs., 160
gender differences in, 143, 158–61
depression, 455
drug treatment of, 462
ethnic differences and, 483–84
marital status and, 361
menopausal, 479, 482—86
ovarian function and, 453
postpartum period and, 332
pregnancy and,328—29
symptoms of, 446, 482
DES (diethylstilbestrol), 282
Deutsch, Felix, 42
Dora (case history) and, 46
Deutsch, Helene, 50—56
Erikson and, 57
female homosexuality study by, 42
femininity theory of, 52–53, 56
Freud vs., 50—51, 56
masochism viewed by, 53, 75, 428
on menopause, 480, 481,492
on menstruation, 200
sexuality and, 54–55, 244
Deutscher, I., 488
deviance, sex-typing and, 93–94
De Vore, I., 166
Dewey, John, 13
diagnosis, gender differences in, 463–64
Diagnostic and Statistical Manual of Mental
Disorders (DSM III), 446, 448, 449
Dialogue sur les Femmes (Galiani), 124
Diamond, I., 442, 443
diaphragm, 287
Dickinson, Robert, 233—34
Dick-Read, Grandy, 317
Dienhart, C. M., 238
diethylstilbestrol (DES), 282
dilation and evacuation (D & E), 293–94
Diner, H., 2
DiPietro, J. A., 166
disorders:
chromosomal, 101–2,311
eating, 447—48, 450, 453–54
menstrual, 123—25
personality, 447
somatoform, 446—47
substance use, 446
see also mental disorders, sexual dysfunction
Disorders of Sexual Desire (Kaplan), 260
divorce, 357, 381
Dixon, R. B., 24
Doeli, R„ 110, 115
Doherty, M. A., 64n
Dora (case history), 43—47
douches, 288
Douvan, E., 208
Down’s syndrome, 479
Dowty, N., 486
drug prescription, 462—63
Duffy, E„ 158
dysfunctions:
of menstrual cycle, 123—25
see also sexual dysfunction
dysmenorrhea (cramps), 124 dysthymic disorder, see depression
Eagan, A. B., 283
eating disorders, 447—48, 450, 453—54
Eckholm, E„ 271
Eckstein, Emma, 48—50
education, sex, 201
education of women:
blacks and, 385—86
Mill on, 16
Plato on, 15
Rousseau on, 14
sexual harassment and. 440–41
Edwards, J. E., 328
Ehrhardt, A. A., 102, 103, 108, 166, 167
on congenital adrenal hyperplasia (CAH), 113, 114, 115, 116, 163
on sex reassignment, 117–18
Eitner, L., 444
Ellis, Havelock, 232, 398, 403
Embedded Figure Test (EFT), 149, 153, 154
Emile (Rousseau), 14
Emlen, A. C., 365
enchantress-seductress myth, 3—5
Engels, Friedrich, 342
English,]., 13, 15
environment:
aggressive behavior influenced by, 169–71
cognitive development influenced by, 153–56
episiotomy, 315, 318
Equal Employment Opportunity Commis
sion, 440
Equal Rights Amendment, 12
Erikson, Erik, 57–69, 174, 218 Freud vs., 61, 69
inner space theory of, 63—64, 66, 67 psychosocial development, stages of, 57–62, 64–65, 453
erogenous zones, 239
Eron, L. D„ 169–71, 439
erotogenic zones, 32
ESE factor, 355, 357
estrogen, 106
infection and, 130
menopause and, 127–28 menstruation and, 122–23 mood changes and, 452—53 nausea induced by, 309 puberty and, 120—21 Turner’s syndrome and, 101
estrogen replacement therapy (ERT), 491–92
estrous cycle, 111 ethnic minorities, 377n exogamy, 433
Faderman, Lillian, 389, 395, 396, 397, 400 Fallopius, 280 family:
black women and, 380—83 division of labor within, 371–75 types of, 339—40
father:
childbirth involvement of, 316, 319, 322 daughter’s relationship with, 188—90 see also parenthood; parents
fearfulness:
anxiety vs., 156
gender differences in, 142–43, 157–58 Fear of Flying (Jong), 187 fear of success, 211–14 Feinman, C„ 421, 424
Feldman, D. H., 198
“Female Sexuality” (Freud), 34
Feminine Mystique, The. (Friedan), 337 Feminine Psychology (Horney), 74 femininity:
H. Deutsch’s theory of, 52—53, 56 patient role and, 461—62
see also gender identity; gender role identification
“Femininity” (Freud), 28, 34
Feminist Papers, The (Rossi), 342 feminists:
black civil rights and, 378, 379 childbirth viewed by, 320 domestic reform and, 342–43
Erikson criticized by, 64—67
Freud criticized by, 39—41 lesbianism and, 399, 400, 408 libertarian vs. radical, 444 male, 16
marriage viewed by, 355 motherhood viewed by, 348—49 pornography and, 442—44 psychotherapy and, 466—71 rape interpreted by, 431 feminists (continued)
sexuality and, 257–59
working women and, 369, 374
see also women’s movement
Fenichel, Otto, 198
Fennema, E. H., 148, 151
Ferenczi, Sandor, 76—77
Ferguson, Ann, 258, 390–91, 444
Ferrandino, M. M., 200
Feshbach, N. D., 167
Fidell, L. S„ 463, 464
field independence, 149. 153
Figes, E„ 2, 4, 9
Fingerer, M. E., 295
Fish, M„ 423
Fish, S. L„ 473
Fisher. S., 244
Fishman, L. T., 4 18
Fliess, Wilhelm, 48—50
“Flight from Womanhood, The” (Horney), 71, 72
follicle stimulating hormone (FSH), 122–23
Ford. C. S„ 228«
Forrest, J. D„ 277, 279
Fox, L. H., 151, 155
“Fragment of an Analysis of a Case of Hysteria” (Freud), 43
Franks, V., 465n
Franzwa, H. H., 342
free association, 31
Freedman, E. B., 258
Freedman, R., 454
Freud, Anna, 57
Freud, Martha Bernays, 29
Freud, Sigmund, 29–50
Adler and, 38, 70, 81–82
Deutsch vs., 50–51, 56, 69
Dora’s case history and, 43—47
Erikson vs., 61,69
female development theory of, 28, 34–38,40, 185, 243
female masochism view of, 428
feminist criticism of, 39–41, 467
Horney and, 71–77
lesbianism viewed by, 403–4
male psychosexual model of, 2, 34, 218
Mead on, 96
mystery myth and, 7–8
normalcy defined by, 445–46
obsessional jealousy case of, 485—86
personal data on, 29, 232
psychosexual stages theory of, 3 1–34
seduction theory of, 47—50
sexual equality and, 29, 219
Thompson and, 71, 77–81
Friday, N„ 187
Friedan, Betty, 337
frigidity.
