Ted Kaczynski's Autopsy Report
North Carolina Department of Health and Human Services
Office of the Chief Medical Examiner
3025 Mail Service Center Raleigh, NC 27699-3025
Telephone 919-743-9000
Fax 919-743-9099
REPORT OF AUTOPSY EXAMINATION
Decedent
Document Identifier B202303444
Autopsy Type ME Autopsy
Name Theodore John Kaczynski
Age 81 yrs
Race White
Sex M
Authorization
Authorized By Christina M. Stafford RN
Received From Durham
Environment
Date of Exam 06/12/2023
Autopsy Facility Office of the Chief Medical Examiner
Time of Exam 09:35
Persons Present Mr. Ian Kang (Autopsy Technician); Derek Upperman and Tariq Conyers (Federal Bureau of Prisons)
Certification
Cause of Death
HANGING
The facts stated herein are correct to the best of my knowledge and belief.
Digitally signed by
Paul Yell MD 11 April 2024 16:06
Diagnoses
I. Hanging
-
Abraded, thin ligature furrow with upward canting, lowest point just below the thyroid cartilage
-
Reportedly used a shoelace ligature
-
Petechiae of the bilateral lower eyelids and upper lip
-
Left strap muscle and thyroid hemorrhages
-
Early ischemic changes in the hippocampus
-
-
Resuscitative efforts
-
Overlapping anterior chest contusions with numerous associated rib fractures and a transverse sternal fracture
-
Multifocal liver lacerations with associated hemoperitoneum (3000 mL), skin pallor
-
-
Anasarca
-
Pitting edema, moderate, lower legs
-
Scrotal edema, severe
-
Pleural effusions, bilateral, mild, serosanguinous
-
-
II. Metastatic rectal carcinoma
-
Primary site in the rectum (5.0 cm)
-
Innumerable, large metastases to bilateral lungs and liver
III. Hypertensive and atherosclerotic cardiovascular disease
-
Globoid heart (410 g) with right ventricular dilation
-
Coronary artery disease, mild
-
Left ventricular subendocardial calcification
-
Mitral and tricuspid valve redundancy/ballooning
-
Aortic atherosclerosis, moderate, with a dilated root
-
Hypertensive arterionephrosclerosis, moderate
IV. Benign prostatic hypertrophy
-
Increased bladder trabeculations, with no mucosal erythema
-
Mild, non-specific chronic inflammation submucosally on histology
-
V. Small intestinal serosal calcified nodule (<0.5 cm)
VI. Blunt trauma
-
Abrasion of left ankle
Identification
Body Identified By
Papers/ID Tag
EXTERNAL DESCRIPTION
Length 68.5 inches
Weight 158 pounds
Body Condition Intact