concept of, 259, 260
Deutsch on, 55–56
Ellis on, 232
Freud on, 37, 243
see also sexual dysfunction
Frisch, R. E., 124
Frodi, A., 146
Gabalac, N. W., 470
Galdston, I., 294
Galiani, Ferdinando, 124 gangs, teenage, 417–18
Garai, J. E„ 138, 450, 453
Garland, T. N„ 373
Gay American History (Katz), 401
gay liberation movement, 408
Gelles, R. J., 434, 435
gender, sex vs., 135
gender differences:
aggression and, 165–71
biological factors in, 150—53
cognitive development and, 139–41, 146–50
conclusions on, 171—72
defined,135
drug advertising and, 463
infant social behavior and, 142—44
interpretation of, 136–37
medical practice and, 462–65
mental disorders and, 446, 448—50, 479
neonatal period and, 138–39
nurturance and, 162—65
suicide and, 450–51
variability factor vs., 172
see also sex differences
gender identity, 98–99
sexual reassignment and, 1 16–18
variations of, 118—19
gender-role identification:
adoption of behavior and, 183
development of, 181–84
learning theories and, 175—81
parental vs., 175
preference in, 181–83
sex differences and, 183–84
see also gender identity; sex typing genitalia, see sex organs
genital stage of psychosexual development, 33
genius, 205
Gerson, M-J„ 306, 308, 348
Giallombardo, R., 422, 423
Gibson, L., 198
Gilbert, S. M., 399
Gilkes, C. T„ 387
Gillespie, D. L., 376
Gilligan, Carol, 219–20, 510
Gilman, Charlotte Perkins. 349
Girlhood (Deutsch), 54
girls, see adolescents; children; daughters
Goldfarb, W., 414
Goldfoot, D., 112
Goldstein, L., 439–40
Golub. Sharon, 202, 243, 334
gonads, 100–102
see also sex hormones
Gordon, K. K., 333
Gordon, L., 432
Gordon, R. E., 333
Gorky, Maxim, 59, 60
Gossypol, 285
Gove, W. R., 450, 454
Goy, R. W„ 99, 110, 112, 113, 164, 168
Grady, K. L., Ill
Graebner, D. B., 196
Graefenberg, E., 281
Graham, H., 305
Gray, M„ 148
Greenberg, N., 102
Greenberg, N. H., 329
Greenspan, M. A., 465n, 466
Grimes, D. A., 293, 294
Grimke, Sarah, 343
Grossman, M., 480
Groth, A. N„ 431
Grunbaum, A., 38, 39
Gubar, S., 399
Gump, J. P„ 369, 385, 387
Gutmann, D. L., 181, 500, 501
Hall, Radclyffe, 399, 400, 402
Haller, J. S., 11, 230, 231
Haller, R. M., 11, 230, 231
Halverson, C. F., Jr., 159
Handbook of Obstetrics and Gynecology (Benson), 123
Hare-Mustin, R. T., 465n. 466
Harlow, H„ 162, 166, 350
Hatcher, R. A., 273, 275, 292
Hayler, B„ 292
Hayner, N., 425
health care, for female patients, 461–63
health maintenance, 470
Heffernan, E., 422
Hefner, R., 181
Heilbrun, A. B„ 185, 186, 460
“Heinz dilemma,” 218
Hennig, M., 215
Henley, N. M.,510
Henshaw, S. K., 277, 279
Hesiod, 5
Heyman, K., 165
Hier, D. B„ 152
Higham, E., 246
Hilberman, E., 426, 430—31
Hill, K. T„ 157
Hill, R„ 383
Himes, Norman, 269
Hitchcock, J. T., 174
Hite, Shere, 227, 252, 257
Hite Report, The (Hite), 227, 257
Hitler, Adolf, 59, 60
Hoffman, L. W., 213, 214
on interpretation of gender differences, 136, 137
on parenthood, 306, 308, 349
on working women, 368, 369
Hoffman, M. L., 306, 308
Hogan, D. F., 381
holistic approach, defined, 72
Hollingworth, Leta Stetter, 85—90, 96
Holmes, F. B., 157
Holmstrom, L., 430 home birth, 319–20 homosexuality:
childhood, 247
male vs. lesbian, 391–92, 393, 394, 401
prison systems of, 423–24
sexual preference development and, 409 see also lesbianism
homosexuals, relationships between, 411
Horgan, C. M., 448
Horner, M. S., 21, 211, 212
Horney, Karen, 72–77, 96, 446
Freud and, 71, 72, 73 hospitals:
breast-feeding in, 334
childbirth in, 312–13, 315–16, 318–19, 320
mother-infant bonding and, 330–31
Houseknecht, S. K., 366 housewife role:
depression and, 483–84, 485–86 domestic reform movement and, 342—43 housewives’ views of, 345–46
other occupations vs., 343–45 promotion of, 341–42
Howard, E. M., 424
Howard, J. L., 424
Howell, M. C., 462, 465
Hrdy, S. B„ 166
Hughes, E., 498–99
Human Sexual Response (Masters and Johnson), 235
Hunt, M., 246, 249, 250, 408 husbands;
childbirth involvement of, 316, 319, 322 domestic chores and, 371–75
family role of, 347–48 see also marriage
H-Y antigen, 100
hymen, 236
hypnosis (cathartic method), 30–31 hypothalamus, 111
menstruation and, 122–23, 124 puberty and, 119–20
hysterectomy, 275–76, 279, 462 hysteria:
Charcot on, 30
Dora’s case history of, 43—47
Freud’s seduction theory and, 47, 50 repression and, 31
Ideal Marriage (van de Velde), 233
Iglitzin, L. B., 207–8 illegitimacy rate, 381 Immodest Acts (Brown), 393—95 impotence, 493
In a Different Voice (Gilligan), 219—20
Individual Psychology, 81 infanticide, female, 303–4 infants.
cognitive development in, 139—41 defined, 137??,
infants (continued)
early bonding with, 330–32
physical development in, 137–38
premature, 312
sexuality of, 32, 246–47
social and affective behavior in, 142–44 inhibited sexual desire (1SD), 260, 266 “Inner and Outer Space, The” (Erikson), 57 inner space, Erikson’s concept of, 63–64, 66, 67
“In Praise of Older Women,” 502
In Search of Our Mothers’ Gardens (Walker), 174
instrumental competence, 217 intellectual ability:
aging and, 478
social class and, 141
variability hypothesis and, 205 intercourse, sexual:
adolescent experience of, 249, 252 pregnancy and, 242–43, 323–26
sexual response and, 239—42
sexual revolution and, 250—53
Victorianism and, 230, 231
interests, values and, 220—26
internal reproductive system, 237–38 Interpretation of Dreams, The (Freud), 81 intimacy, 453
intrauterine device (IUD), 281, 286, 302
IT scale, 177
Jacklin, Carol, 18, 21
on children’s gender differences, 146–47, 149, 150, 157–59, 166–67, 177, 178, 205
on infant development, 140, 143, 144
on socialization of children, 182, 192, 193, 194, 415
Jackson, J. J., 386
Jacobson, W. D., 376
Jakobovits, I., 291
James, W. H„ 321
James, William, 13
Janeway, E., 2, 64«
Jelliffe, D. B., 335
Jelliffe, E. F. P„ 335
Jersild, A. T., 157
Jewish mother, 483–84
John, K. E., 422
Johnson, Samuel, 173
Johnson, Virginia:
on aging and sexuality, 491, 493
on female orgasms, 228, 242, 244—45
on pregnancy and sexuality, 324–26
on sexual dysfunction, 260, 262, 268
on sexual response cycle, 234—35, 239
Jones, Ernest, 8, 29, 31«, 39
Jong, Erica, 187
Joslyn, W. D., 168
Jost, A., 106
jourard, S. M., 159
juvenile delinquency, 416—19
Kagan, Jerome, 456
on childhood development, 154, 160, 214
on infant gender differences, 143, 144
on infant sex differences, 137, 140—41 Kaplan, Helen Singer, 260, 261«, 265—68 Kaplan, J., 152, 254
Karie, Isabella, 215
Karie, Jerome, 215
Karmel, Marjorie, 317
Katchadourian, IL, 228«, 234, 309«, 322
Katz, Jonathan, 401
Katz, S„ 426, 431
Kaufman, S. A., 277
Kearney, H. R., 366
Kelman, Harold, 72«, 74
Kennell, J., 331
Kiesler, S., 366
Kimball, M. M„ 149
Kimmel, D. C., 478
Kinsey, Alfred, 234, 246–54, 405, 407–8
Kisker, E. E„ 289, 290
Kitzinger, S., 163
Klaich, D„ 393
Klaus, M. H„ 331
Kleiman, D., 211
Klein, V., 341
Klinefelter’s syndrome, 101, 102
Kluckhohn, C., 26
Knopf, Irwin J., 414
Koff, E., 204
Kogan, N., 154
Kohlberg, Lawrence, 178, 218–19, 220
Konopka, Gisela, 224
on adolescent problems, 412, 417
on menstruation, 200, 201
on mother-daughter relationships, 188, 189
Koten, J., 479
Krafft-Ebing, Richard von, 402–3, 404
Kravetz, D., 474
Kreuz, L. E., 168
Krieger, Susan, 405—7
Kuhn, T. S., 65«
Kummer, H., 162
Kushner, H. L, 451
Kutner, S. J., 327
labia, 104, 236
labor in childbirth, 314–15
lactation, 333
Ladder, The (Daughters of Bilitis), 401
Ladner, Joyce, 200, 208, 379, 382, 384
Lamaze, Fernand, 317–19
Lamaze method of childbirth, 317–19
Lamb, J., 189
Lamb, M. E., 189
Lambert, H. H., 150, 151, 152, 164
Lambert, W. E., 192, 194
Lampl-De Groot, Jeanne, 42
Land, Edwin H., 204«
Landers, Ann, 257
laparascopic sterilization, 275
latency stage of psychosexual development, 33
Launois, J., 415«
leadership, sex differences and, 225—26
Lear, M. W., 358n
learning, theory of, 175–81
cognitive-developmental, 178–80
modeling, 176—78
reinforcement, 175—76
I.eboyer, Frederick, 315—16
legal system:
battering and, 438–39
sexual harassment and, 440, 441
see also criminal justice system; prison
Leifer, M., 305, 330
Lemkau, J. P., 215
Lennane, K. J., 124
Lennane, R. J., 124
Leonard, E. B., 420, 421
Lerner, G., 378
Lerner, I. Michael, 128–29
lesbianism:
contemporary tolerance of, 407–8 cultural tradition of, 399–401
defined, 389–92, 408
history of, 393—99
incidence of, 408
male homosexuality vs., 391–92, 393, 394, 401
pathology-oriented view of, 401–4 political implications of, 409—10
prison family systems and, 423 romantic friendship and, 396–99, 401, 403
sexuality of, 398, 410–11
sexual preference development and, 409
social context studies on, 405—7
stereotypes and, 410
word derivation of, 393
Lesbian/Woman (Martin and Lyon), 410
Leventhal, G., 421
Levinson, D. G., 370
Lévi-Strauss, Claude, 228, 433
Levy, J., 151
Levy, J. M„ 296
Lewis, D. K., 378, 386
Lewis, M,, 144
Lewis, Oscar, 93–94
Libby, William J,, 128—29
libido:
defined, 32
genital stage of psychosexual development and,33
sex differences and, 36
life chances, 24
life expectancy, 478—79
Lincoln, R., 288—89
Lindzey, G., 222
Linn, L., 463
Loesch, J. G., 329
Lombroso, Cesare, 419
London, P., 20«
Longino, H., 1 10, 1 15, 441
Looking Back (Maynard), 174
Lopata, H. Z„ 339, 344
on motherhood role, 66, 350, 352
on widowhood, 495—97
Lowenthal, M. F,, 479
Luker, Kristin, 296—99
Lunde, D. T„ 167, 228«, 234, 309«, 322
Luther, Martin, 229–30
Lynn, D. B„ 181, 187, 190
Lyon, Phyllis, 410
McCaldon, R. J,, 429
McCaryJ. L„ 273, 321, 333
Maccoby, Eleanor, 18, 21
on children’s gender differences, 146—47, 149, 150, 157–59, 166–67, 177, 178, 205
on infant development, 140, 143, 144
on socialization of children, 192, 193, 194, 415
McDermott, M. J., 427
McEwen, B. S„ 99, 112, 113, 164
Macfarlane, A., 312, 320
McGuinness, D., 151
MacLeish, K., 415«
McLeod, B., 253
Magrab, P. R., 187
Mainardi, P., 343
Male and Female (Mead), 305
Malthus, Thomas, 272, 281
Mamay, P. D., 195
Man and Woman, Boy and Girl (Money and
Ehrhardt), 103
Mann, H„ 395
Margolin, G., 189
Mark, E. W., 510
marriage:
alternatives to, 360—64
black women and, 380
Christian views of, 229—30, 272
current trends in, 355—57
Freud on, 40
group, 362
life cycle and, 338—39
mental disorders and, 450
open, 357—60
origin of, 433
parenthood effects on, 353—54
physical assault and, 433—34
prison homosexuality and, 423
sexual liberation and, 250—51
shock theory of, 455—56
suicide rates and, 451–52
working women and, 338, 360, 367—68, 371–77
see also housewife role
Marshall, D. S., 228«
Martin, D., 432–33
Martin, Del, 410
Martin, L„ 152, 153
Martina (Navratilova), 389
masculinity, 67
see also gender identity; gender role identification
masculinity complex, 35, 53, 56, 74, 80
Maslow, Abraham, 358, 460–61
masochism:
Deutsch on, 53
Erikson on, 67
Horney on, 75—76
Masson, Jeffrey, 47, 49
Masters, William:
on aging and sexuality, 491, 493
on female orgasms, 228, 242, 244–45
on pregnancy and sexuality, 324–26
on sexual dysfunction, 260, 262, 268
on sexual response cycle, 234–35, 239
masturbation:
children and, 248–49
Freud on, 32–33, 34, 35
lesbianism and, 403
Victorian view of, 230
maternal behavior, see nurturance
maternal instinct, 19
Hollingworth on, 88, 89
maternity ratio, 269—70 see also birth rate
mathematical ability, 147–49, 151, 156
matriarchy, black, 378, 380–81, 382
May, R„ 21
May, Rollo, 13
Maynard, Joyce, 174
Mazur, M. A., 426, 431
Mead, Margaret, 71—72, 90—96, 305
on equality of gender roles, 375, 471
on sex differences, 91–92, 96, 165
Means, C. C., 291
Medea, A., 431
Medical History of Contraception, The (Himes), 269
medical practice:
gender bias in, 462–65
menopause and, 481
medical training, sexism in, 464–65
Medina, Lina, 121
Mednick, M. T. S., 208, 212
Mein Kampf (Hitler), 60
menarche, 118, 120, 199–204
Menarche (Golub), 202
menopause:
depression and, 479, 482—86
medical profession and, 481
sexuality and, 490
symbolic meaning of, 480
women’s response to, 480–82
menstruation:
adolescent attitudes on, 201, 202—4
androgen studies on, 111
behavior and, 125—26
climacterium and, 126—27
cultural beliefs and, 121–22, 199
cycle of, 122–23
dysfunctions in, 123–25
onset of, 118, 120, 199–204
sex drive and, 243
women’s performance and, 22—23, 86–87 mental disorders:
attitudes toward, 445 classifications of, 446–48
gender differences and, 446, 448—50, 479
gender roles and, 454—56
marriage and, 450
social roles and, 453—57
suicide and, 446, 450
women’s biology and, 452—53
work and, 480
see also specific disorders
mental health:
double standard for, 457—59
feminist model of, 470
Freud on, 445–46
Meyer-Bahlburg, H. F. L., 114, 115 middle age, see aging; menopause midwives, 312, 319–20 milk, human, 334, 335
Mill, John Stuart, 16, 20, 29, 89, 217, 34243
Miller, A. L„ 370
Miller, J. B., 43n
Milton, John, 5—6
Mind of the South, The (Cash), 10
Minton, C., 193
Minturn, L., 174
Mirror Dance, The (Krieger), 405—7 miscarriages, 310–11, 324
Mischel, W., 143, 160
misogyny, 5, 13—15
Mitchell, J., 36, 40–41
Mitchell, Joni, 370 modeling, 175, 176–78 “Mom” stereotype, 59–60
Money,John, 22, 102, 103, 108, 111, 167, 168, 395
on congenital adrenal hyperplasia (CAH), 113, 114, 115, 116, 163
on sex reassignment, 117—18 mongolism, 479
Moore, D., 432, 435