The body is received in a zipped body bag, sealed with a tamper-evident lock #0083146. There are matching identification tags present on the outside of the bag and on the decedent.
CLOTHES AND POSSESSIONS: None.
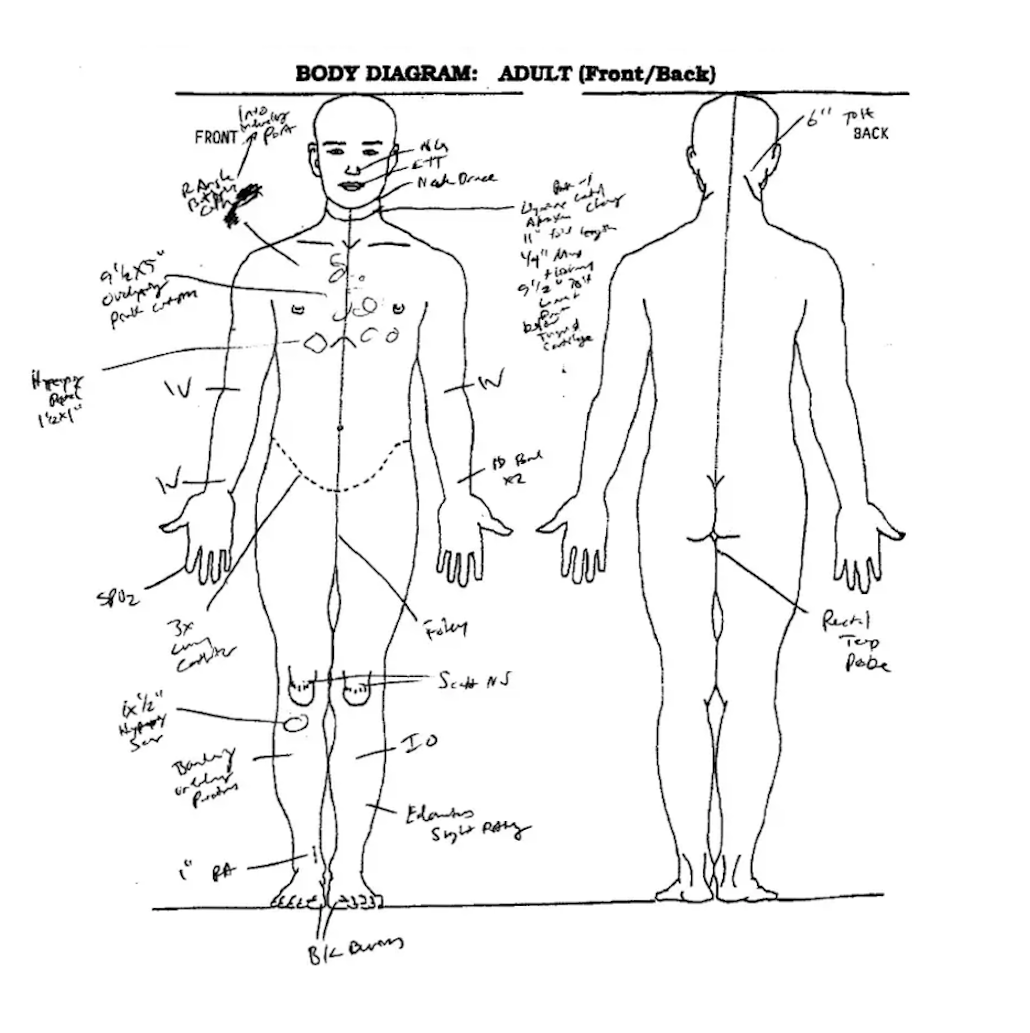
EVIDENCE OF MEDICAL THERAPY:
-
Nasogastric tube
-
Endotracheal tube
-
Cervical collar
-
Right angle butterfly catheter of the right upper chest
-
Intravenous catheters of the bilateral antecubital fossae (one each)
-
Intravenous catheter of the right volar wrist
-
Pulse oximetry sensor of the right 2nd finger
-
Triple-lumen catheter of the right inguinal crease
-
Foley catheter
-
Hospital identification bands x2 on the left wrist
-
Intraosseous catheter of the left tibia
-
Gauze bandage of the right anterior lower leg with some faint blood staining and a few underlying puncture wounds (likely failed intraosseous access attempts)
-
Rectal temperature probe
The body is that of a normally developed, well-nourished, light-complexioned man appearing consistent with the listed age. The length is 68 1/2" and the weight is 158 lbs, as received. The body is cool, well-preserved, and has not been embalmed. The skin is overall very pale. Rigidity is moderately developed in the large and small muscle groups. Lividity is very faint pink, fixed, and in a posterior distribution.
The scalp is covered with brown-gray, wavy hair measuring up to 2" on the top of the head. There is also facial hair in a beard and mustache distribution which is up to 2" in length. The ears are normally formed and without drainage. No piercings are apparent. The irides are blue, the corneas slightly cloudy, and the sclerae are white with a yellow tinge. The bulbar conjunctivae are free of petechiae, however the palpebral conjunctivae particularly on the inferior surfaces do have a few scattered subtle petechiae. The nose is intact and the nares unobstructed. The lips are normally formed. There are some faint petechiae on the inner surface of the upper lip and some injuries on the inner surface of the lower lip which appear related to endotracheal tube insertion. The anterior teeth are natural and in poor condition, with many irregularly absent on the upper jaw. The superior and inferior frenula are intact. The neck is normally formed and symmetrical, and has evidence of injury which will be described below.