moral development, 218–20
Moral Judgment of the Child, The (Piaget), 218
Moran, R„ 356
morning sickness, 309
mortality, sex differences in, 129–30
Morton, J. H., 125
Moss, H. A., 142, 160, 214
mother-daughter relationship, 187–88 pregnancy and, 329
motherhood:
careers and, 16, 19, 56
emotional experience of, 348–55
Erikson’s view of, 65–66
future of, 364–65
Hollingworth on, 88—89
Jewish, 483–84
male envy of, 66, 74
marriage affected by, 353–54 middle age and, 483, 484, 487–89
sexuality vs., 325–26
working women and, 371–72, 373–74, 375
see also parenthood
Motherhood (Deutsch), 54 mother-infant bonding, 330–32 mother nature myth, 2—3, 8
Moulton, J., 15
Moynihan, Daniel, 382
Mullerian ducts, 102–3, 104
Mullerian inhibiting substance, 103, 104, 106–8
Muncy, R. L., 363
Mundugumor tribal society, 91, 92, 94
Murai, N., 321
Murray, H. A., 26
Mussen, P. H., 177
mystery, mythic woman and, 6–8
mythic woman, 1–8
enchantress-seductress as, 3—5
mother nature as, 2–3, 8
mystery and, 6–8
necessary evil and, 5–6, 8
virtue and, 8—12
Nahum, L. H., 311
narcissism, 37, 52
Nash, S. C-, 154, 155, 156
Navratilova, Martina, 389
necessary evil myth, 5–6
Negro Family, The (Moynihan), 382 neonatal period, 137n, 138—39 Neugarten, B. L., 181, 482, 500, 501
Neurosis and Human Growth (Horney), 77
Neurotic Personality of Our Time, The (Hor
ney), 76–77
Newland, K„ 271, 371
New Our Bodies, Our Selves, The (Boston
Women’s Health Collective), 201, 465
New Sex Therapy, The (Kaplan), 260
Newson, E., 193
Newson, J., 193
Newton, M., 313, 314, 335
Newton, N., 313, 314
New Woman, 402
Niederhoffer, A., 417
Nietzsche, Friedrich, 14–15
Nilsson, A., 332
normative behavior, 412–13
Norplant, 284–85
Nortman, D., 479 nurse-midwives, 319–20 nurturance:
animal patterns of, 160—61
defined, 161
gender differences in, 162—65
psychoanalytic analysis of, 164—65
O’Brien, J. S„ 311
obstetrics, 313, 314, 318
see also childbirth
O’Connor, A. N., 86
Oedipal conflict, 43
Oedipus complex, 33–34
Oedipus Rex (Sophocles), 29
Oetzel, R. M., 166
Of Woman Born (Rich), 352—53
Oliver, W. A., 318
“Once More the Inner Space” (Erikson), 57
Oneida colony, 274
O’Neill, G., 355, 357
O’Neill, N., 355, 357
On the Subjection of Women (Mill), 16, 29
On Women (Schopenhauer), 6 oophorectomy, 275–76 oral contraceptives, 281–84 oral stage of psychosexual development, 32 orgasm:
aging and, 490–91
Deutsch on, 55—56
physiology of, 241–43
sexual dysfunction and, 261, 267 sexual inhibition and, 254—57
vaginal vs. clitoral, 243–45
variability in, 227–28
Victorianism and, 231
see also intercourse, sexual; sexual behavior
Orlando (Woolf), 399
Our Right to Love (Vida), 401
Outline of Psychoanalysis, An (Freud), 32 ovaries, 237–38 ovulation:
defined, 122
decline of, 126 oxytocin, 314, 333
Page, B. M., 194
Palm, R., 429
Paradise Lost (Milton), 5—6 parental identification:
adolescent girls and, 185—86
defined, 174, 184
mothers and, 183 parenthood:
marriage affected by, 353–54 motivations for, 306—8
religious views on, 307
see also motherhood; postparental life parents:
authority patterns of, 216
relationship of daughter and, 186–90 sex-typing influences of, 190–94
Parke, R., 163
Parks, M., 303
Parlee, M. B., 125, 509, 510
Parsons, Talcott, 372, 417 parturition, 314
see also childbirth passivity:
Deutsch on, 52–53
Freud on, 36
medieval woman and, 10
Paterson, E. J., 434–35, 438 patients, female, 461—63
Patterson, G. R., 189
Payak, B., 419
Pendergrass, V. E., 448
penis, 104
penis envy:
Deutsch on, 43
Erikson on, 63, 67
Freud’s theory of, 34–35, 37, 38–39
Horney on, 74
Mead on, 96
Thompson on, 78—79
Peplau, L. A., 411
Perlmutter, J. F., 321, 480
Perry, J. B., Jr., 365
personality:
Adler’s theory of, 83
aging and, 499—501
androgynous model of, 459—61
defined, 25
development of, 26
masculine ideal model for, 457—59 psychoanalytic theories of, 69–70 reproductive function and, 96 sex-typing and, 93–95, 198–99 temperament vs., 25–26
personality disorders, 447
perversity, polymorphous, 32
Petersen, A. C., 152
Peterson, J., 139
phallic stage of psychosexual development, 33
Phillips, D„ 456
philosophy:
misogyny in, 13—15
sexual equality in, 15–16
phobias, 446
Phoenix, C. H., 168
physical development:
in childhood, 145
in infancy, 137—38
in puberty, 118–21 physicians, see medical practice Piaget, Jean, 218
Pierce, C., 15
Pill (oral contraception), 282–84
Pinel, Philippe, 445
pituitary gland:
function of, 111
menstruation and, 122–23, 124
puberty and, 119—21
placenta, 310, 312
Plato, 15
Playboy Foundation survey, 246, 248–52, 408
Pieck, J. H., 374–75
PMS (premenstrual syndrome), 124–25, 126
Pollack, Otto, 419
Poloma, M. M., 373, 376
polymorphous perversity, 32
Ponsonby, Sarah, 396–97
Pope, C. P., 166
pornography:
defined, 441
feminist attacks on, 442–44
liberal interpretation of, 442 traditional view of, 441—42
Porteus, S., 18
Portnoy’s Complaint (Roth), 484 postparental life, 483, 487—89 postpartum period, 330—33 potency, 128, 491, 493
Powell, G.J., 382, 383, 388
Prather, J., 463
pregnancy:
adolescents and 288—89, 381
attitudes toward, 305
drugs taken during, 321—22
emotional effects on, 320–21
imitations of, 322–23
orgasm in, 242—43, 323—24
physiological events of, 309—12
psychological aspects of, 326—30
safest age for, 271
sexuality and, 242–43, 323–26
tests for, 310
see also birth control
premature babies, 312 premenstrual syndrome (PMS), 124—25, 126
Prendergast, P., 385
prescription of drugs, 462–63
Presser, H. B., 279
Preston, L., 422, 425
Price, R. R., 423, 425
Pringle, M. L. K., 145
prison:
homosexuality in, 423–24
rehabilitation and, 424–25
sex ratio in, 421–22
social systems in, 422–23
women’s families and, 425
problem behavior:
sex differences in, 413–15
societal classifications of, 416
see also crime, female; delinquency, juvenile; mental disorders
“Problem of Feminine Masochism, The”
(Horney), 75
progesterone, 106
contraceptive use of, 282
infectious agents and, 130
PMS and, 126
prostitutes, 4—5 pseudocyesis, 322—23 psychoanalysis, 28–29
authoritarian approach of, 467—68
Horney on, 72, 73
interpersonal, 78
menarche viewed in, 199—200
patriarchal society and, 38–42
psychology vs., 38, 42
seduction theory and, 47, 50
sexual dysfunction and, 262, 263, 265
subjectivity of, 42—43
traditional views of women in, 69—70 see also psychotherapy; specific analysts “Psychogenesis of a Case of Homosexuality in a Woman, The” (Freud), 403—4 psychology:
behaviorist school of, 19 biological factors in, 22–23 early development of, 17 philosophical origins of, 12–13 psychoanalysis vs., 38, 42 see also psychoanalysis; psychotherapy
Psychology of Sex Differences, The (Maccoby and Jacklin), 146–47
Psychology of Women (Deutsch), 42 psychoprophylactic method (PPM) of childbirth, 317–19
psychosexual development, Freud’s theory on, 31–34
psychosocial development, Erikson on, 57–59, 64–65
psychotherapy: alternatives to, 472–75 defined,465
feminist values in, 469—71 psychoanalysis and, 467–68 sex bias in, 466—69
puberty, 119–21 delinquency and, 417 sociosexual activity in, 249 see also adolescents
Puner, M., 490n, 493
Puritanism, 5, 60
racism, 377—79
Radloff, L., 361
Rainwater, L., 307
Ramey, J., 364
Rand, L. M., 370 rape, forcible: defined,426 feminist interpretation of, 431 homosexual, 427 incidence of, 427 pornography and, 442, 443 psychological reaction to, 429—31,474 resistance to, 428 statutory vs., 426 theories on, 428–29
Roy, P„ 372
Read method of childbirth, 317, 318, 319 rehabilitation programs, 424—25 reinforcement, 175–76 religion, parenthood and, 307 Renne, K. S„ 353 repression, 31, 34 reproductive system, internal, 237–39 Republic, The (Plato), 15 Rheingold, J. C., 188 rhythm method, 272—73
Rich, Adrienne, 352–53, 390–92, 409–10 Riesman, D., 368
Riopelle, A. J., 479
Ritter, C. A., 313
Rivenbark, W. H., Ill, 159
Rivers, L. W„ 385, 387
Rodgers, D. A., 277
Rodman, H., 296
Roe vs. Wade, 292
Rogers, C. M., 479
Rogers, K., 6
Rogers, K. O., 418
romantic friendship, 396—99, 40In, 403
Romanticism, 230
Room of One’s Own, A (Woolf), 205—6
Rosaldo, M. Z., 23
Rose, R. M„ 168
Rosen, D. H., 404
Rosen, J. L„ 500
Rosenberg, K. M., 162
Rosenblatt, J. S., 162
Rosenhan, D., 20n
Ross, E„ 227
Rossi, Alice:
biosocial perspective of, 133, 164
on feminist writers, 205, 342, 348–49
Roth, Philip, 484
Rothbart, M. K„ 141, 193
Rousseau, Jean Jacques, 14–15
Rowe, I. L., 462
Rubin, J. Z„ 191
Rubin, R. T„ 126
Rugoff, M„ 230
Russell, D. E. H., 443, 444
Russo, N. F„ 86, 349, 448, 450, 455, 462
Rutherford, E., 177
Sachs, Hanns, 72
Sackville-West, Vita, 399
Sadd, S., 252
Safilios-Rothschild, C., 476
St.John-Parsons, D., 373
Sampson, Deborah, 395
sapphism, 392
Sappho, 392n, 393
Sarason, S. B., 157
Sarvis, B., 296
Sato, T., 321
Saucier, J. F., 323, 325
Schaar, K., 451
Schaefer, Leah, 255
Schafer, A., 148
Scheinfeld, A., 138
Scherl, D., 430
Schildkraut, J. J., 328
schizophrenia, sex differences and, 415, 450
Scholastic Aptitude Test (SAT), 148–49 school:
sex typing in, 197—98
sexual harassment in, 440—41
“School-Friendships of Girls, The,” (Ellis), 398
Schopenhauer, Friedrich, 6
Schwartz, P., 410, 411
Schweitzer, Albert, 77
Science and Gender (Bleier), 97, 134, 509
Scully, D., 243
Sears, P. S., 198
Sears, R. R., 176, 189
Second Sex, The (de Beauvoir), 1 Second Stage, The (Friedan), 337 seduction theory, 47–50 Segal, B„ 456 self actualization, 460–61 sex, gender vs., 135
Sex and Temperament in Three Primitive Societies (Mead), 91 sex differences:
achievement and, 204–6
aggression and, 26 aging and, 478–79 biological determination of, 98 biological vs. psychological, 22 brain size and, 17—18
childhood development and, 145—50 childhood problematic behavior and, 415–17
crime and, 416, 419–20
Freud on, 21
gender identity and, 98–99
genetic determinants of, 99—102
hormonal determinants of, 99–100, 102— 9
infant development and, 137—44 juvenile delinquency and, 416—19 leadership and, 225—26 life cycle and, 128 masculine criteria and, 20–21 Mead’s work on, 91—92, 96 mortality and, 129–30,479 nurturant behavior and, 19 opportunities influenced by, 24 psychosexual development and, 32–38 reproductive capacity and, 479 schizophrenia and, 415 sexuality and, 257 socialization and, 23–24 spatial organization and, 62, 66–67 values and, 220–25 variability hypothesis and, 18 sex education, 201 sex hormones:
androgenic, 103–4
animal studies and, 110–13 breast-feeding and, 333 contraceptive use of, 282–83, 284–86 human behavior studies and, 113–16 nurturant behavior and, 161–62 pregnancy and, 309, 310, 328, 332 see also specific hormones
sexism:
achievement and, 206 psychotherapy and, 466–69 sex organs:
anatomy of, 235—37
fetal development of, 104
see also specific organs sex ratio, 128–29, 303n sex reassignment, 117–19 sex roles:
age-related perceptions of, 500–501
sociobiology and, 131–32
see also gender-role identification
sex therapy, 265–66
see also sexual dysfunction
sex typing, 174–75
children’s books and, 195–97
childhood career choices and, 207–8
Mead on, 93—95
parental influences on, 191–94
school experiences and, 196—97
socialization and, 190–91
stereotyping vs., 191
television and, 195
see also gender role identification “Sexual Aberrations, The” (Freud), 403, 404
sexual abuse of children, 47, 50, 427
sexual anatomy, 235
external, 235–37
internal, 237–39
sexual behavior:
defined, 245–46
development of, 246–49
juvenile criminal justice and, 418–19
revolution in, 249–53
women’s attitudes toward, 254–57
Sexual Behavior in the Human Female (Kinsey), 234
Sexual Behavior in the Human Male (Kinsey), 234
sexual dimorphism:
human behavior and, 115–16
see also gender differences; sex differences
sexual dysfunction, 259–68
etiology of, 262–65
treatment of, 265–68
types of, 269–62
sexual harassment, 439–41
sexual intercourse, see intercourse, sexual sexuality:
aging and, 490–94
children and, 47, 247–49
Deutsch on, 54–55
feminism and, 257—59
historical perspective on, 228–29
infants and, 32, 246–47
lesbianism and, 398, 410—11
motherhood vs., 325–26
pornography and, 442—44
pregnancy and,242–43, 323–26
rape and, 429, 431
scientific study of, 232–35
Thompson on, 80–81
Victorianism and, 230–32
sexual preference, development of, 409 sexual response, physiology of, 239–42 Shah, F„249
Shanan,J., 124
Shaw, George Bernard, 12n
Sheldon, E. B., 339, 340
shelters for battered women, 437–38, 474
Shephard, B. D., 310, 319, 322
Shephard, C. A., 310, 319, 322
Shepherd, W., 139
Shereshefsky, P., 332
Sherfey, M. J., 236, 242n, 243, 244
Sherman, J., 148, 151, 152, 182, 482
Shields, S. A., 17, 18, 19, 205
Shope, D. F„ 255, 261
Shostak, Marjorie, 199
Shusterman, L. R., 296
Sidel, R., 169
Silka, L., 366
Silvers, W. K„ 100
Simpson, E. L., 219
Simpson, R. L., 195
Singer, I., 244
Singer, J., 244
Singer, J. E„ 138, 318–19
Singer, Laura, 358n
single life, 356–57, 361–62
Single Woman, The (Dickinson and Beam), 233
Sioux tribal society, 61–62, 65, 66
Skinner, B. F„ 354–55
Smith, E.J., 385
Smith-Rosenberg, Carol, 396, 397
Snuff, 443
social class, 141
“Social Devices for Impelling Women to Bear and Rear Children” (Hollingworth), 88
socialization:
achievement and, 206–11