The chest is normally formed, symmetrical, and without palpable masses other than an indwelling port at the right upper chest. The abdomen is protuberant and has a fluid wave. There are no palpable masses. The external genitalia are those of an adult man, and the scrotum is edematous. The back is straight and symmetrical. The anus is atraumatic.
The arms are normally formed and appear slightly atrophic. No needle punctures other than those from medical intervention, nor any track marks or ventral wrist scars are seen. The fingernails are trimmed short. The legs are normally formed and have moderate pitting edema. There are no lower extremity amputations or deformities. The toenails are trimmed short and there are bunions of both halluces.
BODY MARKINGS: On the right lower chest is a hyperpigmented patch which is 1 1/2 x 1" and oval. On the bilateral anterior knees are scattered, nonspecific scars. Just below the right knee is a hyperpigmented, elevated patch which is 1 x 1 1/2" and oval.
Injuries
HANGING:
Primarily on the anterior neck is a ligature furrow which is abraded and pink with central tan clearing. There are upward canting ends posteriorly. The overall furrow length is 11", with a maximum width of 1/4" at the anterior-most point. The anterior-most point is 9 1/2" below the top of the head and just below the thyroid cartilage. The highest point of the furrow is at the right posterolateral neck and is 6 below the top of the head. There are associated petechiae of the upper lip and bilateral eyelids as described above. Layered anterior neck dissection reveals strap muscle hemorrhages of the left omohyoid and left sternothyroid muscles, as well as minor hemorrhage on the surface of the left thyroid gland. There were no cervical vertebral injuries. There were also no vascular injuries.
RESUSCITATION-RELATED TRAUMA:
On the anterior chest towards the left and in the center is a 9 1/2 x 5" cluster of overlapping pink contusions consistent with CPR. Underlying this are numerous rib fractures with surrounding fresh hemorrhage affecting the left lst-8th and right lst-6th ribs anteriorly with an accompanying transverse sternal fracture. The underlying liver is severely affected by numerous metastases and has two large lacerations on the right lobe anteriorly which measure 6.0 and 3.0 cm respectively, as well as a posterior liver laceration near the hilum which is 2.5 cm. There is associated massive hemoperitoneum which measures 3000 mL.
BLUNT TRAUMA:
On the medial left ankle is a 1", linear, vertically oriented, red abrasion.
Disposition of Personal Effects and Evidence
The following items are released with the body None.
The following items are preserved as evidence
A pulled scalp hair sample and a blood card are retained as evidence. There are no other items to release.
Procedures
Radiographs
Full-body, postmortem radiographs are performed.
Internal Examination
Body Cavities
All injuries are described above and will not be further characterized in the Internal Exam Section.
The abdominal fat layer measures up to 1.0 cm in thickness. The body cavities have extensive hemorrhage in the peritoneum as described above, as well as smaller amounts of serosanguinous fluid in the right and left pleural spaces. The serosal surfaces are smooth, glistening, and without adhesions. The organs are normally located. The diaphragm is intact.
Cardiovascular System
Heart Weight 410 grams
The heart has a globoid shape with a smooth, glistening epicardium. The coronary arteries have a normal origin and distribution with right dominance. The proximal portion of the left anterior descending coronary artery has up to 20% atherosclerotic stenosis. The proximal portion of the right coronary artery has up to 30% atherosclerotic stenosis.
The myocardium is red-brown, firm, and uniform without focal fibrosis, softening, or hyperemia. There is a small amount of calcification in the subendocardial area of the left ventricle. The right ventricle is moderately dilated. The thicknesses of the right ventricle, left ventricle, and interventricular septum are 0.3 cm, 1.3 cm, and 1.6 cm, respectively.
The endocardium is intact, smooth, and glistening. The cardiac valve leaflets are of normal number, pliable, intact, and free of vegetations, however the leaflets of the mitral and tricuspid valves appear redundant/ballooned. The atrial and ventricular septa are free of defects.
The aorta has a dilated root and moderate atherosclerotic changes. There are no vascular anomalies or aneurysms. The vena cavae and pulmonary arteries are without thrombus or embolus.