black women and, 383—85
childhood problematic behavior and, 414–15
crime and, 419–20
mental disorders and, 453–57
sex-role differentiation and, 23–24
sex typing and, 190—91
sociobiology, 131—33
Sociobiology (Wilson), 131
Solberg, D. A., 324
somatoform disorders, 446—47
“Some Psychical Consequences of the Anatomical Distinction between the Sexes” (Freud), 34
Sophocles, 29
Soranos of Ephesus, 280
Sorenson, R., 408
spatial ability, 149—50
biological factors in, 150–51
environmental influence on, 153–55
sex differences in, 62, 66–67
Spence, J. T., 460
Spitz, R., 350
Spranger, E., 220
Sprenger, Jacob, 4—5
Squires, S., 257
Stafford, R. E., 151
Stanley, J. C., 148
Stanton, Elizabeth Cady, 343
Staples, R., 382
statutory rape, 426
Stein, A. H„ 210
Steinmann, A., 381
Steklis, H. D„ 113
stereotypes:
children and, 180
departure from, 181
early psychology and, 12—16
fallacy of, 455–56
lesbianism and, 410
“Mom,” 59–60
sex typing vs., 191
virtuous woman, 8—12
sterilization, 274–79
China and, 301–2
incidence of, 276–77
psychological effects of, 277–79
types of, 274–76
Sterling, D. H„ 385
Stewart, I., 125
Stimpson, Catharine, 392n
Stoller, R.J., 22
Stowe, Harriet Beecher, 342
Stricker, G., 468
Striegel-Moore, R. H., 454
Strouse, J., 43n
Studies in Hysteria (Freud and Breuer), 31, 47
Studies in the Psychology of Sex (Ellis), 232
Study of Mathematically Precocious Youth, 148–49
submissiveness, 8—9
Mill on, 16
Victorian woman and, 10—11
substance use disorders, 446
success, fear of, 211–14
Suggs, R. C., 228n
suicide, 450–52
marital status and, 451–52
depression and, 446
Suitters, B., 269, 270, 280, 281
Sullivan, Harry Stack, 78
superego, 38
superwoman model, 210–11
Supreme Court, U.S., 292
Suranyi, I., 321
Surpassing the Love of Men (Faderman), 389
Sutherland, S., 430
Sutherland, H., 125
Sutherland, S. L., 213
Sviland, M. A. P.,492
Swanson, H. H„ 110, 111
Szasz, Thomas, 445
Table Talk (Luther), 229—30
Tanner, J. M„ 119, 137n, 144
Tänzer, D., 318
Taube, C. A., 448
Taussig, F. J., 291
Tavris, C., 252
Taylor, C. W„ 223
Tay-Sachs’ disease, 311
Tchambuli tribal society, 91–92, 93, 94, 98
“Technique of Psychoanalytic Therapy, The” (Horney), 72
teenagers, see adolescents television, 170—71, 195 temperament, defined, 25—26 Terman, L. M„ 204, 345, 448 testicular feminizing syndrome, 106–8 testosterone, 104, 106
aggression and, 112—13
puberty and, 121
Thank You, Dr. Lamaze (Karmel), 317 therapy, see psychotherapy; sex therapy
Thomas Aquinas, Saint, 393–94
Thompson, Clara, 77–81, 96
on menstruation, 200
Thompson, K., 431
Thomson, D., 205
Thorndike, Edward, 87
Thorne, B , 258
Thousand Marriages, A (Dickinson and
Beam), 233
Three Essays on the Theory of Sexuality (Freud), 31–32, 34
Tidball, M. E., 216
Tobin, P., 154
tomboyism, 114, 115—16, 168
Tomorrow’s Tomorrow (Ladner), 384 traditional roles:
adaptations of, 371—77 black women and, 377—88 departures from, 355—67 housewife as, 340–48 life cycles and, 338—39 mother as, 348—55 psychotherapy and, 466, 468 work vs., 367–71
transference, defined, 45 transsexualism, defined, 118 transvestism, 118, 395—96
Treadway, C. R„ 327, 328
Tresemer, D. W., 212
tubal sterilization, 275, 277, 279
Tudor, J. F., 454
Turkington, C., 126
Turner’s syndrome, 101—2
Tylden, E., 327
Uits, C„ 354
unconscious, defined, 31
uterus, 238
vagina, 238–39
vaginal sexuality, 243—45 vaginismus, 239, 261–62, 267–68 values, interests and, 220–26
van de Velde, Theodoor, 232–33
Van Dusen, R. A., 339, 340
variability hypothesis, 18
female sexuality and, 227–28, 254 Hollingworth’s challenge of, 86, 87–88 intellect and, 205
vasectomy, 275, 277, 279 vasocongestion, pelvic, 241—43 verbal ability, 147, 155
Vernon, P. E„ 220–22
Vicinus, M., 398—99 victimization of women, 425–26, 444—45, 474
see also battering; rape, forcible; sexual harassment
Victorianism;
sexual views of, 230—31
Thompson, 79
“true womanhood” and, 10–12
Vida, G., 401
Vienna Psychoanalytic Society, 81
virginity:
property rights and, 229
Victorian view of, 10—11
Vogel, I., 196
Voth, H. M„ 467, 468
Waber, D. P„ 153
Wachtel, S. S., 100
Wade, M. E., 274
Wakefield, W. M„ 189
Walberg, H.J., 222, 223
Walden II (Skinner), 354—55
Waldron, I., 129
Waldrop, M. F., 159
Walker, A., 220
Walker, Alice, 174, 378, 383
Walker, L. E„ 432, 434, 438–39
Wallston, B. S„ 510
Walters, R. G„ 5
Ward, D. A., 419
Ward, I. L„ 110
Ward, W. D„ 183
Warrington, E. K., 151
Watson, John B., 92
Webster, B. S„ 56
Weideger, P., 199
Weinberg, M. S., 410
Weingarten, K., 374
Weinraub, M., 191, 192
Weinzweig, M., 14, 15
Weir, James, Jr., 11
Weisheit, R. A., 418
Weisskopf, M„ 301,302–3, 304, 325, 326
Weissman, H. J., 212
Weitzman, L. j., 195
Welch, M. R., 194
Well of Loneliness, The (Hall), 399–400
Welter, B., 10
Wenger, M. G., 229
Wertz, D. C., 312, 313, 320
Wertz, R. W., 312, 313, 320
Westoff, C. F„ 286, 288
Westoff, L. A., 286
White, W. C., 454
Whiting, A. W. M., 169
Whiting, B. B., 166
Whitman, Walt, 217
Whittack, F. A., 328
Wideman, M. V., 318–19
widowhood:
Angelina’s story of, 498—99
black women and, 495—96
sex ratios in, 493, 494
social relations and, 494—97
wife-beating, see battering
Wilkie, F„ 478
Williams,}. H., 185, 190
Williams, L. R., 200
Williams, V. L., 423
Williamson, N. E., 187
Wilson, E. O„ 110, 131–32, 369
Winick, C., 207
witches, 4—5
Wolfe, L., 252, 408
Wolff, P. H., 151
Wolffian ducts, 102—3, 104, 106
Women on Words and Images, 197
women’s movement:
black women and, 378
consciousness raising and, 472
female crime and, 421
see also feminists
Wood, C., 269, 270, 280, 281
Wooley, Helen Thompson, 134
Woolf, Virginia, 205–6, 399–400, 401
Wordsworth, William, 397
working women:
children and, 371–72, 373–74, 375
marriage and, 338, 360, 367—68, 371—77
mental disorders and, 480, 483
motivations of, 367—70
sexual harassment of, 439—40
single life and, 361—62
Thompson on, 80
see also career
Wright, C. T., 464
Wylie, Elinor, 476
Wylie, Philip, 59
Yarden, P. E., 321
Yorke, P. C., 205
Young, W. C., Ill, 168
Yurok society, 61, 65
Zawadski, E. S., 291
Zelnick, M., 249
Ziegler, F. J., 277
Zita, J. N., 391, 392
Zuckerman, M., 327
Zunich, M., 159
[Back Cover]
PSYCHOLOGY OF WOMEN
Behavior in a Biosocial Context
Third Edition
JUANITA H. WILLIAMS
This is the new third edition of a text that has been the standard for women’s studies courses since its original publication. Retaining its contemporary life-span approach to the female experience, the third edition of Psychology of Women offers a much more research-based presentation informed by numerous case studies and cross-cultural experiences.
New to this edition: a full chapter on lesbianism and a major section on the black female experience; inclusion of biological topics like premenstrual syndrome, why women live longer, sociobiology and Alice Rossi’s biosocial perspective; updated sections on gender differences, especially spatial and mathematical abilities; Carol Gilligan’s theory on women’s moral development; new material on teenage sexuality; expanded treatment of the abortion controversy; China’s one-child policy and its effect on women and birth control; new material on women and careers, “dream versus drift,” and the “having it all”/male role at home conflict; expanded discussion of wife battering and a full new section on pornography; incorporation of DSM III, with new material on female suicide and feminist therapy; and all presented against a historical backdrop that now includes Freud’s seduction theory controversy, the work of the early twentieth-century experimental psychologist Leta Hollingworth, as well as early philosophers’ views on women.
In short, Psychology of Women remains the most complete and accessible text; its third edition keeps pace with the most recent research in the field.
Accompanying Reader
Psychology of Women: Selected Readings, Second Edition, has been specifically designed to accompany Professor Williams’s textbook. It includes thirty-nine multidisciplinary articles on the biological, social, psychological, and personal stages of women’s life cycle.
The Author Juanita H. Williams is professor emeritus of psychology and women’s studies at the University of South Florida.
COVER ART. ANDREA AS PERSEPHONE. BY JACQUELINE MORREAU
COVER DESIGN BY MIKE McIVER
Norton
W • W • NORTON & COMPANY NEW YORK • LONDON
[1] The only women who actually had anything to gain from this perception were the affluent classes who could indulge in it. Obviously it did not apply to black women, immigrant women, women working in factories. The flights of rhetoric which made woman an exalted being were meant to pay tribute to white Anglo-Saxon wives of prosperous planters and business and professional men.
[2] The twentieth-century Irish dramatist George Bernard Shaw pointed out the darker consequences for women of being perceived as angels: “It is all very well to be regarded as an angel up to a certain point; but there come moments at which you are seriously inconvenienced by the fact that you are not an angel; that you very seriously require certain accommodations and conveniences which angels can do without; and that when these are denied to you on the ground that you are an angel, you suffer for it” (Adams and Briscoe, 1971, p. 197).
[3] All was not Utopian for women in the Republic. Plato talks of a community of wives, but not of a community of husbands. Also, while he elevated women to a higher status than they ever had in reality in classical Greece, he believed that in general the talents and abilities of women were inferior to those of men.
[4] In the meantime, Anna had fallen in love with Breuer, a turn of events which upset the proper physician greatly. When he attempted to terminate treatment she immediately relapsed and presented him with her most dramatic symptom, a hallucination that she was in labor with his child. Breuer hastily left with his wife on a vacation, and never again could he bring himself to use the “talking cure” on a patient. Anna eventually regained her health and became prominent as the first social worker in Germany. A major part of her life’s work was spent on women’s causes and emancipation. In 1922, she wrote, “If there is any justice in the next life women will make the laws there and men will bear the children” (Jones, 1953, p. 224).
[5] Narcissism derives its name from the name of the mythological Greek youth Narcissus, who fell in love with his own image reflected in a pool of water.
[6] For example, see Strouse (1974) and Miller (1973).
[7] Definitions are for the positive aspect of these polarities and are the author’s distillation of Erikson’s descriptions. For full discussion of the meaning of both poles, see Erikson (1963), pp. 247–74.
[8] For example, see Janeway (1971), Chesler (1972), and Doherty (1973).
[9] For the relationship between theory and anomaly, see Kuhn (1970).
[10] Funk & Wagnails Standard College Dictionary (New York: Funk & Wagnails, 1968).
[11] In Kelman (1967), p. 167.
[12] It should be remembered that at this time the United States was on the eve of entry into World War I and there was a great deal of concern about military conscription, national aggrandizement through colonization, and patriotism, manifested in men by willingness to fight for their country and in women by the bearing of children, especially sons, to support the national effort. Large families were encouraged to support all these values.
[13] The same may be said of other categorical variables, such as race or age.
[14] In this and subsequent discussions, sex will refer to the biological identity of the person as male or female. By contrast, gender will refer to culturally defined and imposed female-male differences, as in roles, dress, certain personality characteristics, and so on.
[15] Since the male has only one X chromosome, if he inherits genes for a pathological condition that are carried on the X, he will manifest the condition since, in the absence of a second X, there is no normal dominant allele to override it.
[16] The neonatal period is usually defined as the first month of life and is part of infancy, the first year or two of life. These terms are loosely used to designate newborn infants and babies who have not acquired language.
[17] Skeletal maturation or bone age is the most useful measure of physical maturity (Tanner, 1978).
[18] Examples are hemophilia, the “bleeder’s disease,” and red-green color blindness.
[19] The Apgar score refers to a group of physiological signs that indicates the infant’s condition at birth
[20] Some publishers of children’s books are making an effort to avoid sexism and to depict girls and women (as well as boys and men) in more nontraditional roles. Even so, a review of the field concluded that the problem still exists (Weitzman, 1979).
[21] [Footnote missing]
[22] It has been suggested both facetiously and seriously that one reason for the dearth of females among the achievers is that women don’t have wives. Edwin H. Land, inventor of the Polaroid camera, said in an interview (Bello, 1959) that he found it important to work intensively for long hours when he was approaching a solution to a difficult problem. “You are handling so many variables at a barely conscious level that you can’t afford to be interrupted. If you are, it may take a year to cover the same ground you could otherwise cover in sixty hours.” For most married women, life is a history of interruptions. One of my older students told me that on weekends when everyone was at home, whatever she was doing was the least important of all the ongoing activities—she was the most interruptible. Even the dog knew it!
[23] The score ranges on the ordinates of Figures 6.4 and 6.5 are different because a revised form on the instrument was used for the latter study.
[24] For analyses of sexuality in relation to culture, see Katchadourian and Lunde (1975), Marshall and Suggs (1971), and Ford and Beach (1951).