Respiratory System
Right Lung Weight 810 grams
Left Lung Weight 790 grams
The tongue is free of hemorrhage. The strap muscles and other anterior neck soft tissues are injured as described above. The hyoid bone and cartilaginous structures of the larynx and trachea are normally formed and without fracture. The airway is unobstructed, contains no foreign material, and is lined by smooth, pink mucosa. The prevertebral soft tissues are free of hemorrhage. The cervical vertebrae have no displacement, hypermobility, or crepitus.
The lungs have the usual lobation, but are massively distorted by metastatic carcinoma. The pleurae are mostly smooth and glistening, however there are puckered areas underlying the metastases. The lungs have moderate anthracotic pigment. The background of the lungs is well expanded and crepitant, however the right lung is 30% replaced by metastasis, and the left lung is 50% replaced by metastasis. The metastatic lesions are roughly round with a radial arrangement around central necrosis and are white and friable. The background parenchyma is dark red and exudes small amounts of fluid on sectioning. The lungs have no consolidation, hemorrhage, infarct, gross fibrosis, or enlargement of air spaces. The bronchi contain no foreign material and have smooth, pink mucosa.
Gastrointestinal System
The esophagus and gastroesophageal junction are unremarkable. The stomach contains approximately 20 mL of green masticated food, but no visible pills or pill residue. The gastric and duodenal mucosae are intact and unremarkable. The small intestine has a single focus of serosal calcification which is less than 0.5 cm. The large intestines and appendix are unremarkable to inspection and palpation. There is a mass in the rectum which is 5 x 4.5 x 1.0 cm and which has central ulceration and rolled and erythematous edges.
Liver
Liver Weight 3410 grams
The liver capsule is markedly distorted by numerous metastases and is injured as described above. Roughly 90% of the liver is replaced by tumor which is similar to that seen in the lungs. The residual parenchyma is red-brown and uniform without yellow discoloration or palpable fibrosis. The gallbladder contains approximately 5 mL of brown bile and no stones. The mucosa is uniform, and the wall is not thickened.
Spleen
Spleen Weight 150 grams
The intact capsule is smooth. The parenchyma is maroon, firm, and uniform.
Pancreas
The pancreas has the normal size, shape, and lobulated architecture. The parenchyma is tan and uniform.
Urinary
Right Kidney Weight 130 grams
Left Kidney Weight 140 grams
The kidneys have retained fetal lobations but otherwise normal shape and position. The cortical surfaces are moderately granular. The kidneys have the usual corticomedullary structure without tumors or cysts. The pelves and ureters are not dilated or thickened. The bladder contains no urine, however the attached Foley bag has 250 mL of orange, cloudy urine. The mucosa is mostly uniform but with increased trabeculations, and the wall is not hypertrophied. The mucosa has no erythema.
Reproductive
The prostate gland is moderately enlarged and nodular but still uniform in color.
Endocrine
The thyroid gland is not enlarged, and the lobes are symmetrical. The parenchyma is red-brown and uniform. The adrenal glands have the normal size and shape. The cortices are thin, uniform, and yellow, and there is no hemorrhage or tumor. The pituitary gland is not enlarged.
Neurologic
Brain Weight 1540 grams
The scalp is free of hemorrhage. The calvarium and base of the skull are normally configured and without fracture. There is no epidural or subdural hemorrhage. The dura is intact.
The leptomeninges are glistening and transparent without underlying hemorrhage, exudate, or cortical contusion. The cerebral hemispheres are symmetrical with a normally developed gyral pattern. There is no flattening of the gyri, narrowing of the sulci, or evidence of herniation. The arteries at the base of the brain have patchy, mild basilar atherosclerosis and no aneurysms.
Sections through the cerebral hemispheres show a normally developed cortical ribbon and uniform white matter. The basal ganglia, thalami, hippocampi, and other internal structures are normally formed and without focal change. The ventricles are not enlarged, and the linings are smooth and glistening. Sections of the brainstem and cerebellum show normal structures without focal change.
Immunologic System
There is no enlargement of the lymph nodes of the neck, chest, or abdomen. The thymus is involuted.
Musculoskeletal System
The musculoskeletal system is well-developed and free of deformity, and there are injuries as described above. The ribs are not brittle. The skeletal muscle is dark red and firm.