[25] Quoted in Brecher (1979), pp. 48—49.
[26] The number of blacks interviewed was too small for statistical analysis (Katchadourian and Lunde, 1975).
[27] Hymen was the Greek God of marriage, son of Dionysus and Aphrodite.
[28] The length of the male’s refractory period during which renewal of response is impossible varies with age, length of time since last intercourse, alcohol consumption, and other variables. The capacity for a quick succession of erections and orgasms in the male is usually lost after thirty.
[29] For a highly detailed and technical account of female eroticism and response and the mechanisms underlying them, see Sherfey (1972).
[30] The male sample was already close to its maximum in .the youngest group, the fifteen- to twenty-year-olds.
[31] In 1982, at a Barnard College conference on sexuality, antipornography feminists picketed and called for a boycott on speakers whose “pro-sex” views they judged to be nonfeminist (Freedman and Thorne, 1984).
[32] For exceptions related to physical causes, see Kaplan (1974).
[33] One hundred woman-years means one hundred fertile, sexually active women using the method for one year.
[34] Cowper’s glands are the male counterpart to the Bartholin’s glands of the female.
[35] It should be noted, however, that while abortion is an alternative for a pregnant woman, it is not recommended as a method of birth control. For instance, the aim of an organization such as Planned Parenthood is educating the public about preventive methods of birth control.
[36] This amendment to the Labor and Health, Education, and Welfare appropriations bill has been adopted each year since 1976 (Hayler, 1979).
[37] It is important to note that the study participants are identified activists in the abortion controversy. Their characteristics and beliefs are not necessarily those of others who share their views on abortion.
[38] The sex ratio is defined as the ratio of male to female births, times 100.
[39] The length of a pregnancy sometimes has legal implications if a child is born when the husband has been away more than nine months. The longest pregnancy upheld as legitimate in this country was 355 days (Katchadourian and Lunde, 1975).
[40] Tay-Sachs’ is a fatal hereditary blood disease found almost exclusively among Jewish people.
[41] Today, women who major in home economics are preparing for a career. I have never heard of anyone taking such a course in preparation for the role of housewife.
[42] St. Petersburg Times (Florida), December 8, 1974.
[43] U.S. Census Bureau report, “Households, Families, Marital Status and Living Arrangements, 1985.”
[44] Dr. Laura Singer, formerly president of the American Association of Marriage and Family Counselors, was speaking of traditional marriage when she said, “1 wouldn’t say that marriage and self-actualization are necessarily mutually exclusive, but they are difficult to reconcile” (Lear, 1972).
[45] Women’s Bureau, U.S. Department of Labor.
[46] This is true of other ethnic minority women too, such as Native American, Hispanic, and Asian women. Research specifically focusing on these groups is so sparse, however, that few generalizations are possible. For excellent cross-cultural and ethnic studies of women, see Signs: Journal of Women in Culture and Society, vol. 1, 1975, to the present.
[47] Catharine Stimpson (1981) noted that the first citation for lesbianism as a female passion in The Shorter Oxford English Dictionary is 1908, while sapphism appeared in 1890. Sapphism, of course, is derived from the name of Sappho (see p. 393).
[48] This relative lack of attention by the law persisted for centuries. When the Criminal Law Amendment was passed in England during Victoria’s reign, prohibiting homosexual acts between adults, the queen refused to sign the act until all references to women were removed. It was her firm belief that lesbianism did not exist; consequently, lesbianism was never illegal in England as it has been elsewhere.
[49] It was for this reason that the romantic friendships between women of the eighteenth and nineteenth centuries could flourish unchallenged. As long as they were thought to be nonsexual in actual behavior regardless of the sensual and erotic meanings they often had for many, they did not threaten the heterosexual model and thus could be tolerated as benign.
[50] As we saw in Chapter 5, this is not as fateful and sinister as it sounds. The role of the biological determinant is very limited indeed compared to the greater potency of experientially determined behavior shaping. Although the participants in socially sanctioned forms of aggression such as sports and war are overwhelmingly male, many individual males and even whole tribes such as the Tasaday of the Philippines are quite unaggressive. The Tasaday, in fact, have no weapons and no word for war (MacLeish and Launois, 1972).
[51] Uniform Crime Reports, Bureau of Investigation, 1968, 1979, 1984.
[52] For detailed discussion of definitions of rape, see Katz and Mazur, 1979.
[53] For Uniform Crime Reporting purposes the victims of forcible rape are always female.
[54] By a 1977 ruling of the U.S. Court of Appeals in Washington, D.C.
[55] Many colleges and universities have adapted the EEOC guidelines on sexual harassment in work settings to the academic environment (Crocker, 1983).
[56] From The Random House Dictionary of the English Language, College Edition, New York: Random House, 1969.
[57] Washington, D.C.: Government Printing Office, September 1970.
[58] Time, August 10, 1970, p. 13.
[59] For a detailed discussion of the climacterium see Chapters 4 and 13.
[60] Psychoactive drugs affect mental and emotional states as contrasted to physical or organic conditions.
[61] For historical accounts of women and psychotherapy, see Franks and Burtle (1974), Greenspan (1983), and Hare-Mustin (1983).
[62] An exaggeration of this phenomenon is commonly observed in the reactions of the general public to persons who are in the vanguard of social movements. A good example of this tendency is the readiness to label supporters of women’s liberation lesbians. A woman who questions or violates normative female behavior is thus seen as deviant, which “explains” her lack of interest in or hostility toward society’s definition of her role.
[63] Copyright 1932 by Alfred A. Knopf, Inc. Renewed 1960 by Edwina C. Rubenstein. Reprinted by permission of the publisher.
[64] Seriousness of problems is not the only determinant of seeking help. Attitudes toward symptoms, finances, availability of care, educational level, and personality are also important. For example, one woman might have a very stoic attitude, believing that she must “live with” problems she sees as inevitable; another with the same kind and degree of symptoms might be less willing to endure or be more knowledgeable of kinds of help available.
[65] Copyright © 1969 by Random House, Inc. Reprinted with permission of the publisher.
[66] A review of such material cited the observation that there are no “old bachelor” jokes and that the jokes about women are more often negative (77 percent) than are those about men (51 percent) (Puner, 1974).
{1} The Epigenetic Chart is reprinted from Childhood and Society, Second Edition, Revised, by Erik H. Erikson, with the permission of W. W. Norton & Company, Inc. Copyright 1950, © 1963 by W. W. Norton & Company, Inc.
{2} From Heredity, Evolution, and Society, 2nd ed., by 1. Michael Lerner and William J. l.ibbv. W. H. Freeman and Company. Copyright © 1976.
{3} Source: Institutional Research Report, University of South Florida, 1985.
{4} Source: The Tampa Tribune, October 17, 1985. schools where their numbers make them highly visible, women faculty exemplify female achievement, serving as important role models for their students (Tidball, 1980).
{5} Adapted from Beach, F. A., ed.. Sex and Behavior, New York, John Wiley and Sons, 1965, by permission of editor.
{6} Adapted from Beach, F. A., ed., Sex and Behavior, New York, John Wifey and Sons, 1965, by permission of editor.
{7} Copyright © 1973, 1974 by Morton Hunt.
{8} Copyright © 1973, 1974 by Morton Hunt.
{9} From data in Irwin J. Knopf, Childhood Psychopathology, Englewood Cliffs, N.J.: Prentice-Hall, 1984.
{10} Range of ratios reported in various studies.
{11} Ibid.
{12} Ibid.
{13} Adapted from Uniform Crime Reports, Federal Bureau of Investigation, 1979, 1984
{14} Adapted from The Diagnostic and Statistical Manual, American Psychiatric Association, 1980.