Microscopic Examination
Microscopic Comment
Representative sections of organs and tissues are retained.
SECTION KEY:
-
Liver, left lung, right kidney
-
Left ventricle, right ventricle, right lung, and right lower lobe tumor
-
Hippocampus
-
Rectal tumor and bladder wall
Cardiovascular
Sections of both ventricles have no significant histopathologic changes.
Respiratory
The background lung parenchyma has scattered fat/marrow emboli likely related to cardiopulmonary resuscitation. Metastatic adenocarcinoma foci are frequent, and appear similar to the primary described below.
Liver
The background liver is markedly distorted by the nearby metastasis, with buckled/elongated hepatocellular plates, frequent hemorrhages, bile duct proliferation, and cholestasis. The nearby adenocarcinoma metastasis appears similar to the primary described below.
Genitourinary
The right kidney has typical parenchymal architecture and moderate atherosclerotic intimal thickening of arteriolar walls. A section of bladder has moderate submucosal chronic inflammation and reactive changes of stromal cells, which is nonspecific but could be seen with instrumentation such as a Foley catheter, or in some types of urinary tract infection.
Neurologic
A section of hippocampus has scattered acutely necrotic neurons, particularly in the CAI, subiculum, and entorhinal zones.
Gastrointestinal
A section of the rectal mass reveals a large, infiltrative adenocarcinoma made up of moderately differentiated glandular tissue with frequent mitoses and frequent dirty necrosis. Infiltration is present to the serosa.
Summary and Interpretation
According to reports, this 81-year-old man, Theodore Kaczynski, had been incarcerated since 1996 at Butner Federal Correctional Complex. He had a medical history of metastatic rectal carcinoma (diagnosed in March 2021 after complaints of rectal bleeding), as well as schizotypal disorder, avoidant personality disorder, and hyperlipidemia. In November of 2021, CT demonstrated pulmonary and hepatic metastases and he was transferred to the Butner Medical Center and housed in a solitary cell. Around 1 month prior to his death, he was noted to be depressed and sent for psychiatric evaluation. At around midnight on June 10, 2023, he was found to have hung himself from a handicap rail in his room with shoelaces. He was initially pulseless, and resuscitation was initiated. Return of spontaneous circulation was eventually achieved, and he was then transferred to the local emergency department with low blood pressure. Despite maximal efforts, he continued to decline and time of death was pronounced at 0807 hours. The decedent was not on any prescription medications and had no prior suicidal ideations or attempts. Federal Law Enforcement had no concern for foul play.
The autopsy documented a well-developed, elderly man who appeared pale and had edema of the lower extremities. Prominently, he had a thin, abraded ligature furrow of the neck which was upward canting. He also had petechiae of his eyes and upper lip. Internally, there was some minor hemorrhage of muscles and fascia on the left side of the neck, associated with the area where the furrow was. There was extensive injury to the rib cage from chest compressions, with underlying lacerations of the liver which resulted in massive hemoperitoneum (3000 mL). Brain examination revealed early signs of damage from low blood flow (ischemia). Otherwise, there was underlying metastatic rectal carcinoma with innumerable metastases to the liver and both lungs. These hypervascular and friable lesions may represent a diathesis for the liver lacerations and resultant intraabdominal bleeding. He also incidentally had a mildly enlarged and globoid heart with mild coronary artery disease, and some moderate hypertensive renal vascular disease.
While the immediate cause of Mr. Kaczynski's death was doubtless the massive blood loss which resulted from efforts to revive him (specifically, chest compressions causing lacerations of his severely diseased liver), said efforts would not have been necessary if not for his own inciting actions of hanging himself, and thus the manner is appropriately suicide. It is also probable that, even had he not suffered the large hemoperitoneum, he still would have eventually died as a result of ischemic brain damage from the initial hanging.
Based on the autopsy findings and circumstances surrounding the death, as currently understood, the cause of death is listed as hanging. The manner of death is classified as suicide.
Diagrams
1. Body Diagram: Adult (Front/Back)
State of North Carolina
Office of the Chief Medical Examiner
Examined By: PY
Date: 6/12/23